
![圖2.23。A.後窩脈絡膜動脈示意圖。上側:後位或枕下位。脈絡膜叢由兩個內側段和兩個外側段組成。每個內側節分為吻側(結節狀)和尾側(扁桃體)部分。每個側段被分為內側,或梗,和外側,或絮凝,部分。髓質,第四腦室,椎動脈和PICAs的起源如下。脈絡膜動脈起源於PICA、SCA和AICA。脈絡膜叢與脈絡膜端相連,脈絡膜端沿著第四腦室底部的邊界與帶絛蟲相連。低:前外側的觀點。 The choroid plexus is seen through the brainstem. The AICA arises from the basilar artery and sends branches that enter the choroid plexus near the flocculus. The SCA may also send choroidal branches to the floccular part of the choroid plexus. Right Center: Diagram showing subdivision of the choroid plexus into medial and lateral segments. The medial segments have nodular and tonsillar parts and the lateral segments have peduncular and floccular parts. The floccular parts protrude through the foramina of Luschka, and the tonsillar parts extend through the foramen of Magendie. B. Schematic illustrations of the choroid plexus of the posterior fossa showing the different patterns of blood supply. Upper: Orienting diagram. The PICA and its plexal area of supply are shown in blue, the AICA in red, and the SCA in green. The PICA divides into vermian and tonsillohemispheric branches. Lower diagrams (A--D): The size of the area supplied by the arteries arising from the AICA, PICA, and SCA is shown. Each half of the schematic diagrams shows a different pattern. Colors used to show plexal areas of supply of the different cerebellar arteries are as follows: red: ipsilateral AICA; orange: contralateral AICA; blue: ipsilateral PICA; yellow: contralateral PICA; and green: ipsilateral SCA. (From, Fujii K, Lenkey C, Rhoton AL Jr: Microsurgical anatomy of the choroidal arteries: Fourth ventricle and cerebellopontine angles. J Neurosurg 52:504–524, 1980 [15].) A., artery; A.I.C.A., anteroinferior cerebellar artery; B.A., basilar artery; Ch., choroidal; F., foramen; fl., floccular; He., hemispheric; L., lateral; M., medial; Med., medulla; no., nodular; pe., peduncular; P.I.C.A., posteroinferior cerebellar artery; Pl., plexus; S.C.A., superior cerebellar artery; to., tonsillar; To., tonsillo; V.A., vertebral artery; Ve., vermian.](https://assets.neurosurgicalatlas.com/eyJidWNrZXQiOiJuc2F0bGFzLWFzc2V0cyIsImtleSI6Im5ldXJvYW5hdG9teVwvUmhvdG9uXy1fTWlzc2VkX0ltYWdlc1wvSW5mcmF0ZW50b3JpYWxfMi4yM19lZGl0ZWQuanBnIiwiZWRpdHMiOnsicmVzaXplIjp7ImZpdCI6ImNvdmVyIiwid2lkdGgiOjE4MzB9LCJqcGVnIjp7InF1YWxpdHkiOjY1fX19)

你可以有所作為。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
現在請捐!
最後更新:2021年4月8日
優化進入後窩的手術入路需要了解小腦動脈與顱神經、腦幹、小腦梗、小腦與腦幹之間的裂隙和小腦表麵的關係(45)。當檢查這些關係時,定義了三種神經血管複合體:與小腦上動脈(SCA)相關的上複合體;與小腦前下動脈(AICA)有關的中間複合體;以及與小腦後下動脈(PICA)相關的下複合體(圖2.1和2.2)(35)。
除了三條小腦動脈外,後顱窩的其他三組結構與SCA、AICA和異食尼卡有著一致的關係,它們是腦幹的部分(中腦、腦橋和髓質);小腦梗(上、中、下);腦幹和小腦(小腦、腦橋小腦和延髓小腦)之間的裂隙;還有小腦的表麵(腦幕,岩麵和枕下)。每個神經血管複叢包括腦幹的三個部分中的一個,小腦的三個表麵中的一個,小腦的三個小腦梗中的一個,小腦和腦幹之間的三個主要裂縫中的一個。此外,每個神經血管複合體都包含一組顱神經。上部複合體包括與SCA相關的動眼神經、滑車神經和三叉神經。中間複合體包括與AICA相關的外展神經、麵神經和前庭耳蝸神經。下複合體包括舌咽神經、迷走神經、副神經和舌下神經,這些神經與異食癖有關。
總之,上複合體包括SCA、中腦、小腦後裂、小腦上梗、小腦幕麵、動眼神經、滑車神經和三叉神經。SCA起於中腦前方,經過動眼神經和滑車神經下方和三叉神經上方,到達小腦後腦裂,在小腦上梗上延伸,並通過供應小腦幕麵而終止。
中間複叢包括AICA、橋腦、小腦中梗、橋小腦裂、小腦岩麵、外展神經、麵神經和前庭耳蝸神經。AICA起於橋腦水平,與外展神經、麵神經和前庭耳蝸神經有關,延伸至小腦中梗表麵,在那裏,它沿著橋小腦裂延伸,並通過供應小腦岩麵而終止。
下複叢包括異食癖、髓質、小腦下梗、小腦髓裂、小腦枕下麵、舌咽神經、迷走神經、脊髓副神經和舌下神經。異食癖發生於髓質水平,環繞髓質,通過與舌咽神經、迷走神經、副神經和舌下神經的關係,到達小腦下梗表麵,在那裏它進入小腦髓裂,並通過供應小腦枕下麵而終止。

SCA或其分支在顱底尖、幕切、三叉神經、橋小腦角、鬆果體區、斜坡和小腦上部的手術入路中暴露(18,19)。
SCA與小腦後腦裂、第四腦室頂上半部、小腦上梗和腦幕麵密切相關(圖2.3-2.5)。SCA起於中腦前方,通常起於顱底動脈近尖處,並通過動眼神經下方,但很少從PCA近端起並通過動眼神經上方。它向尾側下垂,環繞腦幹,靠近橋腦交界處,經過滑車神經下方和三叉神經上方。它的近端部分在小腦幕下遊離邊緣的內側,遠端部分在小腦幕下穿過,使它成為幕下動脈的最前端。它經過三叉神經上方,進入小腦後裂,在那裏它的分支做了幾個急轉彎,形成小腦前動脈,這些動脈通到小腦深層白質和齒狀核。在離開小腦後腦裂時,它的分支在腦幕邊緣的內側,它的分支在腦幕邊緣的後方穿過並分布到腦幕表麵。它通常作為單一中繼出現,但也可能作為雙(或重複)中繼出現。作為一個單一主幹產生的sca分叉為吻側主幹和尾側主幹。SCA向腦幹和小腦梗發出穿孔分支。小腦前分支出現在小腦中腦裂內。 The rostral trunk supplies the vermian and paravermian area and the caudal trunk supplies the hemisphere on the suboccipital surface. The SCA frequently has points of contact with the oculomotor, trochlear, and trigeminal nerves.
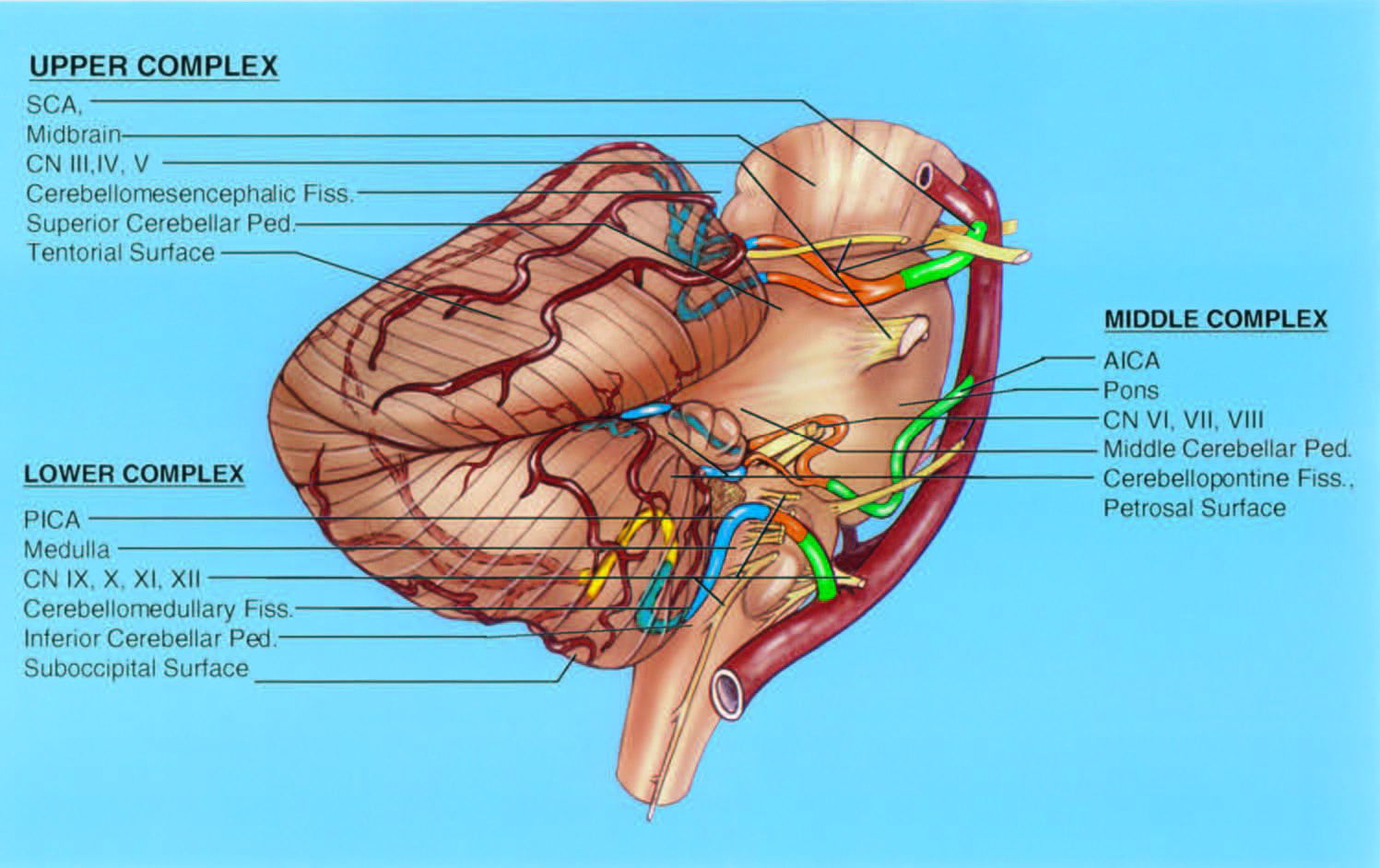
圖2.1。在後窩的三個神經血管複叢中,每一個都包括三條小腦動脈中的一條,腦幹的三個部分中的一個,三個小腦梗中的一個,三個小腦麵中的一個,腦幹和小腦之間的三個裂隙中的一個,以及三組腦神經中的一組。上麵的複合體與SCA有關,中間的複合體與AICA有關,下麵的複合體與PICA有關。上部複合體包括SCA、中腦、小腦上梗、小腦後裂、小腦幕麵、動眼神經、滑車神經和三叉神經。中間複群包括異食癖、橋腦、小腦中梗、橋小腦裂、岩麵、外展神經、麵神經和前庭耳蝸神經。下複叢包括異食癖、髓質、小腦下梗、小腦髓裂、枕下麵,以及舌咽神經、迷走神經、副神經和舌下神經。SCA被分為四個節段:前側橋腦(綠色)、側橋腦(橙色)、小腦(藍色)和皮質(紅色)。每個段可以由一個或多個主幹組成,這取決於主幹線的分支級別。AICA分為四個部分:橋前(綠色)、橋髓外側(橙色)、絮凝結節(藍色)和皮質(紅色)。PICA被分為五個部分:前髓質(綠色),側髓質(橙色),扁桃體髓質(藍色),端速扁桃體(黃色)和皮質(紅色)。 A.I.C.A., anteroinferior cerebellar artery; CN, cranial nerve; Fiss., fissure; Ped., peduncle; P.I.C.A., posteroinferior cerebellar artery; S.C.A., superior cerebellar artery.
SCA被分為四個節段:前側橋腦、外側橋腦、小腦和皮質(圖2.1)。每個段可以由一條或多條主幹組成,這取決於主幹線的分叉程度(圖2.6)。
這個部分位於鞍背和上腦幹之間。它開始於SCA的起點,並延伸到動眼神經以下的腦幹前外側邊緣。它的外側部分在遊離幕邊緣前半部分的內側。
這段開始於腦幹的前外側邊緣,經常向尾側延伸到橋腦上側的外側(圖2.1、2.7和2.8)。它的尾袢向三叉神經的根入口區延伸並經常到達橋中水平。滑車神經穿過這個節段的中間部分。這部分的前部通常在幕邊緣以上可見,但尾袢通常將它帶到幕下。這一段終止於小腦後腦裂的前緣。基底靜脈和主動脈在其上並與主動脈平行。
該節段位於小腦後腦裂內(圖2.7-2.9)。SCA分支進入位於三叉神經根入口區上方的裂隙最淺部分,再次向幕邊緣內側延伸,其分支與滑車神經纏繞在一起。SCA進入的裂隙向內側逐漸加深,在上髓膜後方中線處最深。通過一係列發夾狀的曲線,SCA深入到裂隙中,向上延伸到幕麵的前邊緣。SCA的主幹和分支被穿透裂縫相對壁的分支固定在裂縫中。在這個裂隙中,SCA的單個分支由於分支的尖銳曲線和大量交織的動脈環而難以識別。
這一段包括小腦後腦裂遠端分支,它們穿過幕邊緣下方,分布到幕表麵,如果存在邊緣分支,則分布到岩麵上部(圖2.6-2.9)。

