


You can make a difference.
The188bet手机appdepends almost entirely on your donations.
我們無法繼續與您捐贈的捐贈。
請commit at least a yearly $250 donation to the Atlas.如果沒有這一承諾,地圖集將很快要求支付認購事項,並且在世界各地的許多外科醫生都將無法進入其患者的護理依賴於它。
請donate now!
Last Updated: April 27, 2021
Figure 1: Harvey Cushing is the father of modern neurosurgery. His contributions paved the way for the establishment of the safety of brain tumor surgery in the face of critics.
Craniotomy techniques for brain tumor surgery have evolved immensely because of advances in imaging and microsurgical techniques. The development of flexible operative corridors, cortical and subcortical mapping, and magnetic resonance imaging (MRI) navigation have all enhanced the ability of the surgeon to resect tumors that were previously deemed inoperable.
通過這些技術進步,重點是簡單地減少死亡率,朝著最小化發病率,同時也實現了最大的切除,以便為患者提供最佳結果。
In this chapter, I review the general principles of brain tumor surgery. The specific tenets for resection for each pathology are covered in the dedicated tumor chapters.

Atlas選擇Bipolar Forceps (Coming in Feb, 2022)
專為您的每個手術機動設計
Five tip sizes for brain and spine procedures
Unparalleled non-stick and low-profile features
A careful history and physical examination are necessary to verify symptoms and correlate imaging findings.It is important to rule out non-neoplastic causes of mass lesions. Examples of these include infectious sources such as toxoplasmosis, vascular events such as evolving infarction, inflammatory factors such as sarcoidosis, and autoimmune causes such as multiple sclerosis.
這些病變可以模仿成像和呈現的腫瘤,並導致不必要的手術幹預,以可避免的風險放置患者。外科醫生應密切熟悉細微的臨床和成像結果,這些結果增加了對這些疾病在鑒別診斷中的懷疑。

圖2:這些圖像顯示病變th的例子at do not require resection as part of their treatment strategy. These images belong to three patients with multiple sclerosis. Note that the pattern of enhancement is faint in certain locations at the periphery of the lesion. The resultant extent of mass effect is minimal compared with the size of the lesion. Neoplasms frequently lead to more mass effect when they reach a large size.

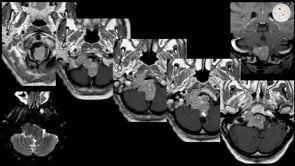
Figure 3: The images of the top row belong to a patient who suffered from a seizure. The MR enhanced images demonstrate gyral enhancement pattern compatible with acute infarction and not a neoplasm. The rest of the images in the subsequent rows belong to another patient with hemiparesis who was thought to have an insular tumor. A careful review of these images advances the suspicion of an infarct as the T2 hyperintensity crosses the striatum (left lower image); this feature is not consistent with tumorous masses that respect the medial gray matter structures. Diffusion imaging (right lower photo) confirms the findings of infarction and avoids unnecessary operative intervention.
有些腫瘤非常適合放療and do not require surgical resection.Germinomas., lymphomas, cerebral multiple myeloma and leukemia masses should be considered in the differential diagnosis of select neoplastic masses and nonresective diagnostic strategies such as CSF studies or stereotactic biopsy attempted.