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.2。A,腦幹和小腦動脈的前視圖。B,顱底後視圖,保留了顱神經和動脈。A和B, SCA出現在中腦水平,並環繞 腦幹附近的橋腦連接。SCA位於動眼神經和滑車神經下方,三叉神經上方。SCA在B處比在a處更靠近三叉神經。AICA在橋腦水平出現,經過外展神經、麵神經和前庭耳蝸神經。在A區,兩個aica通過外展神經的下方。在B區,左側外展神經經過AICA前麵,右側外展神經經過AICA後麵。pica起源於椎動脈髓質水平,與舌咽神經、迷走神經、副神經和舌下神經有關。sca的起源從一側到另一側是相當對稱的。 There is slight asymmetry in the level of origin of the AICAs and marked asymmetry in the level of the origin of the PICAs, especially in A. A., artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; CN, cranial nerve; P.C.A., posterior cerebral artery; P.I.C.A., posteroinferior cerebellar artery; S.C.A., superior cerebellar artery; Sp., spinal; Vert., vertebral.
![圖2.3。小腦動脈的關係。A,後視圖,左小腦和部分右腦被切除。B,側位圖,切除左小腦,露出第四腦室。SCAs(黃色)與第四腦室頂上半部和小腦後腦裂密切相關;aica(橙色)與橋小腦裂和側隱窩密切相關;PICAs(紅色)與屋頂尾半部和小腦延髓裂密切相關。骶髂韌帶在三叉神經上方繞過中腦,分為吻側幹和尾側幹。這些主幹的分支深入小腦後腦裂,並發出小腦前動脈,這些動脈沿著小腦上梗延伸到齒狀核。PICAS起源於椎動脈,通過舌咽神經、迷走神經和副神經之間到達小腦髓裂。 After passing near the caudal pole of the tonsils, where they form a caudal loop, they ascend through the cerebellomedullary fissure, where they are intimately related to the caudal part of the ventricular roof. They pass around the rostral pole of the tonsil and through the telovelotonsillar cleft, where they form a cranial loop. In their course around the tonsils, they divide into medial and lateral trunks. They give off branches to the dentate nuclei near the superior pole of the tonsils. The AICAs arise from the basilar artery and pass near or between the facial and vestibulocochlear nerves and are intimately related to the cerebellopontine fissures, the flocculi, and the lateral recesses. The AICAs divide into rostral and caudal trunks before reaching the facial and vestibulocochlear nerves. The rostral trunk passes between the nerves and along the middle cerebellar peduncle near the cerebellopontine fissure. The caudal trunk passes below the nerves and near the lateral recess to supply the lower part of the petrosal surface. The AICA and the PICA give rise to the choroidal arteries, which supply the tela choroidea and attached choroid plexus. (From, Matsushima T, Rhoton AL Jr, Lenkey C: Microsurgery of the fourth ventricle: Part I—Microsurgical anatomy. Neurosurgery 11:631–667, 1982 [35].) A., artery; A.I.C.A., anteroinferior cerebellar artery; B., basilar; Ca., caudal; Cer., cerebellar; Cer. Med., cerebellomedullary; Cer. Mes., cerebellomesencephalic; Ch., choroid, choroidal; Coll., colliculus; Dent., dentate; F., foramen; Inf., inferior; Lat., lateral; Med., medial, medullary; Mid., middle; Nucl., nucleus; P.C.A., posterior cerebral artery; Ped., peduncle; P.I.C.A., posteroinferior cerebellar artery; Pl., plexus; Ro., rostral; S.C.A., superior cerebellar artery; Sup., superior; Tr., trunk; V., vein; V.A., vertebral artery; Vel., velum.](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_Book_-_Posterior_Fossa/Figure_2.3.png)
點擊這裏查看此圖像的交互模塊和相關內容。
圖2.3。小腦動脈的關係。A,後視圖,左小腦和部分右腦被切除。B,側位圖,切除左小腦,露出第四腦室。SCAs(黃色)與第四腦室頂上半部和小腦後腦裂密切相關;aica(橙色)與橋小腦裂和側隱窩密切相關;PICAs(紅色)與屋頂尾半部和小腦延髓裂密切相關。骶髂韌帶在三叉神經上方繞過中腦,分為吻側幹和尾側幹。這些主幹的分支深入小腦後腦裂,並發出小腦前動脈,這些動脈沿著小腦上梗延伸到齒狀核。PICAS起源於椎動脈,通過舌咽神經、迷走神經和副神經之間到達小腦髓裂。 After passing near the caudal pole of the tonsils, where they form a caudal loop, they ascend through the cerebellomedullary fissure, where they are intimately related to the caudal part of the ventricular roof. They pass around the rostral pole of the tonsil and through the telovelotonsillar cleft, where they form a cranial loop. In their course around the tonsils, they divide into medial and lateral trunks. They give off branches to the dentate nuclei near the superior pole of the tonsils. The AICAs arise from the basilar artery and pass near or between the facial and vestibulocochlear nerves and are intimately related to the cerebellopontine fissures, the flocculi, and the lateral recesses. The AICAs divide into rostral and caudal trunks before reaching the facial and vestibulocochlear nerves. The rostral trunk passes between the nerves and along the middle cerebellar peduncle near the cerebellopontine fissure. The caudal trunk passes below the nerves and near the lateral recess to supply the lower part of the petrosal surface. The AICA and the PICA give rise to the choroidal arteries, which supply the tela choroidea and attached choroid plexus. (From, Matsushima T, Rhoton AL Jr, Lenkey C: Microsurgery of the fourth ventricle: Part I—Microsurgical anatomy. Neurosurgery 11:631–667, 1982 [35].) A., artery; A.I.C.A., anteroinferior cerebellar artery; B., basilar; Ca., caudal; Cer., cerebellar; Cer. Med., cerebellomedullary; Cer. Mes., cerebellomesencephalic; Ch., choroid, choroidal; Coll., colliculus; Dent., dentate; F., foramen; Inf., inferior; Lat., lateral; Med., medial, medullary; Mid., middle; Nucl., nucleus; P.C.A., posterior cerebral artery; Ped., peduncle; P.I.C.A., posteroinferior cerebellar artery; Pl., plexus; Ro., rostral; S.C.A., superior cerebellar artery; Sup., superior; Tr., trunk; V., vein; V.A., vertebral artery; Vel., velum.

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.4。模擬。小腦動脈,腦幹,小腦-腦幹裂。後外側的視圖。SCA繞過中腦進入小腦後腦裂,在那裏它發送穿孔分支進入中腦後側,位於上丘和下丘之間的一條線上,並沿上椎梗向下到達齒狀核。AICA環繞小葉、麵神經和前庭耳蝸神經。左異食癖穿過進入頸靜脈孔的神經根之間,在左側扁桃體的下極(已被切除)周圍尾側轉彎,然後上升,在扁桃體的上極與腦室頂下半部分交界處形成顱環。B,另一個標本。左小腦被切除了。SCA在周圍池和四頭池的下部繞過PCA下方的中腦,進入小腦後腦裂,並在裂的後唇盤旋,供應腦幕表麵。 The PICA arises from the vertebral artery, passes around the medulla, crosses the inferior cerebellar peduncle, and enters the cerebellomedullary fissure, where it passes along the inferior half of the ventricular roof, and exits the fissure to supply the suboccipital surface. The AICA passes laterally around the pons and above the flocculus. C, enlarged oblique view. The right PICA loops around the caudal and rostral poles of the tonsil. The left PICA dips below the level of the foramen magnum. D, posterior view after removing all of the cerebellum except for the right tonsil and dentate nucleus. A., artery; A.I.C.A., anteroinferior cerebellar artery; Caud., caudal; Cer. Med., cerebellomedullary; Cer. Mes., cerebellomesencephalic; Chor., choroid; CN, cranial nerve; Cran., cranial; Dent., dentate; Fiss., fissure; Flocc., flocculus; Inf., inferior; Mid., middle; Nucl., nucleus; P.C.A., posterior cerebral artery; Ped., peduncle; P.I.C.A., posteroinferior cerebellar artery; Plex., plexus; S.C.A., superior cerebellar artery; Sup., superior; Vent., ventricle; Vert., vertebral.

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.4。E和F. 小腦動脈,腦幹, 和小腦-腦幹裂。E, SCA穿過 三叉神經並進入小腦後腦裂,在那裏它將 分支沿上 神經梗向下發送到 齒狀核。異食癖在迷走神經和 副神經之間通過 ,並在下足梗上經過 至 ,到達小腦延髓 裂。F, 側隱窩的放大視圖。 小葉和脈絡膜叢 從 Luschka孔的 緣向外側投射到 橋小腦角, 在舌咽部 和迷走神經後麵, 在PICA上麵。舌下 小根起源於舌咽神經和迷走神經前麵的髓質,穿過椎動脈的後表麵。有些舌下根在異食癖起源的上方通過,有些在異食癖起源的下方通過。
SCA是小腦幕下動脈中存在和供血區域最一致的動脈(49)。沒有
雖然罕見,但已有報道(50例)。在我們之前對50個sca的研究中,43個作為單一中繼出現,7個作為兩個(重複)中繼出現(19個)。我們檢查的大腦中,隻有一個大腦出現了雙側重複的樹幹。起源的三倍是罕見的。50例sca中除2例外均起源於基底動脈。這兩個例外完全或部分來自大腦後動脈,並通過動眼神經之上,之後遵循典型的遠端路線。非重複鱗狀動脈的獨立幹和重複鱗狀動脈的吻側幹通常來自於基底動脈的下方,但直接與PCA的起源相鄰。不發生在PCA原點附近的動脈發生在PCA原點2.5 mm以內。
左右sca和pca的起源通常呈十字形,其中肢體在基底動脈的頂端交叉(圖2.2)。基底動脈分叉的高度是起始路徑的一個重要決定因素(47,59)。基底動脈分支位於橋腦交界處為正常水平,位於中腦前方為高水平,位於橋腦前方為低水平。如果分岔高,SCA的起點在幕頂邊緣以上,如果正常,則在遊離邊緣中間,如果低,則在幕頂以下。在我們的研究中,在我們檢查的25個大腦中,有18個的分支處於正常位置,6個是高的,1個是低的。6條高分叉動脈中的3條與胎兒起源的PCA相關(47)。
基底動脈的長度範圍為20 - 40mm(平均,30),其直徑在椎動脈的起源處更大,範圍為3 - 8mm(平均,5-6 mm),而在其頂端(範圍,3 - 7mm;意思是,4 - 5毫米)。基底動脈通常是直的或偏離中線很短的距離,但少數會向外側偏離到外展神經或麵神經和前庭耳蝸神經的起點(18,19)。
所有作為單一血管出現的sca都分叉成兩個主幹,一個吻側和一個尾側(圖2.10)。該分叉發生在距起源0.6 - 34.0 mm(平均19 mm)之間,最常發生在腦幹外側動脈最大尾側下降點附近。幾乎每個腦半球都有吻側和尾側主幹,這是重複起源或主動脈分叉的結果。由重複起源形成的吻側和尾側主幹稱為吻側和尾側重複SCA,其分布與單個SCA的分叉形成的吻側和尾側主幹相當。
吻側幹通過提供蚓部和鄰近半球的可變部分而終止。尾側幹支配由吻側幹支配的區域外側的半球表麵。吻側幹和尾側幹的直徑大致相等,但如果其中一個較小,通常是尾側幹。如果一個主幹很小,另一個主幹提供較大的麵積。尾幹很少向蚓部分支。

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.5。模擬。小腦動脈。優越的觀點。A,兩個sca作為中腦水平的重複動脈出現並伴隨腦幹周圍的基底靜脈進入小腦後腦裂。它們經過動眼神經和滑車神經下麵三叉神經上麵。SCA幹與腦幹後外側滑車神經纏繞在一起。B,腦幹部分已經向下延伸到腦橋。雙側骶管的吻側和尾側幹直接從基底動脈的一側發出,並在三叉神經的外側上方通過。 C,腦幹部分已經延伸到中腦橋。將三叉神經、動眼神經和滑車神經分開,以便腦幹向後反射,暴露AICA和麵神經和前庭耳蝸神經。 Both AICAs pass below the abducens nerves and loop laterally toward the internal acoustic meatus. The left PICA loops upward in front of the pons between the facial and vestibulocochlear nerves and the AICA before turning downward to encircle the medulla. D, enlarged view. The right AICA loops laterally into the porus of the internal acoustic meatus, as occurs in approximately half of cases. The AICA has a premeatal segment that passes toward the meatus, a meatal segment that loops into the porus in about half of cerebellopontine angles, and a postmeatal segment that loops back to the brainstem. The vestibulocochlear nerve has been retracted to expose the nervus intermedius, which arises at the brainstem along the anterior surface of the vestibulocochlear nerve, has a free segment in the cerebellopontine angle, and joins the facial nerve as it proceeds laterally toward the meatus. The AICA gives rise to a recurrent perforating branch to the brainstem. A., artery; A.I.C.A., anteroinferior cerebellar artery; Bas., basilar; Bridg., bridging; Cer. Mes., cerebellomesencephalic; CN, cranial nerve; Fiss., fissure; Flocc., flocculus; Intermed., intermedius; Meat., meatal; Mes., mesencephalic; Nerv., nervus; P.C.A., posterior cerebral artery; Ped., peduncle; Perf., perforating; P.I.C.A., posteroinferior cerebellar artery; Premeat., premeatal; Rec., recurrent; S.C.A., superior cerebellar artery; Seg., segment; V., vein; Vent., ventrical; Vert., vertebral.

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.5。情況。小腦動脈。E,放大視圖。左耳鼻喉管起於基底動脈,向外側穿過內聽道孔,然後在麵神經和前庭耳蝸神經之間轉向內側。彎曲的異食癖在AICA和麵神經之間向上循環,然後向下轉動。F, AICA和進入內聽道的神經被分開了。異食癖先向上循環,然後向尾側旋轉,穿過迷走神經和副神經的細根。舌下神經起源於橄欖前的腦幹。舌下神經的其中一根細根在異食癖起源處盤旋向上,然後向下在舌下管處與其他細根彙合。 A bridging vein passes from the medulla to the jugular bulb. G, the section has been extended downward to the level of the medulla to show the perforating branches of the vertebral and basilar arteries entering the medullary pyramids and the lateral medulla. The glossopharyngeal, vagus, and accessory nerves arise dorsal to the olives. The hypoglossal nerve arises ventral to the olives and passes behind the vertebral arteries. H, the medullary section has been extended caudally. The level of the PICA origins from the vertebral arteries are asymmetric. The right PICA intermingles with multiple rootlets of the hypoglossal nerve, while the left PICA, which arises at a higher level, has only the upper hypoglossal rootlet stretched around it. The PICAs encircle the medulla and appear on the dorsal surface behind the fourth ventricle. The left is larger than the right vertebral artery.
這些射孔分支分為直流式和旋流式(圖2.7)。直接型沿著一條直線進入腦幹。旋回型在腦幹周圍纏繞,最後在腦幹終止。旋狀穿通動脈分為短型和長型。短旋回型繞腦幹周長移動90度或更小。長旋流型移動更大的距離到達對麵的表麵。兩種類型的旋動脈都在其運行過程中將分支送入腦幹。
穿孔枝產生於絕大多數的主幹、吻側主幹和尾側主幹。大多數主幹會產生2 - 5個穿孔枝,盡管有些可能不會產生穿孔枝,而另一些則會產生多達10個穿孔枝。從主幹產生的最常見的穿通動脈類型是長旋支,但它也產生直接和短旋支。從大到小依次為主幹分支終止於小腦上、中末梢、足間窩(通常為直接型)、腦梗和丘區交界區域的被蓋。
吻側和尾側主幹的分支最常旋曲。它們繞著腦幹運動,到達兩個主要區域:小腦上踝和中踝的連接處和四頭池,位於上丘和下丘之間的溝下方。按降序排列,它們終止於小腦上、中踝、下丘、腦踝和踝間窩之間的連接處。
基底動脈還形成腦幹的多個穿孔分支。在SCA起源附近產生的分支與SCA近端產生的直接穿孔分支混合。那些在SCA起源以上產生的進入椎間窩。
小腦前動脈起源於小腦間裂的主幹和皮層分支(圖2.7- 2.9)。裂隙內可能出現多達8根小腦前動脈,再加上主幹和皮質分支以及裂隙內的急轉彎,造成了動脈解剖和識別的複雜性。這些小腦前支連接著主幹的遠端和裂內皮質動脈的近端。小腦前動脈由內側一組穿過上髓膜和中央小葉之間的小分支和外側一組穿過上、中小腦梗和中央小葉兩翼之間的大分支組成。位於蚓部外側的皮層動脈向大腦半球表麵提供小腦前分支,這些分支到達齒狀核和小腦深部核,終止於蚓部的皮層動脈向下丘和上髓膜提供分支。

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.6。SCA,小腦-後腦裂,和腦幕麵。優越的觀點。A, sca穿過中腦進入小腦後腦裂,在裂內經過一係列發夾狀轉彎後,繞過裂後唇到達腦幕表麵。四頭腦池的下部延伸至小腦後腦裂。帳篷的表麵從裂縫後麵的頂端向下傾斜。B,前上的觀點。左側SCA發生在一條重複動脈上。在最初的過程中,SCAs在腦幕邊緣下方橫向循環,但進一步向後,它們在腦幕邊緣下方內側進入小腦後裂。C,另一個小腦。 The SCAs loop into the cerebellomesencephalic fissure, where they undergo a series of hairpin turns before exiting the fissure to supply the tentorial surface. D, the posterior lip of the fissure has been retracted to expose the branches of the SCA within the fissure. Cer. Mes., cerebellomesencephalic; Cist., cistern; CN, cranial nerve; Coll., colliculus; Dup., duplicate; Fiss., fissure; Inf., inferior; P.C.A., posterior cerebral artery; Pet., petrosal; Quad., quadrigeminal; S.C.A., superior cerebellar artery; Str., straight; Sup., superior; Tent., tentorial; V., vein.
SCA最穩定的皮質供給是腦幕表麵(圖2.6-2.9)。SCA的皮層區域比AICA和PICA更恒定,但與它們是倒數的。尖沙帶通常分布在大部分的穹幕表麵,也經常分布在相鄰的岩石表麵的上部。最大供血區包括與蚓部對半部重疊的幕麵的整整一半、枕下表麵的上部和岩麵的上三分之二,包括岩裂的兩個唇部。最小的供給場隻包括位於幕裂前的幕麵部分。
皮層分支分為半球組和蚓組(圖2.7)。蚓部每半的皮層表麵分為內側段和中間段,蚓部外側的每個半球分為內側段、中間段和外側段,因為最常見的模式包括兩個蚓動脈和三個與這些段對應的半球動脈。
![圖2.7。SCA的關係。A, SCA左側側麵視圖,切除部分小腦,顯示小腦上梗在齒狀核的終止。SCA主幹經過動眼神經和滑車神經下方和三叉神經上方,分為吻側幹和尾側幹。視神經束和旋短動脈環繞腦幹。小腦前動脈起源於小腦後腦裂,供應鄰近的小腦和下丘,並沿小腦上梗向齒狀核發出分支。上丘主要由異食癖供血。吻側和尾側主幹分裂為蚓動脈和外側動脈、內側動脈和中間半球動脈。B,切除小腦後腦裂上唇,顯示裂內分支。旋狀穿通動脈止於下丘和小腦上、中末梢交界處。 The precerebellar branches pass along the superior cerebellar peduncles to the dentate nucleus. The right half of the vermis is supplied by a large vermian artery and the hemispheric surface is supplied by medial, intermediate, and lateral hemispheric arteries. (From, Hardy DG, Peace DA, Rhoton AL Jr: Microsurgical anatomy of the superior cerebellar artery. Neurosurgery 6:10–28, 1980 [19].) A., artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; B., basilar; Bo., body; Ca., caudal; Cer., cerebellar; Circ., circumflex; Co., communicating; Coll., colliculus; Dent., dentate; Gen., geniculate; He., hemispheric; Inf., inferior; Int., intermediate; L., long; Lat., lateral; Med., medial; Nucl., nucleus; O., optic; P., posterior; P.C.A., posterior cerebral artery; Ped., peduncle; Ro., rostral; S., short; Sup., superior; Tr., trunk; V., ventricle or vertebral; Ve., vermian.](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Infratentorial_2.7.jpg)
圖2.7。SCA的關係。A, SCA左側側麵視圖,切除部分小腦,顯示小腦上梗在齒狀核的終止。SCA主幹經過動眼神經和滑車神經下方和三叉神經上方,分為吻側幹和尾側幹。視神經束和旋短動脈環繞腦幹。小腦前動脈起源於小腦後腦裂,供應鄰近的小腦和下丘,並沿小腦上梗向齒狀核發出分支。上丘主要由異食癖供血。吻側和尾側主幹分裂為蚓動脈和外側動脈、內側動脈和中間半球動脈。B,切除小腦後腦裂上唇,顯示裂內分支。旋狀穿通動脈止於下丘和小腦上、中末梢交界處。 The precerebellar branches pass along the superior cerebellar peduncles to the dentate nucleus. The right half of the vermis is supplied by a large vermian artery and the hemispheric surface is supplied by medial, intermediate, and lateral hemispheric arteries. (From, Hardy DG, Peace DA, Rhoton AL Jr: Microsurgical anatomy of the superior cerebellar artery. Neurosurgery 6:10–28, 1980 [19].) A., artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; B., basilar; Bo., body; Ca., caudal; Cer., cerebellar; Circ., circumflex; Co., communicating; Coll., colliculus; Dent., dentate; Gen., geniculate; He., hemispheric; Inf., inferior; Int., intermediate; L., long; Lat., lateral; Med., medial; Nucl., nucleus; O., optic; P., posterior; P.C.A., posterior cerebral artery; Ped., peduncle; Ro., rostral; S., short; Sup., superior; Tr., trunk; V., ventricle or vertebral; Ve., vermian.
半腦支起於小腦後腦裂深處的吻側和尾側幹。它們形成小腦前動脈,並在小腦後腦裂內結合其近端部位。離開裂隙後,半支繼續供應蚓部外側的幕麵。吻側幹和尾側幹合在一起,最常見的是產生三個,但有時多達五個的半球分枝。半球動脈之間有一種相互作用的關係。如果一艘船很小,那麼相鄰的船就很大,通常由更簡陋的船提供。
最常見的模式是三個半球分支:外側、中間和內側,對應於它們所提供的半球表麵的三分之一。每個分支約占半球幕麵的三分之一。然而,也經常有例外,即大腦半球區域由兩個分支或來自相鄰半球節段的分支提供。內側段最常由吻側幹供給,外側段最常由尾側幹供給。蚓動脈偶爾與半腦內側段重疊,邊緣動脈(稍後描述)與半腦外側段重疊。整個腦幕半球表麵由一個半球尾幹的分支和另一個半球吻側幹的分支構成。在到達腦幕表麵時,半腦動脈分裂成一到七個(平均為三個)分支,這些分支在腦幕表麵上喬木,最終消失在小腦葉之間。
蚓動脈起源於小腦後腦裂內的吻側幹。吻側幹最常見的是產生兩條蚓動脈(最多四條)。如果一側的蚓支發育不良,則其區域由對側SCA的分支提供。最常見的是兩條蚓動脈:一條分布在中線附近的內側條上,另一條分布在半球表麵附近的中端條上。兩側蚓支之間的吻合經常發生在靠近幕麵頂點的地方。
近端SCA主幹約有一半形成了鄰近岩石表麵的邊緣分支(圖2.9和2.10)。當出現時,邊緣分支是第一個皮層分支。它通常起源於橋腦外側段,不像其他皮層分支那樣進入小腦後腦裂,而是從它的起源處進入皮層表麵。它也可能起源於尾動脈或主幹,或起源於基底動脈,作為SCA的一個重複起源的變體。它最恒定的供給是靠近穹幕表麵的岩麵部分。它的最大供應區域包括岩石表麵上部的全部範圍和岩石裂隙的兩個唇。其供應麵積與AICA供應的岩石表麵積大小成反比。如果邊緣動脈很小或沒有,則AICA或它的分支提供岩石裂隙的大部分。邊緣動脈與AICA之間的吻合是常見的,如果邊緣支較大,則吻合最為明顯。從小腦梗中部區域的邊緣分支末端產生的穿孔分支。
SCA靠近並經常與動眼神經、滑車神經或三叉神經接觸(圖2.2、2.5和2.8)。
SCA的近端向下通過,並通過動眼神經與PCA分離(圖2.5)。近三分之二的sca與動眼神經有接觸點,通常在下表麵。接觸點通常涉及主幹,如果有早期分叉,則較少涉及吻側主幹。這是一種神經上表麵的接觸,隻有當SCA起源於PCA時,這種情況很少發生。桑德蘭認為,動眼神經可能偶爾會在PCA和SCA之間收縮(52)。
血管起點與動眼神經接觸點之間的長度平均為4.5毫米(範圍1-9毫米),神經起點與中腦接觸點之間的長度平均為5毫米(範圍1-10毫米)(19)。動脈接觸點的直徑平均為2毫米(範圍1-3毫米)。如果有重複起點,基底動脈低起點,或PCA的胎兒型,則不太可能與動眼神經有接觸點。
滑車神經起於下丘下方,並在小腦後腦裂內向前延伸(圖2.4、2.5和2.10)。它從吻側主幹和尾側主幹分支的內側到外側,在裂隙內向前穿過。到達腦幹外側後,它在幕下表麵和SCA之間經過。幾乎在所有情況下,神經都與SCA主幹有接觸點。這種接觸可能涉及主幹、吻側主幹或尾側主幹,也可能涉及吻側主幹和尾側主幹。神經接觸點距離神經原點平均為17mm (4 - 30mm),距離SCA原點平均為24mm (13 - 38mm)(18)。
三叉神經起於腦橋外側,斜向上延伸(圖2.8和2.10)。它從後顱窩向前穿過在腦幕附著下進入梅克爾洞。SCA在三叉神經上方環繞腦幹,在腦橋外側形成一個淺尾袢(18)。在尾部突出環最突出的情況下,SCA和三叉神經之間發生接觸。大約一半的腦脊梁與腦脊梁有一個連接點,這取決於分叉的位置,可能涉及主主幹、吻側主幹、尾側主幹或吻側主幹和尾側主幹或半球邊緣分支。接觸點的血管直徑平均為1至2毫米,但也可能小於2毫米至近3毫米。血管起點與三叉神經接觸點之間的距離為15 ~ 33毫米(平均21毫米)。SCA與24條三叉神經之間的距離小於1 - 8mm(平均為3mm),無神經血管接觸。
與SCA的接觸點通常在神經的上或超內側。通常,一些神經束被血管壓痕或扭曲3 - 4mm,但在進入腦橋的周圍可達12mm。在我們檢查的50個樣本中,有6個樣本的接觸位於橋腦根入口區,通常是由腦幹和三叉神經內側之間的腋窩形成的一個環。SCA原點的結構與壓迫三叉神經的環的有無之間沒有相關性;然而,SCA的分叉點確實影響與神經接觸的血管的口徑。如果早期有SCA分叉,則接觸血管的口徑較小。這些接觸在三叉神經痛中的意義在關於橋小腦角的章節(7,16,22,45)中進行了綜述。

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.8。SCA關係。第一,左SCA是一條重複動脈。尾側重複幹在進入小腦後裂之前穿過三叉神經的吻側麵。B,右SCA在到達小腦後腦裂前緣之前不分為吻側幹和尾側幹。C,靠近原點處,SCA在動眼神經下方,遠端靠近進入小腦後裂的入口處,通過滑車神經下方。D,另一個SCA。一個大主幹直接從腦幹一側到腦半球表麵,而不進入腦裂,盡管它也向腦裂發出一些較小的分支。E,小腦後裂的後唇被切除第四腦室頂部的上半部分被打開。SCA產生穿過小腦上梗的穿孔分支,為齒狀核供血。 F, oblique posterior view of the SCA branches within the cerebellomesencephalic fissure and the quadrigeminal cistern. The SCA supplies the cisternal walls below the sulcus between the superior and inferior colliculi, and the PCA supplies the wall above this level. A.I.C.A., anteroinferior cerebellar artery; Br., branch; Caud., caudal; Cer. Mes., cerebellomesencephalic; Cist., cistern; CN, cranial nerve; Coll., colliculus; Fiss., fissure; Inf., inferior; Mid., middle; P.C.A., posterior cerebral artery; Ped., peduncle; Pet., petrosal; Quad., quadrigeminal; Rost., rostral; S.C.A., superior cerebellar artery; Sup., superior; Tent., tentorial; Tr., trunk; Vent., ventricle.

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.9。A,右SCA起源於基底動脈作為一條雙動脈。喙側重複幹產生蚓部分支,提供蚓部和半球的鄰近部分。尾部的重複幹產生半球形的分枝。B,放大圖。在閉塞和分割三叉神經周圍的岩上靜脈時需要小心,因為SCA的分支可能與靜脈的支流交織在一起,如本例所示。足靜脈通常流入基底靜脈,與外側中腦靜脈彙合,並流入岩上竇。C,裂縫的邊緣已被收回,露出SCA的主幹和分支。D,小腦後裂的後唇被切除了。在裂隙內,SCA分支向下延伸至小腦上梗。 Some SCA branches pass above and some below the trochlear nerve. The SCA gives rise to a marginal branch that supplies some of the petrosal surface bordering the tentorial surface. Br., branch; Caud., caudal; Cer. Mes., cerebellomesencephalic; CN, cranial nerve; Fiss., fissure; Hem., hemispheric; Lat., lateral; Marg., marginal; Mes., mesencephalic; Ped., peduncle; Pet., petrosal; Rost., rostral; S.C.A., superior cerebellar artery; Sup., superior; Tent., tentorial; Tr., trunk; V., vein; Verm., vermian.
切幕(切口),穿過小腦幕的開口,與斜坡上的基底呈三角形(圖2.6、2.8和2.9)(41)。其他兩肢由左右遊離緣組成,在枕葉下麵的枕丘和枕葉上麵的枕葉之間的頂點連接。
SCA的近端部分,通常為主幹,除非有重複起源或早期分叉,位於遊離緣前三分之一內側。高起點的sca出現於穹幕邊緣之上,但所有這些斜坡的初始過程都是在尾側。近20%的SCAs與幕前半部分遊離邊緣有接觸點。遠端,SCA繞尾和通過下麵,有時接觸中間三分之一的自由邊緣的帳篷。當SCA通過自由邊緣以下時,自由邊緣和SCA之間的間隔平均為3毫米(範圍為0-5毫米)。在大多數情況下,最靠近自由邊緣下表麵的部分是主幹,但如果早期有分叉,則可能是吻側或尾側主幹。再往遠端,分支通過遊離邊緣後三分之一內側進入和離開小腦後腦裂。這些分支在丘和枕葉之間的遊離邊緣水平的尾部,但遠端通過幕下到達小腦上表麵。