損傷的多重性也破壞了積極切除的益處。
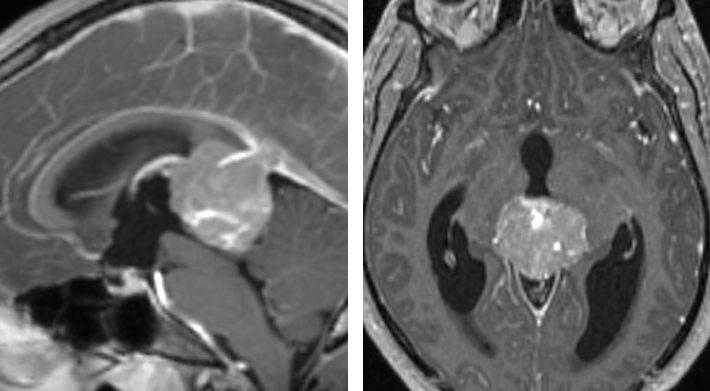
圖4:這位18歲男孩的MRI掃描展示了部分鈣化的鬆果質量。腦脊液標記物與診斷一致生殖器瘤。手術切除不需要。
Most patients who are considered for tumor resection present with a computed tomography (CT) or MRI scan showing a mass lesion. An MRI, with its superior soft-tissue resolution, discloses important details about the pathoanatomy of the lesion(s) and its signal characteristics on different MR sequences. These data define the size, location, proximity to eloquent brain structures, and boundaries of the mass. The pattern of contrast enhancement can be very informative for reaching an appropriate preoperative differential diagnosis.
如果存在骨骼或顱底基礎致力於確定骨腐蝕的模式,則可以需要CT掃描,從而為腫瘤的生長速率提供有價值的數據。CT血管造影和導管血管造影可以研究周圍的重要血管中的血管解剖和血液動力學參數。腫瘤栓塞可以用一些腫瘤救生,如glomus jugulare,hemangiopericytoma, and solidhemangioblastomaof the posterior fossa, when immediate tumor devascularization may not be feasible intraoperatively.
在評估相關的成像研究時,主要考慮是達到結論,繼續進行切除/活檢與其他治療方式(化療或輻射)或觀察和隨訪。如果質量的邊界定義不足,則涉及雄性的皮質/纖維或重要的神經血管結構,或者質量是多中心的,可能是不可能的總切除術或向患者提供次優益處。在這些情況下,應考慮其他治療方式。
If the diagnosis is not reliably possible from imaging and other available data and nonresectable lesions are strongly considered in the differential diagnosis, the surgeon should pursue a stereotactic biopsy to direct the final treatment plan.
Before proceeding with operative intervention, other investigations may need to be performed depending on the patient’s other medical conditions and age. Patients who are older than 40 should obtain a preoperative chest x-ray, and patients who are older than 60 should have an electrocardiogram.
所有患者應具有完整的血統計數,包括血小板計數,以及基本代謝板。如果有需要圍手術期輸血的合理可能性,它們應該是“打字和交叉”。患有已知瘀傷的患者,出血性疾病或正在服用其他醫療病症的抗凝血劑的患者也應該接受凝血酶原時間(PT),部分血栓形成時間(PTT),以及患者曆史所示的其他凝血試驗。許多具有轉移潛力的已知或疑似惡性腫瘤的患者需要最近的胸腔/腹部/骨盆掃描,並且可能是骨掃描。高度建議的神經腫瘤谘詢。對於不到6個月的壽命不到6個月的壽命患者的患者侵略性手術策略通常不合理。
Perioperative medications may be necessary for seizure prophylaxis or reducing vasogenic edema. Many patients present with seizures or are at high risk for postoperative seizures due to the location of their tumor (temporal lobe) and the extent of cortical dissection needed to remove the tumor. Keppra (levetiracetam) 20 mg/kg intravenous loading dose followed by 500-1000 mg q12 hours dosing is commonly prescribed for seizure prophylaxis.
不推薦使用類固醇的常規使用類固醇,但是可以用地塞米鬆10mg靜脈注射劑量降低顯著的促血管性水腫,然後進行4mg Q6小時的維持劑量,以準備手術。
There are four major anesthetic concerns for the intraoperative management of intracranial masses: 1) cerebral perfusion pressure, 2) brain relaxation, 3) ”smooth” anesthesia, and 3) efficient transition to the postoperative period.
During the induction phase of anesthesia, reductions in the metabolic oxygen rate and intracranial pressure (ICP) are greatly beneficial; barbiturates may be used. After administration of a nondepolarizing muscle relaxant, narcotics may be given without the risk of increased ICP from chest rigidity.