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.10。SCA的樹幹。A, SCA的主幹在三叉神經上麵分叉形成吻側幹和尾側幹。主幹在滑車神經和腦幕邊緣的前外側經過,而遠端吻側幹在滑車神經和腦幕邊緣的上方通過,尾側幹在滑車神經和腦幕邊緣的下方通過。B、去掉幕邊後查看。三叉神經痛中最常見的壓迫三叉神經的是位於主幹與吻側主幹和尾側主幹交界處的SCA,在本例中位於三叉神經上方。在到達腦幕表麵之前,兩根主幹都深入小腦後腦裂。C,這個岩上靜脈有多個支流,它們與SCA的分支纏繞在一起。這些靜脈在到達三叉神經時通常需要凝固和分裂。除非小心翼翼地將動脈幹與靜脈支分開,否則在凝固岩上靜脈支的過程中SCA可能被清除。 D, this SCA has a duplicate origin in which both the rostral and caudal trunks arise directly from the basilar artery. Both trunks, at the anterolateral brainstem, pass below the tentorial edge and trochlear nerve and above the trigeminal nerve. At the posterolateral margin of the brainstem, the rostral trunk loops above the level of the trochlear nerve and tentorial edge. The caudal trunk rests against the posterior trigeminal root as the nerve passes below the anterior edge of the tentorium to enter Meckel’s cave. E, another SCA. The main trunk passes above the trigeminal nerve before bifurcating into rostral and caudal trunks. The main trunk courses below the trochlear nerve, but the rostral trunk loops upward medial to the nerve. The caudal trunk divides into a large hemispheric branch that supplies the tentorial surface and a marginal branch, which supplies some of the upper part of the petrosal surface. F, another SCA. The artery bifurcates below the oculomotor nerve. Both trunks pass below the trochlear nerve at the anterolateral margin of the brainstem and above the trochlear nerve distally at the entrance into the cerebellomesencephalic fissure. A., artery; Bas., basilar; Br., branch; Caud., caudal; Cer. Mes., cerebellomesencephalic; CN, cranial nerve; Fiss., fissure; Hem., hemispheric; Marg., marginal; Pet., petrosal; Rost., rostral; S.C.A., superior cerebellar artery; Sup., superior; Tent., tentorial; Tr., trunk; V., vein.
小腦動脈閉塞的影響範圍從臨床沉默到腦幹或小腦部分梗死,並伴有腫脹、出血和死亡(3,18,19,30)。SCA閉塞雖然不常見,但可產生獨特的臨床圖像,其原因是小腦、齒狀核、結膜臂和橋吻側被膜中的長感覺通路的梗死(32)。症狀表現為嘔吐、突然頭暈、無法站立或行走。閉塞可能導致小腦功能障礙,這是由於小腦及其深部核和花序梗受累所致;齒狀核及小腦上梗受累所致同側意向性震顫;眼交感神經降纖維受累致同側霍納氏綜合征;脊髓丘腦外側束和五丘腦束受累引起的對側疼痛和溫度感覺喪失;內側縱束和小腦通路受累所致眼球震顫;外側神經叢交叉纖維受累致對側聽力障礙;以及由於上腦幹的無意識模仿通路受損而導致的鎮痛側情緒表達的喪失。 Although a specific clinical syndrome may result from an SCA occlusion, it is worth emphasizing that in the posterior fossa, a given area of parenchyma cannot be as predictably allotted to a specific vessel as in the cerebral circulation, because of the extensive anastomoses over the cerebellum and the variation in arterial distribution.
許多患者在有意閉塞小腦大動脈後的恢複和存活歸功於側支循環的充足。如果相鄰動脈異常小而閉塞的動脈很大,則側支循環很可能很差,造成不利和危險的情況。由腦收縮引起的機械刺激引起的動脈痙攣可能使側支供血減弱。任何一條小腦動脈的急性閉塞常伴有嘔吐、頭暈和無法站立或行走。
SCA在出血性和缺血性後窩腦血管病中都很重要。齒狀核是自發性小腦出血最常見的部位,由小腦前和SCA的穿透性皮層分支供應(8,49)。SCA供血區域被認為是最容易因後窩血流減少而受損的區域,因為它代表了椎體和基底動脈的遠端交界(49)。在椎動脈或基底動脈閉塞後,SCA不閉塞時可發生梗死。
小腦後窩的病變擴大,導致小腦上表麵通過小腦幕開口的吻側突起,從而使小腦後窩及其分支向小腦幕邊緣伸展。蚓壁的表麵和側葉的鄰近部分被幕的遊離邊緣開槽,因此SCA的分支可能被壓縮。供給區小腦皮層的對稱軟化將會導致,在深支供給區的齒狀核中也可能發現類似的變化(46)。
SCA在處理涉及小腦、後海綿竇、腦幕切骨和橋小腦角的腫瘤時暴露;動脈瘤起源於顱底尖、SCA和PCA的起源處,雖然罕見,但也出現在遠端SCA;較少用於處理動靜脈畸形;三叉神經血管減壓術治療三叉神經痛在後顱窩缺血的血運重建旁路手術中。
對累及SCA的病變選擇手術入路要求準確地確定所累及的動脈段。位於腦幹前部靠近起源處的病灶,與位於腦幹後部四叉腦池或小腦後腦裂處的病灶,需要采用不同的入路。唯一的幕上入路是顳部開顱術,將顳葉和枕葉抬高,並將幕幕分開和收放,以暴露SCA的起源、橋腦腦和小腦腦腦前和外側節段,以及皮質近端分支。將此入路向後延伸至四叉腦池通常需要閉塞一些引流於顳葉和枕葉下表麵的靜脈,有靜脈梗死和水腫的風險。通過幕上-幕下乙狀竇前入路和幕下分裂可獲得類似甚至更大的SCA暴露,但這是一個更廣泛的手術。當以上述任何一種入路切開幕幕時,必須小心防止穿過橋腦外側段和幕幕邊緣之間的滑車神經受傷。SCA起點,以及基底脊尖,如果位於鞍背上方,可通過翼點開顱術和Liliequist膜的開口到達。經翼點路徑暴露低SCA原點可能需要打開海綿竇硬腦膜頂,即所謂的經海綿竇入路,並切除後床突和鞍背上部。在顳下前石壁切開入路中切除岩尖也有助於暴露低SCA起源,如果不能通過分割幕來暴露的話。通過垂直的枕下外側切口並延伸到橫竇和乙狀竇邊緣的枕下側側顱骨切除術,或如本文作者所喜歡的,可以很好地暴露三叉神經區域和小腦後裂前部的SCA。 This approach provides satisfactory exposure of the lateral pontomesencephalic segment, but not of the origin or of other segments. An infratentorial- supracerebellar approach directed through a suboccipital craniectomy provides satisfactory exposure of the cortical branches, but not those within the depths of the cerebellomesencephalic fissure or lateral to the brainstem. The occipital transtentorial approach provides a more favorable angle for exposing the branches ipsilateral to the craniotomy near the midline, below the pineal within the cerebellomesencephalic fissure, and in the posterior part of the ambient cistern.
AICA穿過橋小腦角的中心部分,靠近麵神經和前庭耳蝸神經(圖2.5和2.11)。在橋小腦角、基底動脈或椎動脈、斜坡、第四腦室和小腦的手術入路,以及通過顳骨和枕骨的入路中,它或它的分支可能暴露。
AICA與橋腦、側隱窩、Luschka孔、橋小腦裂、小腦中梗和小腦岩麵密切相關(圖2.1-2.3和2.11)。AICA起源於基底動脈,通常是一個單一的主幹,環繞橋腦橋附近的外展神經、麵神經和前庭耳蝸神經。在向進入聽覺通道的神經和從Luschka孔伸出的脈絡膜叢靠近並發送分支後,它繞過小腦中梗上的小葉,供應橋小腦裂的唇部和岩麵。它通常在麵部-前庭耳蝸神經複合體附近分叉,形成吻側幹和尾側幹。吻側幹的分支沿小腦中段向外側延伸至上側
橋小腦裂的唇部和岩麵的毗連部分,尾幹供應岩麵的下部,包括部分小葉和脈絡膜叢。AICA形成了通向腦幹的穿通動脈、通向端部和脈絡膜叢的脈絡膜分支以及與神經相關的動脈,包括迷路動脈、循環穿通動脈和弓狀下動脈(34)。
AICA分為四個節段:橋前節段、橋外側節段、絮結節段和皮質節段。每個節段可包括一個以上的主幹,這取決於動脈分叉的水平(圖2.1)。
這一段位於斜坡和腦橋的腹部之間,從原點開始,到穿過下橄欖長軸的一條線的水平處結束,並向上延伸到腦橋。這個節段通常與外展神經的小根接觸。
這一段開始於腦橋的前外側緣,經過麵神經和前庭耳蝸神經上麵、下麵或中間的橋小腦角,與內聽覺通道、側隱窩和從Luschka孔突出的脈絡叢密切相關(圖2.11和2.12)。這個節段產生神經相關的分支,在內部聽道附近或內部運行,與麵神經和前庭耳蝸神經密切相關。根據它們與內聲口氣孔的關係,這一段被分為口前、口和口後部分(圖2.5)。這些神經相關的分支是迷路動脈,供應麵神經、前庭耳蝸神經和前庭耳蝸迷宮;循環穿通動脈,它通向入口,但向內側轉向供應腦幹;還有弓下動脈,它進入弓下窩。此節段通常在橋髓連接處以下,特別是在它是彎曲的情況下。
這一段開始於動脈經過小葉的吻側或尾側,到達小腦中梗和橋小腦裂(圖2.11)。沿著花序梗的主幹可能隱藏在小葉或橋小腦裂的唇部。
這部分主要供給岩石表麵。

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.11。AICA關係。腦幹和右側岩狀小腦表麵的前外側視圖。右耳蝸脊經過外展肌下方,在麵神經和前庭耳蝸神經之間,然後到達橋小腦裂和小腦岩麵。B,右髂脊起於椎基底連接處上方,穿過橋髓連接處下方,然後向上延伸至小腦中踝表麵。它穿過絮凝體上方,沿著橋小腦裂到達岩麵。C和D,小腦和腦幹被切除,以顯示aica與顱神經和內聽道的關係。C,左鼻翼間區經過外展神經的上方和麵神經和前庭耳蝸神經的下方,在那裏形成腦幹的循環穿孔支。SCA穿過三叉神經後根上方。D,右耳蝸袢進入入口孔,在麵神經和前庭耳蝸神經之間。 E, another brainstem and cerebellum. The right vertebral artery is a duplicate artery and gives rise to duplicate PICAs. The AICAs arise from the lower part of the basilar artery. The left AICA is larger than the right. The rostral duplicate PICA loops upward into the cerebellopontine angle. The left vertebral artery loops upward into the left cerebellopontine angle. A., artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; Bas., basilar; Caud., caudal; Cer. Pon., cerebellopontine; CN, cranial nerve; Dup., duplicate; Fiss., fissure; Flocc., flocculus; For., foramen; Mid., middle; P.C.A., posterior cerebral artery; Ped., peduncle; Perf., perforating; P.I.C.A., posteroinferior cerebellar artery; Pon., pontine; Rec., recurrent; Rost., rostral; S.C.A., superior cerebellar artery; Sp., spinal; Tent., tentorial; Vert., vertebral.

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.12。AICA關係。前視圖。切除斜坡及鄰近的枕骨和顳骨,露出腦幹前部、椎動脈和基底動脈、右側內聽道的麵神經和前庭耳蝸神經,以及右側舌下管中的舌下神經。左鼻竇袢進入入口孔。B,右側橋小腦角放大圖。AICA通過麵神經和前庭耳蝸神經之間。舌下神經在椎動脈的後表麵周圍伸展。椎動脈向上彎入橋小腦角,異食癖發生於此,與麵神經根出口區密切相關,是麵肌痙攣的常見表現。一個迷宮般的動脈起源於AICA。 C, another enlarged view of the right cerebellopontine angle. The labyrinthine artery passes laterally with the facial nerve. The PICA loops upward and contacts the lower margin of the facial nerve. The vein of the cerebellopontine fissure ascends to empty into the superior petrosal sinus. D, the left AICA passes below the abducens, facial, and vestibulocochlear nerves and loops into the porus where it gives off two labyrinthine branches. Some of the hypoglossal rootlets are stretched over the PICA. The posterior trigeminal nerve was divided behind Meckel’s cave. The proximal stump arises from the midpons and the distal portion enters Meckel’s cave. A., artery; Ac., acoustic; A.I.C.A., anteroinferior cerebellar artery; Cer. Pon., cerebellopontine; CN, cranial nerve; Fiss., fissure; Labyr., labyrinthine; Pet., petrosal; P.I.C.A., posteroinferior cerebellar artery; Prox., proximal; S.C.A., superior cerebellar artery; Sup., superior; V., vein; Vert., vertebral.
AICA通常以單一血管的形式起源於基底動脈,但也可能以雙(重複)或三(重複)動脈的形式出現(圖2.2、2.3和2.11)。它可以發生在基底動脈的任何一點,但最常見的發生在下半部分。從一邊到另一邊的起源水平經常不對稱,其中一個顯著高於另一個的水平。在我們之前的研究中,我們發現在50個aica中,72%出現在單一幹線中,26%出現在兩條(重複)動脈中,2%出現在三條(重複)動脈中(34)。從它的起源,AICA課程向後繞過橋,向CPA。它的近端與外展神經的背側或腹側接觸。在經過外展神經後,它繼續前進到CPA,在那裏,它的一個或多個主幹與麵神經和前庭耳蝸神經密切相關,因此被稱為神經相關。
作為單一主幹產生的aica通常分為吻側主幹和尾側主幹。重複AICA被稱為吻側和尾側重複AICA,其分布類似於單個AICA分叉形成的吻側和尾側主幹的分布。大約三分之二的人在穿過麵神經和前庭耳蝸神經之前分叉,三分之一的人在穿過麵神經和前庭耳蝸神經之後分叉。靠近分叉的段為主幹,由分叉形成的兩條主幹分別為吻側主幹和尾側主幹。如果分叉靠近麵神經和前庭耳蝸神經,則吻側幹或分叉後幹都可能與神經有關。吻側重複aica比尾側重複aica更易產生神經相關的分支。重複aica的主幹也通常分叉,形成吻側主幹和尾側主幹,向小腦發送分支。
吻側幹穿過神經後,通常在小葉的上方向外側移動,到達小腦中梗的表麵和岩裂,分布到橋小腦裂的上唇和岩麵的鄰近部分。尾側幹常與第四腦室的外側部分相連。如果分叉靠近麵神經和前庭耳蝸神經,則尾幹向小葉尾部延伸,支配岩麵下部,包括部分小葉和脈絡膜叢。如果分岔在神經的遠端,尾側幹在橋小腦裂的下肢後方,靠近Luschka孔。尾幹經常進入小腦延髓裂的外側部分,就在外側隱窩的下方,然後向外側轉向供應岩麵的下部。尾側幹遠端分支常與異食尼卡吻合,吻側幹遠端分支常與SCA吻合。AICA形成了通往腦幹的穿通動脈、通往脈絡膜叢外側段的脈絡膜分支,以及上述的神經相關動脈。
與神經相關的分支是在入口孔內或附近、麵神經和前庭耳蝸神經附近的分支(圖2.5和2.11-2.14)(34)。每個神經相關的節段由一個或兩個動脈幹組成。一個是最常見的。單個與神經相關的節段由主主幹或吻側主幹形成,按頻率遞減順序,分別由單個AICA、吻側重複AICA或尾側重複AICA產生。雙節段是由兩種解剖結構中的一種產生的:a)單個AICA或一個重複AICA的吻側和尾側主幹都與神經相關,或b)每個重複AICA的一個主幹或三個重複AICA中的兩個的一個主幹與神經相關。
這一段從基底動脈開始,繞過腦幹到達麵神經和前庭耳蝸神經和入口的前緣。口前段由一條或兩條動脈幹組成。在我們檢查的50名注冊醫師中,有56個神經相關的入口前節段,44名注冊醫師(88%)有單獨的入口前節段,6名注冊醫師(12%)有雙入口前節段(34個)。大部分的口前節段,56個中有46個位於神經的前下。其餘位於神經前、下或前上(圖2.14)。
這段位於內耳道附近,常形成一個側向凸環,即內側環,指向或穿過耳道。大約一半的注冊會計師的內側段位於孔的內側,在另一半的注冊會計師的內側段形成一個環,到達孔或突出到管中。Sunderland和Mazzoni分別在64和67%的注冊會計師中發現孔內或管內的入口段(36,51)。Mazzoni發現,33%的入口段位於孔的內側,27%的入口段到達孔,40%的入口段進入管,很少超過管的內側一半(36)。
在50名注冊會計師的檢查中,我們發現有59個神經相關的耳節;41名注冊會計師(82%)有一個,9名注冊會計師(18%)有兩個齶節。大部分耳段位於麵神經和前庭耳蝸神經的下方或之間(圖2.14)。由於在三個cpa中,一個入口前節段在神經附近分叉,產生兩個與神經相關的入口節段,因此比入口前節段多出三個。大部分的耳袢在神經上方或下方的水平麵上,但也有一些,主要是在麵神經和前庭耳蝸神經之間,在垂直或斜平麵上。
在一些cpa中,與神經相關的環路形成了第二個橫向凸曲線,使環路呈“M”形。這第二個環被稱為弓下環,因為它指向弓下窩,一個在骨上的小凹口。這個環位於前庭耳蝸神經的後、後下或後上。在弓狀下動脈隆起處,動脈袢頂端偶爾與硬腦膜附著。
這段神經從神經的遠端開始,向內側延伸,供應腦幹和小腦。在我們之前對50名注冊會計師的研究中發現的59個齒段導致了60個齒後節段;80%的注冊會計師有一個,10個(20%)有兩個產後節段。由於一個口節分叉形成兩個口後節,故口後節比口段多一個。鼻後節段最常見的是神經後下、上、後或神經之間(圖2.14);沒有一個在神經前麵。形成雙節段的每條血管可能沿著與神經相關的相似或不同的路徑。

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.13。右CPA中A、AICA關係經乙狀竇後法分析。AICA在麵神經和前庭耳蝸神經之間橫向穿過,並向內側轉向,沿小腦中梗和橋小腦裂前進。三叉神經後方有一條巨大的岩上靜脈,有多條支流,包括橋三叉神經、橋橫靜脈和橋小腦裂靜脈。小葉隱藏了麵神經和前庭耳蝸神經與腦幹的連接處。B,小葉和脈絡膜叢,從Luschka孔突出,已經被抬起,暴露麵神經和前庭耳蝸神經與腦幹的連接處,在那裏麵神經在前庭耳蝸神經下麵。AICA分支由弓下動脈和迷宮動脈組成。C,解剖器抬高前庭耳蝸神經以更清楚地確定麵神經與腦幹的交界處。麵神經與腦幹的連接處較容易暴露於前庭耳蝸神經下方而非上方。D口後壁已被切除露出了口內壁的硬腦膜。 E, the meatal dura has been opened and the vestibulocochlear nerve displaced downward to expose the facial nerve coursing anterior and superior within the meatus. The nervus intermedius, which arises on the anterior surface of the vestibulocochlear nerve and passes laterally to join the facial nerve, is composed of several rootlets, as is common. F, the cleavage plane between the superior and inferior vestibular nerves has been developed. The cochlear nerve is located anterior to the inferior vestibular nerve. A., artery; A.I.C.A., antero- inferior cerebellar artery; Cer. Mes., cerebellomesencephalic; Cer. Pon., cerebellopontine; Chor., choroid; CN, cranial nerve; Coch., cochlear; Fiss., fissure; Flocc., flocculus; Inf., inferior; Intermed., intermedius; Labyr., labyrinthine; N., nerve; Nerv., nervus; Pet., petrosal; P.I.C.A., posteroinferior cerebellar artery; Plex., plexus; Pon., pontine; S.C.A., superior cerebellar artery; Subarc., subarcuate; Sup., superior; Trans., transverse; Trig., trigeminal; V., vein; Vest., vestibular.
![圖2.14。神經相關動脈與橋小腦角神經的關係圖。神經的方向如圖腦幹右側中央圖所示。三叉神經起源於腦橋。麵神經、前庭耳蝸神經和中間神經的方向如圖所示。上動脈、前上動脈等術語是指動脈和神經的關係。在50名注冊會計師中發現的動脈和動脈節段的數量是根據它們與神經的位置關係列出的。最常見的部位為口前段、下前段;道的段差;posteroinferior postmeatal段; internal auditory artery origin and course, inferior and anteroinferior; recurrent perforating artery origin, inferior and anteroinferior, and course, superior and between; and subarcuate artery origin, posterior, and course, posterosuperior. (From, Martin RG, Grant JL, Peace DA, Theiss C, Rhoton AL Jr: Microsurgical relationships of the anterior inferior cerebellar artery and the facial-vestibulocochlear nerve complex. Neurosurgery 6:483–507, 1980 [34].) c., course; I.A.A., internal auditory artery; Mea., meatal; o., origin; R.P.A., recurrent perforating artery; S.A., subarcuate artery; Seg., segment.](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Infratentorial_2.14.jpg)
圖2.14。神經相關動脈與橋小腦角神經的關係圖。神經的方向如圖腦幹右側中央圖所示。三叉神經起源於腦橋。麵神經、前庭耳蝸神經和中間神經的方向如圖所示。上動脈、前上動脈等術語是指動脈和神經的關係。在50名注冊會計師中發現的動脈和動脈節段的數量是根據它們與神經的位置關係列出的。最常見的部位為口前段、下前段;道的段差;posteroinferior postmeatal段; internal auditory artery origin and course, inferior and anteroinferior; recurrent perforating artery origin, inferior and anteroinferior, and course, superior and between; and subarcuate artery origin, posterior, and course, posterosuperior. (From, Martin RG, Grant JL, Peace DA, Theiss C, Rhoton AL Jr: Microsurgical relationships of the anterior inferior cerebellar artery and the facial-vestibulocochlear nerve complex. Neurosurgery 6:483–507, 1980 [34].) c., course; I.A.A., internal auditory artery; Mea., meatal; o., origin; R.P.A., recurrent perforating artery; S.A., subarcuate artery; Seg., segment.
在經過CPA的過程中,與神經相關的主幹發出四個分支(圖2.12-2.14):1)迷路(內耳)動脈,進入內耳道到達內耳;2)再循環穿通動脈,從發端向內側向腦幹供血;3)弓下動脈,通過弓下窩到達弓下管;4)小腦弓狀下動脈,其末端有一條分支通往弓狀下管,另一條分支通往小腦。
這些動脈是AICA的一個或多個分支,它們進入內耳道,並將分支發送到內耳道內襯的骨和硬腦膜,發送到內耳道內的神經,並最終形成供應內耳器官的前庭動脈、耳蝸動脈和前庭耳蝸動脈(圖2.12-2.14)(34)。
迷宮式動脈幾乎總是起源於AICA或它的一個分支,盡管有少數報道起源於基底動脈。在一項研究中,多達17%的腫瘤起源於基底動脈(40,51,56)。我們認為,這一差異是由不同研究中使用的內聽動脈和AICA定義的差異所解釋的。在本研究和Adachi和Fisch的研究中,將分支發送到內耳道的動脈基底動脈的起源幹,如果它將分支發送到小腦,盡管很小,被稱為AICA。內聽動脈的起源地被定義為內耳道的分支從傳導分支至小腦的AICA幹起的點(1,13)。另一方麵,如果進入入口的分支比到達小腦的分支大,Nager和Sunderland將來自基底動脈的主幹稱為迷路動脈而不是AICA(40,51)。Adachi和Fisch沒有發現任何由基底動脈產生的內聽動脈,但他們總能在進入入口的血管上發現一個小的小腦分支(1,13)。Mazzoni報道,在少數病例中,內聽動脈起源於異食癖(36),這一發現在我們的研究和上麵提到的其他研究中都沒有得到證實。在我們的研究中,30%的注冊會計師有一條內聽動脈,54%有兩條,14%有三條,2%有四條。
在我們研究中發現的94條內聽動脈中,50名注冊會計師中,72條(77%)來自產前段,20條(21%)來自產前段,2條(2%)來自產後段(34)。在每個存在後一個弓狀回環的CPA中,它們出現在近弓狀回環的位置。54%來自單個AICA, 23%來自重複或重複AICA, 23%來自複發性穿通動脈。Mazzoni和Hansen還指出,內聽動脈可能起源於反複的穿通動脈、弓狀下動脈或小腦弓狀下動脈(37)。
根據與耳道的關係,內耳動脈被分為兩組大小差不多的動脈。一組起源於耳孔內側,另一組起源於耳孔或在耳道內。從孔內側產生的最常起源於神經前、前或下。Fisch注意到,內聽動脈經常通過孔的前下緣進入耳道(13)。發源於孔或管內的最常見的發源於神經的下側或前側。
這些穿通動脈起源於與神經相關的血管,通常從它們的起點向入口移動,在沿麵神經和前庭耳蝸神經循環到達腦幹之前,偶爾會進入入口(圖2.5和2.14)。它們將分支發送到這些神經和這些神經進入區周圍的腦幹。它們也按頻率遞減的順序發送分支到小腦中段和橋腦的鄰近部分,三叉神經入口區周圍的橋腦,CPA的脈絡膜叢,上外側髓質,舌咽神經和迷走神經。約四分之一的內聽動脈和10%的弓狀下動脈由循環穿通動脈構成。
在我們的研究中,41名注冊會計師(82%)存在複發性穿通動脈;37名注冊會計師中有1人(74%),3人中有2人(6%),1人中有3人(2%)(34人)。大部分來自於出生前節,但也來自於出生前節和出生前節。它們與麵神經和前庭耳蝸神經的關係有顯著的變異性。大多數起源於下神經、前下神經或前神經或神經之間,並在神經之間或神經上方或神經下方向內側延伸(圖2.14)。
弓下動脈通常起源於孔內側,穿過覆蓋弓下窩的硬腦膜,進入弓下管(圖2.13和2.14)。在少數情況下,它起源於內耳道。起源於耳道的弓狀下動脈通過兩條路徑中的一條到達耳道;有些經孔循環到達弓下窩,有些則穿過口管壁到達弓下管。動脈供應半規管區域的岩骨(43)。弓狀下管被認為是感染從乳突區延伸到腦膜和岩上竇的潛在途徑(40)。在少數cpa中,弓下動脈起源於弓下窩的硬腦膜上附著AICA。
在我們的研究中,50名注冊會計師中有36人(72%)存在弓形下動脈;13例(26%)來自產前段,2例(4%)來自產前段,21例(42%)來自產後段(34例)。當存在時,隻有一個弓下動脈。大多數起源於神經後上,延伸至弓下窩。起源於麵神經的前、下或前下,穿過麵神經和前庭耳蝸神經的下方,到達弓下窩(圖2.14)。
Nager注意到,在對該區域動脈的描述中很少提及弓狀下動脈(40)。這可能是因為當大腦從頭骨中取出時,動脈及其與骨頭的連接被破壞了。Nager發現其最常見的發源部位是迷路動脈而不是AICA,這一差異可以用前麵提到的AICA和內聽動脈的定義不同來解釋(40)。他報告說弓下動脈也可能有雙重起源;其中一個分支可穿過弓下窩進入弓下管,另一個分支可穿過內耳道壁到達弓下管。
據Mazzoni(37)報道,小腦弓下動脈是AICA的一個小分支,它的一個分支通向弓下窩,另一個分支通向小腦。它通常起源於近端的口環,經過麵部神經和前庭耳蝸神經的下方,然後向上外側延伸到達弓下窩。在小腦窩處,它形成弓形下動脈,並向內側轉向供應小腦。我們調查的4名注冊會計師中存在弓形下小腦動脈(34名)。動脈起源於進入入口的神經的前下方或下方。小腦支在小葉上終止,在小葉下麵的鄰近小腦皮層上終止。
最常見的模式是AICA供給岩石表麵的大部分,但供給的皮質區域變化很大(圖2.11)。它可以從小葉上的一小塊區域和岩麵的鄰近部分變化到包括整個岩麵和幕麵和枕下麵的鄰近部分。吻側幹穿過神經後,通常向小葉上方延伸至橋小腦裂上唇,尾側幹向小葉末端延伸至岩麵下部。如果異食癖缺失,尾幹可支配幾乎所有同側枕下半球和蚓部。SCA在岩石表麵的上部重疊,PICA在枕下表麵的外側重疊並不少見。
AICA的閉塞導致的綜合征主要與腦幹和小腦梗的外側部分軟化有關,而不是與小腦半球受累有關,包括由神經及其核受累引起的麵神經和前庭耳蝸神經麻痹;前庭神經核及其與迷走神經核連接處的病變引起的眩暈、惡心、嘔吐和眼球震顫;三叉神經脊髓束和神經核中斷引起同側麵部痛覺、溫覺喪失和角膜感覺減退;腦橋和髓質外側的瞳孔擴張下行纖維中斷引起的霍納氏綜合征;小腦性共濟失調和精神障礙歸因於小腦梗的病變;身體對側半部分疼痛和溫度感覺的不完全喪失(完全對側痛覺減退的缺乏是由於病變的極端外側和後部位置造成的,這保留了脊髓丘腦外側束的一部分)(2,3)。由於AICA的可變性,其閉塞引起的所有綜合征都是不相同的。症狀通常是突然發作,不伴有意識喪失(2)。最突出的症狀是眩暈,常伴有惡心和嘔吐,其次是麵癱、耳聾、感覺喪失和小腦障礙。值得注意的是,皮質脊髓束和內側丘係受累的征象是由椎體和基底動脈的中線支滋養的。
術中有意阻斷AICA後,許多患者的恢複和存活歸功於來自其他小腦動脈的側支循環的充分性(34)。AICA閉塞後梗死區域的大小與PICA和SCA的大小以及與這些動脈的吻合口的大小呈負相關。如果異尼卡異常小而AICA很大,側支循環很可能很差,在AICA閉塞的情況下造成不利和危險的情況。切除腫瘤時使用的大腦牽開器所引起的機械刺激引起的動脈痙攣可能使側支供應的效力減弱。
在橋小腦角腫瘤的手術中,AICA最常暴露。動脈瘤累及AICA是罕見的,如果不在起源處,則極有可能位於內聲口或附近(25,31)。與聽神經瘤相關的神經動脈的移位和處理在橋小腦角一章中有更詳細的回顧。位於幕下的動靜脈畸形較幕上部位少見,而且除了AICA和腦幹外,也常累及其他小腦動脈,因此增加了處理風險(9,39,44)。被彎曲的動脈壓迫的麵神經和前庭耳蝸神經被認為是導致這些神經功能障礙的原因,這個概念在第四章關於橋小腦角(18,19,34)中進行了綜述。
可通過枕下外側(乙狀竇後)、中窩、經迷路或幕上-幕下乙狀竇前聯合入路入路進入AICA。枕下暴露對於涉及到AICA的口及口後節段、三叉神經下中下腦幹外側部和內聽道附近區域的病變是極好的。顳下中窩入路,切開幕幕,可能結合內側岩石切開術,可用於AICA起源高的病變,或同時累及SCA和基底動脈並位於三叉神經內側的病變。在中窩入路至內入口時,隻有位於入口附近的一小段動脈露出來,有時隻有當動脈袢進入內入口的時候才露出來。經迷路入路暴露AICA,在內聽道近端和遠端一小段距離內及沿岩麵前部。對於位於腦幹前方較深處的病變,特別是位於AICA起源附近的病變,可選擇幕上下乙狀竇前入路,對半規管、前庭和耳蝸進行不同程度的切除。隻有當鼻竇起源靠近中線時,鼻竇起源才可能在直接通過斜坡的前入路中暴露,但如果鼻竇起源來自彎曲的基底動脈,該基底動脈向外側循環進入橋小腦角,位於海綿竇和頸岩的內側,這限製了鼻竇前池的外側暴露範圍。
異食癖是小腦動脈最複雜、曲折和多變的供血路線和區域。在大孔、第四腦室、小腦半球、腦幹、頸靜脈孔、橋小腦角、岩尖和斜坡的手術入路中可能暴露(30)。
異食癖與小腦延髓裂、腦室頂下半部分、小腦下梗和枕下表麵密切相關(圖2.1- 2.5)。根據定義,異食癖起源於靠近下橄欖的椎動脈,並向後繞過髓質。在延髓的前外側緣,它通過舌下神經的細根的吻側或尾側或之間,在延髓的後外側緣,它通過舌咽神經、迷走神經和副神經的絲的吻側或之間。經過後麵的神經後,它繞著小腦扁桃體進入小腦髓裂後經過第四腦室頂部的下半部分。出小腦延髓裂時,其分支分布於枕下麵的蚓部和半球。它的供血區域是小腦動脈中最易變的(26)。大多數pica分為內側主幹和外側主幹。內側幹供應扁桃體和腦半球的鄰近部分,外側幹供應扁桃體和腦半球的皮質表麵。異食尼卡發出穿孔動脈、脈絡膜動脈和皮層動脈。皮質動脈分為蚓動脈組、扁桃體動脈組和半球動脈組。