在誘導之前,通常給予地塞米鬆(10mg),以潛在地有助於腦鬆弛。施用抗生素,例如Cefazolin(1g)用於感染預防。所有患者應佩戴序列壓縮襪,收到Foley導管。可以在選擇患者中插入腰部排水管,以促進腦鬆弛。
用揮發性劑,優選異氟烷,小劑量的毒物和肌肉鬆弛劑,最佳地獲得麻醉。異氟醚還會降低氧氣的氧代型代謝率。注意,已知異氟烷略微增加ICP。
In maintaining hemodynamic stability and cerebral perfusion pressure, only iso-osmolar fluids are administered to best preserve neuronal homeostasis. Fluids containing glucose should be avoided because hyperglycemia has been shown to negatively affect outcomes in patients with ischemic cerebral injury.
定位的總體目標是在優化曝光時保持患者的安全性和舒適度。Mayfield夾具牢固地固定在患者的頭部,用固定點盡可能遠離切口。It is important to be aware of any shunt catheters or burrholes when pinning to avoid puncturing the shunt or penetrating the burrhole, respectively.
Previous craniotomy sites are left unpinned to avoid sinking of the bone flap. Untraditional skull clamp placement in these situations should protect the patient’s eyes and ears. Slippage of the pin into the globe has been reported after the pin was placed too close to the orbital rim.
The vertical arms of the clamp should be perpendicular to the floor and the patient’s head rotated less than 45 degrees while the patient is in the supine position. A lateral or park-bench position is preferred for posterior scalp exposure.
Pillows and pads should be generously used to pad all the patient’s pressure points, preventing peripheral nerve injuries. The patient should be well secured to the operating room table, especially if the patient is obese and changes in patient positioning (tilting) are expected during the procedure to adjust the intradural working angles of the surgeon.
All of the intravenous lines and the lumbar drain catheter are rechecked to ensure their patency after finalizing the patient’s position and before prepping the skin. Shaving should be kept to a minimum and the planned incision should be marked on the scalp after confirming the tumor location with MRI navigation.
Accuracy of the navigation should be confirmed using standard landmarks: external auditory meatus, lateral and media canthus, and the nasion. Navigation can be misleading for lesions situated on the curvature of the skull; coronal, axial, and sagittal images should be used for accurate mapping of the tumor’s location.The location of the tumor, as guided by navigation, is confirmed with respect to surface landmarks (i.e., external auditory meatus and coronal suture, etc.).
The nuances of technique for complication avoidance and management during craniotomy and exposure are discussed in theCranial Approachesvolume. During a craniotomy near the dural venous sinuses, I place two burr holes over the dural sinus, saving the bony cut near the sinus for last.
應進行徹底的灌溉,以確保在打開硬腦膜之前除去所有骨碎片和灰塵。當切割後窩硬窩時,保持足夠的距離骨頭邊緣的距離,以允許足夠的多雲套筒進行防水多雲閉合。
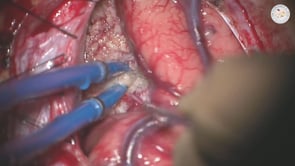
After the dura is reflected, visual inspection of the tumor’s extension to the cortical surface is performed; image guidance or ultrasound may be used if necessary. The surgeon should use multiple anatomic landmarks to confirm navigation data before removing relatively normal-appearing tissue.
依賴於應避免多雲開口後易於錯誤的一個導航源(CT或MRI計算機化導航),這是易於誤差的誤差。大表麵皮質靜脈和動脈,常規靜脈/陀螺儀表麵上腫瘤的界限,以及術前成像的其他識別標誌物應用於在整個解剖和切除過程中補充外科療法。
Details of cortical mapping are discussed in theLanguage MappingandSensorimotor Mappingfor glioma chapters. In general, anen bloc如果腫瘤boundari腫瘤切除是首選es or pseudocapsule are relatively distinguishable from the normal brain parenchyma and if there is enough operative space available to achieve this goal without retracting on the normal structures.
The specific techniques for a given tumor are discussed in the individual chapters in this volume. After resection is complete, the surgeon must pay careful attention to achieve hemostasis using bipolar coagulation. I use thrombin solution irrigation for slow venous ooze along the walls of the resection cavity.
I do not cover or line the resection cavity with hemostatic materials because delayed scarring of these materials may lead to their enchantment on postoperative MRIs and confusion regarding tumor recurrence. In addition, these hemostatic materials can convey a false sense of security regarding the level of hemostasis achieved.
應避免靜態凝固周圍的正常吉爾。持續出血通常是因為殘留的腫瘤,並且可能需要進一步檢查和切除。雖然後窩手術後需要水密硬盤閉合,但我並不堅持為SuprateLential Craniotomies進行這種關閉。
一旦患者喚醒,手術室在手術室後立即進行神經係統檢查。如果患者難以引起或者如果存在意想不到的焦點缺陷,則應獲得CT掃描。
Patients can start with ice chips and small sips of water and advance their diet as tolerated. Hourly neurologic checks and vital signs should be performed throughout the first night for select patient who may deteriorate. Many patients can be observed with neurologic evaluations every 2-4 hours.
Typically patients can be transferred out of the intensive care unit or intermediate care unit to the regular ward on the first postoperative day. Antibiotics should be discontinued after 24 hours unless otherwise indicated, and steroids should be continued at a dose of 4mg every 6 hours.
The decision to terminate the use of steroids should be individualized, and patients may be weaned off over 1 to 2 weeks starting on the 4th or 5th postoperative day. Prophylactic anticonvulsant medications are also terminated one week after surgery if the patient has never suffered from a seizure.
An MRI should be obtained within 48 hours of surgery to assess for residual tumor. Physical and occupational therapy should be consulted to aid with any speech, motor, or sensory deficits. Patients may be safely discharged ~3 days after their craniotomy.
Apuzzo ML, Chandrasoma PT, Cohen D, Zee CS, Zelman V. Computed imaging stereotaxy: Experience and perspective related to 500 procedures applied to brain masses.Neurosurgery。1987;20:930-937.
Sawaya R.腦腫瘤手術的一般原則,Laligam N,Sekhar RGF(EDS):Atlas of Neurosurgical Techniques: Brain,第一red。紐約:Thieme Medical Publishers,2006,PP 411-421
Sawaya R, Rambo WM Jr., Hammoud MA, Ligon BL. Advances in surgery for brain tumors.Neurol Clin.1995;13:757-771.
Tommasino C. Fluids and the neurosurgical patient.Anesthesiol Clin N Am.2002;20:329-346, vi.
Warner DS, Boehland LA. Effects of iso-osmolal intravenous fluid therapy on post-ischemic brain water content in the rat.Anesthesiology.1998;68:86-91.
請loginto post a comment.
Be sure to follow us on social media for exciting content and stay updated onLIVEsessions with Dr. Cohen, questions on surgical technique, and more!



You must be logged in to view this material.

Sign up nowto access the most comprehensive collection of advanced microneurosurgical techniques. The Neurosurgical Atlas collection presents the nuances of technique for complex cranial and spinal cord operations.
The188bet手机appdepends almost entirely on your donations.
我們無法繼續與您捐贈的捐贈。
請commit at least a yearly $250 donation to the Atlas.如果沒有這一承諾,地圖集將很快要求支付認購事項,並且在世界各地的許多外科醫生都將無法進入其患者的護理依賴於它。
請donate now!
我們無法繼續與您捐贈的捐贈。請commit at least a yearly $250 donation to the Atlas.
Without this commitment, the Atlas will soon require a paid subscriptionand will become inaccessible to many surgeons around the world whose patients’ care depend on it. Please donate now!