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.15。A和b異食癖的片段。劣質的視圖。左側扁桃體在扁桃體梗的水平被切除,扁桃體梗與腦半球其餘部分的連接位置。髓前段(綠色)從椎動脈起點延伸到下橄欖。這段位於舌下神經的細根的吻側或尾側或之間。外側髓段(橙色)從橄欖樹最突出的部分延伸到舌咽神經、迷走神經和副神經的根的水平。扁桃體髓段(藍色)從扁桃體尾半部分周圍的後端神經水平延伸,常形成尾側凸環。端速扁桃體段(黃色)從扁桃體中段延伸到位於脈絡膜背、上下髓質膜和下扁桃體上極之間的裂口出口。皮質段(紅色)從動脈及其分支出扁桃體、蚓部和腦半球之間的裂隙處延伸至皮質表麵。 The bifurcation of the main trunk into medial and lateral trunks is often located at the level of the tonsillomedullary or the telovelotonsillar segments. The medial trunk gives rise to median and paramedian vermian arteries. The lateral trunk gives rise to lateral, intermediate, and medial hemispheric and tonsillar arteries. B, enlarged posterior view. The left and part of the right halves of the cerebellum was removed to show the relationship of the PICA to the roof of the fourth ventricle. The dentate nucleus wraps around the superior pole of the tonsil. The telovelotonsillar fissure is below the inferior half of the roof of the fourth ventricle between the tonsil, tela choroidea, and inferior medullary velum. The caudal loop of the PICA is near the caudal pole of the tonsil, and the cranial loop is above the rostral pole of the tonsil. A., artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; B.A., basilar artery; Cer., cerebellar; Ch., choroid; Coll., colliculus; F., foramen; Fiss., fissure; He., hemispheric; Inf., inferior; Int., intermediate; Lat., lateral; Med., medial, medullary; Mid., middle; Nucl., nucleus; Paramed., paramedian; P.C.A., posterior cerebral artery; Ped., peduncle; Pl., plexus; S.C.A., superior cerebellar artery; Seg., segment; Sup., superior; Ton., tonsillar; Tr., trunk; V.A., vertebral artery; Ve., vermian; Vel., velum.
![圖2.15。C和d異食癖的片段。C,側麵圖。髓前段經過舌下神經吻側。側髓段通過附屬細枝之間。扁桃體髓段在扁桃體下極附近形成一個顱凸環。端速扁桃體段形成顱凸環,並在其末端附近分叉為內側主幹和外側主幹。皮質段橫跨枕下表麵。D,矢部分。扁桃體髓和端速扁桃體段將脈絡膜分支送入脈絡膜叢。 The telovelotonsillar segment ascends between the nodule and uvula medially and the tonsil laterally. (From, Lister JR, Rhoton AL Jr, Matsushima T, Peace DA: Microsurgical anatomy of the posterior inferior cerebellar artery. Neurosurgery 10:170–199, 1982 [30].)](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_Book_-_Posterior_Fossa/Figure_2.15_C-D.png)
點擊這裏查看此圖像的交互模塊和相關內容。
圖2.15。C和d異食癖的片段。C,側麵圖。髓前段經過舌下神經吻側。側髓段通過附屬細枝之間。扁桃體髓段在扁桃體下極附近形成一個顱凸環。端速扁桃體段形成顱凸環,並在其末端附近分叉為內側主幹和外側主幹。皮質段橫跨枕下表麵。D,矢部分。扁桃體髓和端速扁桃體段將脈絡膜分支送入脈絡膜叢。 The telovelotonsillar segment ascends between the nodule and uvula medially and the tonsil laterally. (From, Lister JR, Rhoton AL Jr, Matsushima T, Peace DA: Microsurgical anatomy of the posterior inferior cerebellar artery. Neurosurgery 10:170–199, 1982 [30].)
PICA分為五個部分:1)前髓質,2)外側髓質,3)扁桃體髓質4)端速扁桃體,5)皮質(圖2.1和2.15)。這些節段通常比圍繞髓質或扁桃體的距離長,因為異動性腦血管病的過程經常是曲折的,並在腦幹一側下部顱神經之間、扁桃體附近和第四腦室頂部尾部形成複雜的環。每個節段可能包括一個以上的主幹,這取決於動脈分叉的水平。
這段位於髓質的前方。它開始於髓質前方異食膜的起源處,向後延伸,越過舌下小根,通過下橄欖最突出的部分到達後尾線的水平,下橄欖是髓質前表麵和外側表麵之間的分界線。那些發生於髓質外側而不是髓質前方的pica沒有髓質前段。如果異食癖發生於椎動脈的上部,則更有可能出現前髓段,因為椎動脈從下麵的髓質外側延伸到上麵的髓質前表麵。如果異食癖起源水平的椎動脈已通過腦幹前表麵,則存在前髓質段。從它的起源開始,異食癖通常向後繞過舌下小根或在兩者之間,但偶爾在向後繞過舌下小根或在舌下小根之間之前向上、向下、橫向或中間循環。
這一段開始於動脈經過橄欖最突出的地方,結束於舌咽部、迷走神經和附屬小根的起源水平。這個片段存在於大多數pica中。它的路徑各不相同,有的直接經過腦幹後方到達舌咽神經、迷走神經和附屬小根,有的上升、下降,有的橫向或內側穿過,在腦幹一側的腦池中形成一個或多個複雜的循環,然後在這些神經之間穿過。

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.16。異食癖的關係。A,異食癖穿過髓質,進入小腦髓裂,並從裂出供應枕下表麵。裂縫向上延伸在一側的小腦扁桃體和另一側的髓質和腦室頂下半部分之間。pica常在小腦扁桃體的下極形成尾狀環。B,放大圖。左側扁桃體被切除,以暴露異食癖在小腦髓裂內的過程。pica通常繞著扁桃體吻端向上循環,在扁桃體吻端(下側)和脈絡膜端(上側)和下髓膜之間運動。C,切除扁桃體和雙側小葉的相鄰部分,暴露異食癖幹。pica分為內側幹和尾幹,內側幹提供蚓部和半球的鄰近部分,尾幹環繞扁桃體提供半球表麵的最大部分。 Choroidal branches pass to the tela choroidea and choroid plexus in the roof. The vein of the cerebellomedullary fissure crosses the tela and velum and passes above the flocculus to join the veins in the cerebellopontine angle that empty into the superior petrosal sinus. D, another dissection showing the relationship of the cranial loop of the PICA to the tonsils and inferior medullary velum. Both tonsils and the nodule and uvula have been preserved. The inferior medullary velum has been preserved on the right side. The left half of the inferior medullary velum has been removed to expose the supratonsillar loop of the PICA, which courses between the velum and the tonsil. The velum stretches laterally from the nodule across the rostral pole of the tonsil to blend into the flocculus. A., artery; A.I.C.A., antero- inferior cerebellar artery; Br., branch; Cer. Med., cerebellomedullary; Cer. Mes., cerebellomesencephalic; Chor., choroidal; CN, cranial nerve; Fiss., fissure; Flocc., flocculus; Inf., inferior; Lat., lateral; Med., medial, medullary; Mes., mesencephalic; P.I.C.A., posteroinferior cerebellar artery; S.C.A., superior cerebellar artery; Tr., trunk; V., vein; Vel., velum; Vent., ventricle; Verm., vermian; Vert., vertebral.
這一段始於異食癖神經經過舌咽神經、迷走神經和副神經的後方,並向內側延伸至扁桃體尾半部附近的髓質後部(圖2.3、2.4、2.15和2.16)。它在動脈上升到扁桃體內側表麵的中間位置結束。這段的近端部分通常在側隱窩附近,然後向後到達扁桃體的下極。這段通常在扁桃體下緣和髓質之間的內側穿過,然後沿著扁桃體的內側表麵向兩側轉向。經過扁桃體下部附近的袢稱為尾側或扁桃體下側袢,據報道形成與扁桃體尾極重合的尾側凸袢,但它也可能在扁桃體尾極上方或下方經過而不形成袢。在某些情況下,它會低於扁桃體尾部邊緣甚至低於枕骨大孔的水平。如果異食卡直接穿過扁桃體和髓質之間的內側,如果異食卡沿扁桃體外側表麵上升到達半球表麵,或者如果動脈從椎動脈起端較低,上升到髓質後方到達扁桃體,則不存在尾側凸環(圖2.17)。
扁桃體髓段與扁桃體小腦和枕骨大孔之間的關係不同(圖2.17)。在我們之前對42例pica的研究中,23例該節段的尾端極限位於扁桃體尾極之上,8例位於扁桃體下端,11例(30例)位於同一水平。此節段在扁桃體尾端上10.0 mm至上13.0 mm(平均上1.6 mm)的中間位置通過。在37例PICAs中,該節段尾緣高於枕骨大孔,4例低於枕骨大孔,1例處於同一水平。位於枕骨大孔上方18.0 mm(平均上方6.9 mm)下方7.0 mm處。
這是最複雜的部分。它開始於異尼卡突起的中段,沿著扁桃體的內側表麵向第四腦室的頂部延伸,結束於從蚓部、扁桃體和腦半球之間的裂隙流出,到達枕下表麵(圖2.15-2.18)。在大多數(但不是所有)腦半球中,這部分通常形成一個帶有凸吻側曲線的環,稱為顱環(20,38,57)。這個袢位於頂部尾部,位於下麵的小腦扁桃體和上麵的脈絡膜和後髓膜之間。顱環的頂端通常位於下髓膜的中心部位,但其位置從上緣到下緣,從下髓膜的內側到外側範圍不等。顱環的頂端在大多數情況下低於第四腦室頂的水平,但也可能延伸到頂的水平。這個節段形成了供給第四腦室的脈絡膜側和脈絡膜叢的分支。
這一段開始於主幹和分支離開內側蚓體和扁桃體之間的溝槽和外側半球之間的地方,包括皮層末端分支。異食癖的分叉常發生在這個節段的起源附近。皮質分支從扁桃體的上緣和外側緣向外輻射到蚓部和半球的其餘部分。
異食癖在這裏被定義為起源於椎動脈的小腦動脈(圖2.19和2.20)(49,55)。異食癖不常被定義為小腦後下動脈,它供應小腦後下部分,通常起源於椎動脈,但也可能起源於基底動脈(4,56)。
在我們之前的研究中檢查的50個小腦半球中,除1個外,其餘均有椎動脈,49個椎動脈中42個椎動脈引起PICAs(30個)。椎動脈和異食癖在幾個半球均不存在。如果發生異食癖,它是椎動脈最大的分支。罕見雙側異食癖缺失,但可能出現雙側或雙側異食癖。42個pica中有41個作為單一主幹出現,1個作為重複主幹出現。椎動脈有時會在異食癖中終止。
椎動脈在頸髓連接處外側進入硬腦膜,經過上、前、內三個方向,到達髓質前部,並在橋髓連接處與另一側的椎動脈彙合,形成基底動脈。異食癖起源於椎動脈的部位從枕骨大孔以下到椎基底連接處不等。少數起源於枕骨大孔下方的pica可能起源於硬膜外位置的椎動脈(圖2.21)(12)。在我們之前的研究中,42例pica中有35例發生在枕骨大孔以上,7例發生在枕骨大孔以下。起源位於枕骨大孔水平以下14.0 mm至26.0 mm(平均,8.6 mm以上)(30)。起源位於椎體和基底動脈交界處以下0 - 35.0 mm(平均16.9 mm)處。
異食癖發生於椎動脈的後表麵或外側表麵多於內表麵或前表麵(圖2.19)。離開母血管時,異食癖的起始路徑是後、外側或上,而不是前、內側或下(圖2.20)。椎動脈通過硬腦膜的入口直徑較大(範圍:1.8-6.2 mm;平均,4.4 mm)比異食癖起源處(範圍,1.6-5.7 mm;平均3.9毫米)或末端(範圍1.7-5.5毫米;平均3.7毫米)。PICA的直徑在其起源範圍從0.5到3.4毫米(平均2.0毫米)。4個小腦起源直徑小於1.0 mm。據報道,異食癖在5 - 16%的小腦半球存在發育不良(33,48)。
![圖2.17。異食癖分岔的位置,與扁桃體和枕骨大孔相關的尾側環,以及顱環。A,與扁桃體相關的分叉部位。異食癖的主幹可在扁桃體邊緣的任何部位分叉。下外側分支(紅色):外側幹向扁桃體外側向上穿過,到達半腦,內側幹沿扁桃體前內側緣穿過。內下分支(綠色):外側幹上外側穿過扁桃體後緣到達半球表麵,內側幹沿扁桃體前內側緣向上穿過。超內側分支(藍色):外側幹向後穿過扁桃體內側表麵,內側幹向上提供蚓部。上外側分支(黃色):外側幹從扁桃體和腦半球之間的裂隙中出來,並向前延伸至腦半球表麵,內側幹向上提供蚓部。B,尾袢與扁桃體的位置。扁桃體髓段在穿過髓質後表麵時,常形成尾側凸環(藍色、橙色、綠色)。 This caudal part of the tonsillomedullary segment was located between 10.0 mm inferior and 13.0 mm superior (average, 1.6 mm superior) to the caudal tip of the tonsil. This loop could be found superior to (orange), inferior to (green), or at the level of (blue) the caudal tip of the tonsil. In some cases (yellow), the PICA ascended from the vertebral artery (V.A.) or took another course to reach the medial surface of the tonsil without forming a caudal loop. C, relation of the caudal loop to the foramen magnum. Most caudal loops were superior to the foramen magnum (yellow), but they could be inferior to (red) or at the level of (green) the foramen magnum. The caudal loop was located between 7.0 mm inferior and 18.0 mm superior (average, 6.9 mm superior) to the foramen magnum. D, relationship of the cranial loop (arrow) to the superior pole of the tonsil and the trunks of the PICA. The right tonsil was removed at the level of the tonsillar peduncle to expose the inferior medullary velum and the tela choroidea. The telovelotonsillar segment often formed a cranially convex loop. below the fastigium. The cranially convex loop could be formed by either the main (green), medial (yellow), or lateral (blue) trunk. On the left (blue), the lateral trunk (arrow) forms a cranially convex loop over the superior pole of the tonsil and the medial trunk ascends straight to the vermis. In the center (yellow), the medial trunk (arrow) forms a cranially convex loop at the superior pole of the tonsil and the lateral trunk courses around the medial surface of the tonsil. On the right (green), the cranial loop is formed by the main trunk (arrow) and lies in the telovelotonsillar fissure anterior to the superior pole of the tonsil. (From, Lister JR, Rhoton AL Jr, Matsushima T, Peace DA: Microsurgical anatomy of the posterior inferior cerebellar artery. Neurosurgery 10:170–199, 1982 [30].) Inf., inferior; Lat., lateral; Med., medial, medullary; Ped., peduncle; Ton., tonsillar; Tr., trunk; V.A., vertebral artery; Vel., velum.](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_Book_-_Posterior_Fossa/Figure_2.17.png)
點擊這裏查看此圖像的交互模塊和相關內容。
圖2.17。異食癖分岔的位置,與扁桃體和枕骨大孔相關的尾側環,以及顱環。A,與扁桃體相關的分叉部位。異食癖的主幹可在扁桃體邊緣的任何部位分叉。下外側分支(紅色):外側幹向扁桃體外側向上穿過,到達半腦,內側幹沿扁桃體前內側緣穿過。內下分支(綠色):外側幹上外側穿過扁桃體後緣到達半球表麵,內側幹沿扁桃體前內側緣向上穿過。超內側分支(藍色):外側幹向後穿過扁桃體內側表麵,內側幹向上提供蚓部。上外側分支(黃色):外側幹從扁桃體和腦半球之間的裂隙中出來,並向前延伸至腦半球表麵,內側幹向上提供蚓部。B,尾袢與扁桃體的位置。扁桃體髓段在穿過髓質後表麵時,常形成尾側凸環(藍色、橙色、綠色)。 This caudal part of the tonsillomedullary segment was located between 10.0 mm inferior and 13.0 mm superior (average, 1.6 mm superior) to the caudal tip of the tonsil. This loop could be found superior to (orange), inferior to (green), or at the level of (blue) the caudal tip of the tonsil. In some cases (yellow), the PICA ascended from the vertebral artery (V.A.) or took another course to reach the medial surface of the tonsil without forming a caudal loop. C, relation of the caudal loop to the foramen magnum. Most caudal loops were superior to the foramen magnum (yellow), but they could be inferior to (red) or at the level of (green) the foramen magnum. The caudal loop was located between 7.0 mm inferior and 18.0 mm superior (average, 6.9 mm superior) to the foramen magnum. D, relationship of the cranial loop (arrow) to the superior pole of the tonsil and the trunks of the PICA. The right tonsil was removed at the level of the tonsillar peduncle to expose the inferior medullary velum and the tela choroidea. The telovelotonsillar segment often formed a cranially convex loop. below the fastigium. The cranially convex loop could be formed by either the main (green), medial (yellow), or lateral (blue) trunk. On the left (blue), the lateral trunk (arrow) forms a cranially convex loop over the superior pole of the tonsil and the medial trunk ascends straight to the vermis. In the center (yellow), the medial trunk (arrow) forms a cranially convex loop at the superior pole of the tonsil and the lateral trunk courses around the medial surface of the tonsil. On the right (green), the cranial loop is formed by the main trunk (arrow) and lies in the telovelotonsillar fissure anterior to the superior pole of the tonsil. (From, Lister JR, Rhoton AL Jr, Matsushima T, Peace DA: Microsurgical anatomy of the posterior inferior cerebellar artery. Neurosurgery 10:170–199, 1982 [30].) Inf., inferior; Lat., lateral; Med., medial, medullary; Ped., peduncle; Ton., tonsillar; Tr., trunk; V.A., vertebral artery; Vel., velum.

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.18。異食癖的關係。第一,小腦的右半部分被切除。右異食癖通過迷走神經和副神經的細根之間到達小腦下梗的表麵。左異食癖,由於它在扁桃體的吻端附近移動,被小舌剩下的左半邊所掩蓋。SCA穿過腦幹,在動眼神經下麵,三叉神經上麵。B,小舌的部分和扁桃體內側的結節已經被切除,暴露PICAs通道通過小腦髓裂和扁桃體周圍。動脈常在扁桃體下緣形成尾側袢,並在扁桃體吻側極周圍形成顱側或扁桃體上袢。C,扁桃體被切除,暴露異食癖通過小腦髓裂的循環過程。D,下髓質膜,它橫跨扁桃體的吻端,向下折疊露出齒狀結節,齒狀核下的齒狀突起。 The lateral recess is also exposed. The telovelotonsillar segment of the PICA courses in the cerebellomedullary fissure between the tela and velum on one side and the tonsil on the other side. Cer. Med., cerebellomedullary; Cer. Mes., cerebellomesencephalic; CN, cranial nerve; Cran., cranial; Dent., dentate; Fiss., fissure; Inf., inferior; Lat., lateral; Med., median, medullary; Mid., middle; Nucl., nucleus; Ped., peduncle; P.I.C.A., posteroinferior cerebellar artery; S.C.A., superior cerebellar artery; Sulc., sulcus; Sup., superior; Vel., velum.
![圖2.19。腦幹和小腦的下視圖(上)顯示了椎動脈周長(右下)上50個小腦半球中42個pica起源的位置。右下圓對應椎動脈的周長。50個小腦半球中有8個沒有異食癖。異食癖最常發生於椎動脈的後、後外側或外側表麵,但也有少數起源於動脈的前半部分或內半部分。(來自,Lister JR, Rhoton AL JR, Matsushima T, Peace DA:小腦後下動脈的顯微外科解剖。神經外科10:17 - 199,1982[30]。](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Infratentorial_2.19.jpg)
圖2.19。腦幹和小腦的下視圖(上)顯示了椎動脈周長(右下)上50個小腦半球中42個pica起源的位置。右下圓對應椎動脈的周長。50個小腦半球中有8個沒有異食癖。異食癖最常發生於椎動脈的後、後外側或外側表麵,但也有少數起源於動脈的前半部分或內半部分。(來自,Lister JR, Rhoton AL JR, Matsushima T, Peace DA:小腦後下動脈的顯微外科解剖。神經外科10:17 - 199,1982[30]。
![圖2.20。橋腦、髓質、椎動脈和基底動脈的前上(上)和前(下)視圖顯示了異食尼卡起始節段所采取的方向。在我們檢查的50個小腦半球中發現了42個pica。箭頭是開的,並定義pica的初始段所采取的方向,直接遠端於其原點。外展神經、麵神經和前庭耳蝸神經在橋髓連接處出現。舌咽神經、迷走神經和副神經起於下橄欖的後方,舌下神經起於下橄欖的前方。最初節段最常指向後、外側上、後外側或後內側。少數PICAS定向於上外側、下外側、前外側、後下、上內側、下內側或前。(來自,Lister JR, Rhoton AL JR, Matsushima T, Peace DA:小腦後下動脈的顯微外科解剖。神經外科10:17 - 199,1982[30]。 Ant., anterior; B.A., basilar artery; Inf., inferior; Lat., lateral; Med., medial; Post., posterior; Sup., superior; V.A., vertebral artery.](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Infratentorial_2.20.jpg)
圖2.20。橋腦、髓質、椎動脈和基底動脈的前上(上)和前(下)視圖顯示了異食尼卡起始節段所采取的方向。在我們檢查的50個小腦半球中發現了42個pica。箭頭是開的,並定義pica的初始段所采取的方向,直接遠端於其原點。外展神經、麵神經和前庭耳蝸神經在橋髓連接處出現。舌咽神經、迷走神經和副神經起於下橄欖的後方,舌下神經起於下橄欖的前方。最初節段最常指向後、外側上、後外側或後內側。少數PICAS定向於上外側、下外側、前外側、後下、上內側、下內側或前。(來自,Lister JR, Rhoton AL JR, Matsushima T, Peace DA:小腦後下動脈的顯微外科解剖。神經外科10:17 - 199,1982[30]。 Ant., anterior; B.A., basilar artery; Inf., inferior; Lat., lateral; Med., medial; Post., posterior; Sup., superior; V.A., vertebral artery.

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.21。起源於硬膜外的雙側PICAs。A,兩種pica都發生在硬腦膜外,因為椎動脈經過寰枕關節後方。pica在背外側髓質水平進入硬腦膜,沒有前髓質或完整的外側髓質段。左異食癖在寰椎後弓前向下循環。B,放大圖。左側異食癖發出腦膜後動脈,通過椎動脈周圍的硬腦膜套穿過硬腦膜,在副神經和C1和C2根後向下循環,然後上升進入小腦髓裂。右側異食癖穿過硬腦膜,沿副神經細根前的髓質側行。C,左側異食癖伴椎動脈和C1神經根穿透硬腦膜套。副神經通過椎動脈和異食癖後方。 The rostral attachment of the dentate ligament ascends between the PICA and the vertebral artery to attach to the dura at the level of the foramen magnum. D, the C1 nerve root passes through the dural cuff with the vertebral artery and the PICA. The accessory nerve ascends posterior to both the vertebral artery and PICA. A small posterior spinal artery arises from the PICA and courses along the dorsolateral aspect of the spinal cord. A., artery; Atl., atlanto; CN, cranial nerve; Dent., dentate; Lig., ligament; Men., meningeal; Occ., occipital; P.I.C.A., posteroinferior cerebellar artery; Post., posterior; Sp., spinal; Suboccip., suboccipital; Vert., vertebral.
大多數pica分叉成一個較小的內側主幹和一個較大的外側主幹;分叉前的主幹稱為主幹線。內側幹支配著蚓部和半球的鄰近部分,外側幹支配著枕下表麵的大部分半球和扁桃體部分。不分叉的pica通常很小,隻分布在扁桃體和蚓部和半球的鄰近部分的一小部分。
當異尼卡在扁桃體周圍運動時,分叉通常發生在腦幹後方(圖2.16、2.17和2.22)。最常見的分叉部位是扁桃體端速裂,因為動脈繞著扁桃體吻端極旋轉。內側幹通常在蚓半裂上升到達蚓麵,外側幹從端速扁桃體裂向外側穿過到達半球表麵。如果分叉發生在離扁桃體較近的位置,內側幹通常沿扁桃體內側表麵上升並通過蚓半裂,外側幹在分叉點附近經過扁桃體表麵後方到達半球表麵。如果分叉發生在扁桃體外側緣近端,內側幹通常沿著扁桃體內側表麵延伸至蚓-半球裂,外側幹直接到達扁桃體半球表麵。
內側幹的末端通過分支延伸到蚓部下部和扁桃體和半球的鄰近部分。外側幹分為較大的半腦幹,向扁桃體半球發出多個分支,較小的扁桃體分支分布在扁桃體的後表麵和下表麵。側幹分裂為扁桃體和半腦分支可能發生在與扁桃體有關的不同部位,但最常見的是位於扁桃體內側表麵的後緣附近。穿過扁桃體髓裂的主幹將分支發送到髓質,穿過端速扁桃體裂的主幹將上行分支發送到齒狀核(55)。
異貫性耳膜形成了貫穿髓質的分支,提供脈絡膜端和脈絡膜叢的脈絡膜動脈和皮層動脈。皮質動脈分為蚓中動脈和蚓中動脈;扁桃體;還有內側,中間和外側動脈。位於扁桃體上極附近的皮層分支向上提供齒狀核。

點擊這裏查看此圖像的交互模塊和相關內容。
圖2.22。異食癖的關係。A,左側異食癖比右側大。兩種pica進入小腦延髓裂,繞過扁桃體,然後從裂出供應枕下表麵。右扁桃體和雙側小葉之間的天然裂口已經打開。扁桃體通過扁桃體梗與小腦的其餘部分相連,扁桃體梗是一個沿著扁桃體上外側邊緣的白質束。扁桃體的其他邊緣都是遊離邊緣。B,放大圖。左雙腹小葉被抬高,露出從側隱窩邊緣突出的小葉。C,扁桃體向外側收縮,暴露在小腦髓裂中的PICAs。 The right PICA bifurcates into medial and lateral trunks before reaching the cerebellomedullary fissure. The left PICA bifurcates within the fissure. The medial trunks supply the vermis and adjacent part of the hemisphere and the lateral trunks supply the remainder of the hemisphere. D, the right tonsil has been removed to expose the lateral recess and bifurcation of the right PICA into medial and lateral trunks. E, both tonsils and the tela have been removed to expose the ventricular floor and walls. The left PICA divides into its trunks within the cerebellomedullary fissure. The inferior medullary velum has been preserved, but is a thin layer that can be opened, if needed, to increase the exposure of the fourth ventricle. F, enlarged view showing the relationship of the PICAs to the fourth ventricle. The PICAs, after passing between the rootlets of the accessory rootlets course along the caudolateral margin of the fourth ventricle on the inferior cerebellar peduncle before entering the cerebellomedullary fissure. The left PICA has been reflected laterally. The facial colliculus is in the upper and hypoglossal and vagal nuclei are in the lower part of the floor. Bivent., biventral; Br., branch; Cer. Med., cerebellomedullary; CN, cranial nerve; Coll., colliculus; Fiss., fissure; Flocc., flocculus; Hem., hemispheric; Hypogl., hypoglossal; Inf., inferior; Lat., lateral; Med., medial, medullary; Ped., peduncle; P.I.C.A., posteroinferior cerebellar artery; Suboccip., suboccipital; Tr., trunk; Trig., trigeminal; V., vein; Vel., velum; Vent., ventricle; Verm., vermian.
穿通動脈是由三個髓段產生的小動脈,終止於腦幹。它們分為直接型和回旋型。直接型沿著一條直線進入腦幹。旋回型繞過腦幹,最後到達腦幹。旋狀穿通動脈分為短型和長型。短旋狀腦幹繞腦幹周長不超過90度。長旋流型移動更大的距離到達對麵的表麵。兩種類型的旋動脈都在其運行過程中將分支送入腦幹。穿通動脈有許多分支和吻合,在髓質表麵形成網狀結構。在我們之前的研究中,前髓段每個半球產生0 - 2個(平均1.0)穿孔分支,這些分支最常見的是短旋後型,供應髓質的前、外側或後表麵(30)。 The lateral medullary segments gave rise to 0 to 5 (average, 1.8) branches per hemisphere that supplied the lateral or posterior medulla predominately as short circumflex arteries. The tonsillomedullary segment gave rise to more perforating branches than the other segments (range, 0–11 per hemisphere; average, 3.3). They were either of the direct or short circumflex type, but the former predominated. They terminated in the lateral and posterior surfaces of the medulla.
PICA的穿支與來自椎動脈的穿支混合並重疊(圖2.5)。異食癖起源遠端的椎動脈段比異食癖起源近端的椎動脈段更容易形成穿通動脈。在進入硬腦膜的椎動脈入口和異食性骨骺端之間產生的穿支最常見的是短旋狀或直狀,主要終止於髓質外側。發生在異食癖起源和椎基底交界處之間的主要是短旋回型,終止於髓質的前表麵和外側表麵。PICA起源遠端的椎動脈段也產生了一些分支,進入從Luschka孔突出的脈絡膜叢。
PICA產生的分支供應第四腦室的脈絡膜末梢和脈絡膜叢,通常供應第四腦室頂部中線附近和側隱窩內側的脈絡膜叢(圖2.16和2.23)(15)。這包括所有的內段和脈絡膜叢外側段的相鄰部分。更多的脈絡膜分支來自扁桃體髓和端速扁桃體段,而不是外側或前髓段。AICA通常支配異食尼卡不支配的脈絡膜叢部分,通常是橋小腦角的部分和側隱窩的鄰近部分。
PICA提供的最穩定的區域包括小腦枕下表麵同側半部分的大部分(圖2.15、2.16和2.22)。這包括同側半球和扁桃體的枕下表麵的大部分,蚓部的同側半部分,以及扁桃體的前部。異食癖提供的最大區域包括所有同側半枕下表麵,並與對側半枕下表麵重疊,以及幕麵和岩麵相鄰部分。異食癖提供的最小區域局限於同側小腦扁桃體的下部。PICA提供的皮層麵積比AICA和SCA提供的皮層麵積變化更大。如果一側異食癖缺失,則對側異食癖或同側異食癖提供通常由缺失異食癖提供的大部分區域。
皮層分支分為半球、蚓狀和扁桃體組。蚓支通常來自內側幹,半球和扁桃體分支來自外側幹。蚓部每半分為中段和中段,蚓部外側半球分為內側段、中間段和外側段。扁桃體、半球和蚓支所提供的區域有頻繁重疊的相互關係。
半腦支最常起源於蚓半裂內或遠端外側幹。它們似乎從扁桃體的上緣和外側緣向外輻射到扁桃體的半球表麵。在我們之前的研究中,PICA產生的半球分支的數量從0到9(平均2.8)。4例pica無半球分支(30例)。常見的模式是有三個分支,其中一個分支指向枕下表麵的內側、中間和外側節段。內側半腦段偶爾由內側幹供血。同側的AICA常產生與外側半球段重疊的分支,而SCA常與三個半球段的上部重疊。
圖2.23。A.後窩脈絡膜動脈示意圖。上側:後位或枕下位。脈絡膜叢由兩個內側段和兩個外側段組成。每個內側節分為吻側(結節狀)和尾側(扁桃體)部分。每個側段被分為內側,或梗,和外側,或絮凝,部分。髓質,第四腦室,椎動脈和PICAs的起源如下。脈絡膜動脈起源於PICA、SCA和AICA。脈絡膜叢與脈絡膜端相連,脈絡膜端沿著第四腦室底部的邊界與帶絛蟲相連。低:前外側的觀點。 The choroid plexus is seen through the brainstem. The AICA arises from the basilar artery and sends branches that enter the choroid plexus near the flocculus. The SCA may also send choroidal branches to the floccular part of the choroid plexus. Right Center: Diagram showing subdivision of the choroid plexus into medial and lateral segments. The medial segments have nodular and tonsillar parts and the lateral segments have peduncular and floccular parts. The floccular parts protrude through the foramina of Luschka, and the tonsillar parts extend through the foramen of Magendie. B. Schematic illustrations of the choroid plexus of the posterior fossa showing the different patterns of blood supply. Upper: Orienting diagram. The PICA and its plexal area of supply are shown in blue, the AICA in red, and the SCA in green. The PICA divides into vermian and tonsillohemispheric branches. Lower diagrams (A--D): The size of the area supplied by the arteries arising from the AICA, PICA, and SCA is shown. Each half of the schematic diagrams shows a different pattern. Colors used to show plexal areas of supply of the different cerebellar arteries are as follows: red: ipsilateral AICA; orange: contralateral AICA; blue: ipsilateral PICA; yellow: contralateral PICA; and green: ipsilateral SCA. (From, Fujii K, Lenkey C, Rhoton AL Jr: Microsurgical anatomy of the choroidal arteries: Fourth ventricle and cerebellopontine angles. J Neurosurg 52:504–524, 1980 [15].) A., artery; A.I.C.A., anteroinferior cerebellar artery; B.A., basilar artery; Ch., choroidal; F., foramen; fl., floccular; He., hemispheric; L., lateral; M., medial; Med., medulla; no., nodular; pe., peduncular; P.I.C.A., posteroinferior cerebellar artery; Pl., plexus; S.C.A., superior cerebellar artery; to., tonsillar; To., tonsillo; V.A., vertebral artery; Ve., vermian.
蚓動脈通常起源於蚓半裂的內側幹。一個常見的模式是有一個或兩個蚓分枝。如果有兩個,通常指向中位數和中位數段。如果沒有蟲蟲分支,蟲蟲區通常由對側異食癖供血。
扁桃體分支通常起源於扁桃體的外側幹,最常見的分布於扁桃體的內側、後表麵、下表麵和部分前表麵。如果扁桃體沒有主要指向扁桃體的分支,則扁桃體由相鄰的半支和蚓支供應。
異食癖與任何動脈顱神經的關係最為複雜(27,30,52)。椎動脈位於舌咽神經、迷走神經、副神經和舌下神經的前麵,異食癖神經的近端繞過或介於這些神經和鄰近神經之間,並經常拉伸或扭曲這些神經的細根。
下橄欖從椎動脈附近的髓質前外側表麵和異食癖起源處突出(圖2.24)。舌下神經前緣連接腦幹,後緣連接舌咽神經、迷走神經和副神經。大多數PICAs發生在橄欖的水平,但也有一些會發生在吻側或尾側到該水平。異食癖起源於橄欖的水平,或在橄欖的外側或前方。如果椎動脈通常在椎動脈前行,異食尼卡起始點在椎動脈前,但如果椎動脈在椎動脈後曲,異食尼卡起始點在椎動脈外側。
舌下神經在橄欖前溝(橄欖和髓錐體之間的溝)中沿橄欖尾2 / 3的前緣出腦幹形成一列細根(圖2.24)。舌下小根,在從橄欖前溝到舌下管的過程中,除了在罕見的情況下,它們在椎動脈的前麵通過。如果椎動脈拉長或彎曲,並向橄欖動脈的外側延伸,它將舌下小根向後延伸至其後表麵。一些彎曲的椎動脈將舌下小根向後伸展,與舌咽神經、迷走神經和副神經混合在一起。
異食癖的起源和近端與舌下小根的關係明顯不同。異食癖發生於舌側或舌尾或舌下細根的水平。大多數PICAs發生在舌下根與髓質交界處附近的舌下根水平(圖2.24)。發生於舌下細根上方或下方的PICAs通常發生於舌下細根上方或下方,而不是介於兩者之間。舌下小根除了被椎動脈向後拉伸外,還經常在位於橄欖尾2 / 3水平的PICAs的起源和起始段周圍拉伸。大約一半的異食尼卡起源位於舌下小根從延髓的出口引出的舌下小根的前側和後側,或位於舌下小根從延髓的出口引出的喙側線的水平。椎動脈從髓質下半部的外側延伸到髓質上半部的前表麵。PICA發生在橄欖骨下方,如果發生PICA的椎動脈沒有向前移動到舌下小根水平,就會發生在舌下小根水平的後方。如果椎動脈在到達舌下小根時位於橄欖的前方,異食尼卡的起源在舌下小根的前方。如果異食性骨痂起源部位的椎動脈向橄欖椎側延伸並向後延伸舌下小根,則異食性骨痂起源位於舌下小根的水平或後部。
PICA的起始段與舌下小根的關係是可變的。最常見的過程是異食癖起源於椎動脈,並直接在舌下小根周圍或之間通過。然而,有些pica會向上、向下或橫向地在舌下小根前麵繞圈,然後在它們之間或周圍繞圈。
經舌下小根後,異食癖遇到舌咽神經、迷走神經和副神經的小根(圖2.25)。舌咽神經、迷走神經和副神經以一列細根的形式出現,然後沿著橄欖的後緣在橄欖後溝(橄欖和髓質後外側表麵之間的一條淺溝)中離開腦幹。舌咽神經位於橄欖上三分之一的後方,位於橋髓連接處的下方,位於Luschka孔和第四腦室側隱窩的菱形唇的前方。迷走神經起於舌咽神經下方,在橄欖上三分之一的後方形成一排緊密排列的細根。副神經起源於髓質和上頸髓,位於迷走神經的下方,位於橄欖樹上三分之一和中三分之一交界處。舌咽神經和迷走神經起源於舌下小根起源水平的吻側。副細根生長於舌下細根的水平和下方。
異食癖通常通過舌咽神經、迷走神經和副神經的小根之間,從延髓的外側傳到後側。異食癖可能是上升的,下降的,或橫向的,或中間的,或參與一個複雜的循環,伸展和扭曲這些神經之間通過。在之前的研究中在50個小腦中發現的42個PICAs中,16個通過副神經的細根之間,10個通過迷走神經的細根之間,13個通過迷走神經和副神經之間,2個通過舌咽神經上方的後神經和前庭耳蝸神經之間,1個通過舌咽神經和迷走神經之間(30個)。
麵神經和前庭耳蝸神經起於舌咽神經的上方,位於橋髓連接處。異食癖的近端通常經過腦幹周圍,低於麵神經和前庭耳蝸神經。然而,在一些橋小腦角中,異食腦的近端,在向舌下小根的後方移動後,向上方循環,甚至壓迫麵神經和前庭耳蝸神經,然後向下穿過舌咽神經、迷走神經和副小根之間(圖2.11和2.12)。
異食癖閉塞的後果各不相同,可能被椎動脈閉塞的影響所掩蓋。其影響範圍從臨床無症狀閉塞到腦幹或小腦部分梗死,並伴有腫脹、出血和死亡(53)。幾乎所有異食癖的閉塞,但隻有略多於一半的椎動脈閉塞,會導致髓質或小腦梗死(5,11)。在椎動脈閉塞中,如果包括異食癖的起源,髓質和小腦梗死的發生率會大大增加。異食癖閉塞通常是由動脈粥樣硬化狹窄形成血栓的結果,較少由栓塞引起(5)。
異食癖閉塞導致下橄欖核背側的外側髓質梗塞。異食癖閉塞綜合征,稱為外側髓質綜合征,包括三叉神經脊髓束損傷引起的同側麵部麻木;脊髓丘腦道損傷引起的對側半邊身體的疼痛和體溫消失;吞咽困難、構音障礙和聲音嘶啞,這是由齶、咽、聲帶同側無力引起的,偶爾也有由模糊核病變引起的胸側突肌無力;前庭核、腦幹小腦束和小腦損傷引起的共濟失調、頭暈、眩暈、眼球震顫和同側小腦體征;由外側髓網狀物質的眼交感神經纖維斷裂引起的同側霍納氏綜合征;還有因累及細胞核和孤束而引起的嘔吐。其他不常見的伴隨症狀包括眼震和複視,這是由脊髓背側和內側縱束的病變引起的;麵部運動核損傷引起的麵部無力(10,14,17)。
與外側髓質梗死相關的綜合征可能是由PICA或椎動脈閉塞引起的,但最常見的原因是椎動脈閉塞(14,17)。Fisher等人注意到75%的外側髓質綜合征病例與椎動脈閉塞有關,隻有12%的病例有異食癖閉塞(14)。異食癖閉塞的梗死部位與椎動脈閉塞的梗死部位無明顯差異。如果出現外側髓質綜合征的其他表現,則提示椎動脈而非異食癖閉塞,包括軀幹、肢體和舌肌麻痹、交叉感覺喪失伴吞咽困難、提示鈣質皮層受累的視覺喪失、外展神經麻痹伴複視、聽力喪失或麵癱。
PICA遠端髓支分支的閉塞會產生類似迷路炎的綜合征,包括旋轉性頭暈、惡心、嘔吐、無法獨立站立或行走,以及無闌尾功能障礙的眼球震顫。頭暈、不穩定和眼球震顫被認為是由絮凝結複合體參與引起的。該綜合征中腦幹體征的缺乏表明閉塞位於異食尼卡髓支的遠端。分支閉塞通常由栓子引起,並導致小腦半球和蚓部枕下部分的梗塞。大麵積急性小腦梗死最常由異食癖或椎動脈閉塞引起,最常見的小腦梗死部位位於異食癖區域(53)。
![圖2.24。右側腦幹側位麵顯示異食癖的起源位置與下橄欖和舌下神經的小根有關。在我們檢查的50個小腦半球中發現了42個pica。舌咽神經、迷走神經和副神經的細根在橄欖的後方出現。舌咽神經和迷走神經出現在橄欖樹上三分之一的水平。附屬細枝生長在橄欖樹下三分之二及以下的水平。舌下神經的細根位於橄欖下三分之二的前方和略下方。兩個PICAS出現在橄欖的吻端三分之一處,12個出現在中間三分之一處,16個出現在尾部三分之一處,12個出現在橄欖的下方。橄欖樹前有二十棵,橄欖樹旁有二十二棵。椎動脈和位於橄欖樹旁的異食性骨骺端將舌下小根向後伸展,因為舌下小根總是在椎動脈後方通過。 (From, Lister JR, Rhoton AL Jr, Matsushima T, Peace DA: Microsurgical anatomy of the posterior inferior cerebellar artery. Neurosurgery 10:170–199, 1982 [30].)](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Infratentorial_2.24.jpg)
圖2.24。右側腦幹側位麵顯示異食癖的起源位置與下橄欖和舌下神經的小根有關。在我們檢查的50個小腦半球中發現了42個pica。舌咽神經、迷走神經和副神經的細根在橄欖的後方出現。舌咽神經和迷走神經出現在橄欖樹上三分之一的水平。附屬細枝生長在橄欖樹下三分之二及以下的水平。舌下神經的細根位於橄欖下三分之二的前方和略下方。兩個PICAS出現在橄欖的吻端三分之一處,12個出現在中間三分之一處,16個出現在尾部三分之一處,12個出現在橄欖的下方。橄欖樹前有二十棵,橄欖樹旁有二十二棵。椎動脈和位於橄欖樹旁的異食性骨骺端將舌下小根向後伸展,因為舌下小根總是在椎動脈後方通過。 (From, Lister JR, Rhoton AL Jr, Matsushima T, Peace DA: Microsurgical anatomy of the posterior inferior cerebellar artery. Neurosurgery 10:170–199, 1982 [30].)
![圖2.25。異食癖與舌咽神經、迷走神經和副神經的細根的關係。A,插圖B到f的方向。插圖顯示頭皮皮瓣和顱骨切除術的位置。大圖顯示了小腦的收縮和麵神經,前庭耳蝸,舌咽神經,迷走神經,副神經和舌下神經。舌咽根、迷走根和附屬根在橄欖的後方生長,舌下根在橄欖的前方生長。脈絡叢和小葉延伸到橋小腦角在舌咽神經和迷走神經的後麵。異食癖起源於椎動脈,經過下(B和C)、上(E和F)或舌下神經根(D)之間。在50個小腦半球發現的42個pica中,16個通過副神經根(B)之間,13個通過迷走神經和副神經根(C)之間,
10個通過迷走神經根(D)之間,
2個通過舌咽神經和前庭耳蝸神經(E)之間,1在舌咽神經和迷走神經之間(F)。曲曲性異食性耳咽癌可能上行至舌咽神經和迷走神經的前方,壓迫和扭曲麵神經和前庭耳蝸神經,然後再後移至舌咽神經、迷走神經和副神經(E和F)之間。(來自,Lister JR, Rhoton AL JR, Matsushima T, Peace DA:小腦後下動脈的顯微外科解剖。)神經外科10:17 - 199,1982[30]。](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Infratentorial_2.25.jpg)
圖2.25。異食癖與舌咽神經、迷走神經和副神經的細根的關係。A,插圖B到f的方向。插圖顯示頭皮皮瓣和顱骨切除術的位置。大圖顯示了小腦的收縮和麵神經,前庭耳蝸,舌咽神經,迷走神經,副神經和舌下神經。舌咽根、迷走根和附屬根在橄欖的後方生長,舌下根在橄欖的前方生長。脈絡叢和小葉延伸到橋小腦角在舌咽神經和迷走神經的後麵。異食癖起源於椎動脈,經過下(B和C)、上(E和F)或舌下神經根(D)之間。在50個小腦半球發現的42個pica中,16個通過副神經根(B)之間,13個通過迷走神經和副神經根(C)之間, 10個通過迷走神經根(D)之間, 2個通過舌咽神經和前庭耳蝸神經(E)之間,1在舌咽神經和迷走神經之間(F)。曲曲性異食性耳咽癌可能上行至舌咽神經和迷走神經的前方,壓迫和扭曲麵神經和前庭耳蝸神經,然後再後移至舌咽神經、迷走神經和副神經(E和F)之間。(來自,Lister JR, Rhoton AL JR, Matsushima T, Peace DA:小腦後下動脈的顯微外科解剖。)神經外科10:17 - 199,1982[30]。
PICA在處理涉及小腦橋突角、枕骨大孔、頸顱交界處、斜坡、頸靜脈孔、第四腦室和小腦的腫瘤時暴露;起源於異食性頸動脈起源的動脈瘤,最常見的部位是顱底尖以下的後窩,較少見的部位是遠端節段(30);pica -椎體交界處的動脈解剖(54,58);動靜脈畸形,通常也累及其他小腦動脈、腦幹和小腦(6);後顱窩缺血需要搭橋,因為pica可通過枕下開顱術方便進入,且靠近枕動脈(28);顱頸交界處的畸形,如Chiari畸形和骨畸形;下顱神經功能障礙如舌咽神經痛(21,23,24,29,42)。
異食癖可發生在硬腦膜外,也可發生在椎動脈硬腦膜內的任何位置。如果動脈起源於椎動脈穿過硬腦膜的通道附近,則可位於髓質外側;如果動脈起源於椎基底動脈連接處高處,則可位於腦幹前方。暴露較低的異食癖起始部位,無論是外側還是硬膜內,都可以通過枕下正中線或遠側入路實現。如果起始位置較低的動脈必須向上進入橋小腦角,或者需要移動椎動脈通過硬腦膜的部位,則需要考慮遠側或經髁突改良入路。乙狀結腸後開顱術可能足以暴露起源於腦幹外側椎動脈中部、橋小腦角下部的異食癖。如果需要暴露中線深處靠近椎基底關節處的起始點,則可能需要采用幕上下乙狀竇前入路,並增加一定程度的迷宮切除,具體取決於異食癖起始點的深度和病理情況。中線枕下顱骨切除術,可能同時切除寰後弓,通常足以暴露扁桃體髓和端速扁桃體動脈段的病理。在第四腦室壁、蚓部和蚓旁區發生異食癖的病變,通常通過枕下中線入路暴露。可通過垂直枕下切口和以病理為中心的開顱術暴露半球支病變。下顱神經和髓質的異食癖壓迫的解剖在橋小腦角部分進行了回顧。
貢獻者:Albert L. Rhoton, Jr, MD
內容來自Rhoton AL, Jr.後顱窩:顯微外科解剖和外科入路。神經外科2000; 47:1196。doi.org/10.1097/00006123 - 200105000 - 00065.經牛津大學出版社代表神經外科醫師協會批準。©神經外科醫生協會。
神經外科188bet手机app圖譜很榮幸能夠繼承Albert L. Rhoton, Jr . MD的遺產。
請登錄發表評論。
一定要在社交媒體上關注我們,獲取精彩內容並保持更新生活科恩醫生的會議,關於手術技術的問題,以及更多!


您必須登錄才能查看此材料。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
現在請捐!
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。請承諾每年至少捐贈250美元給Atlas。
如果沒有這個承諾,Atlas將很快需要付費訂閱世界上許多病人的護理都依賴於它的外科醫生將無法使用它。現在請捐!