

你可以有所作為。
的188bet手机app這幾乎完全取決於你的捐款。
沒有你們的大量捐贈,我們無法繼續進行地圖集。
請承諾每年至少捐款250美元給地圖集。如果沒有這個承諾,Atlas將很快需要付費訂閱,世界上許多病人的治療依賴於它的外科醫生將無法獲得它。
現在請捐!
最後更新日期:2021年6月22日
本研究的目的是展示和回顧沿整個走行展神經及其周圍結構的詳細顯微解剖,並提供其地形測量。在動脈和靜脈注射彩色矽膠後,用×3到×40的放大倍數檢查了10具屍體的頭部。采用不同的顱底入路解剖每具頭顱的兩側,以展示外展神經從橋髓溝到外側直肌的整個走行過程。岩斜坡區和外展神經通過的海綿竇的解剖結構複雜,因為重要的神經和血管結構密度很高。外展神經有成角和固定點沿其路線,使神經在許多臨床情況下的風險。從外科角度看,岩尖的岩結節是術中避免損傷外展神經的標誌。外展神經與其他神經有很大的不同。沒有其他顱神經有像岩斜坡靜脈彙合處外展神經那樣的長硬膜內成角和固定。準確了解外展神經與周圍結構之間的關係,使神經外科醫生能夠在無手術並發症的情況下接近斜坡、岩斜坡區、海綿竇和眶上裂。
在過去的幾年中,顱底病變的外科治療越來越多。由於外展神經位於岩斜坡區和海綿竇區,是顱底最複雜的區域,因此其顯微外科解剖對於臨床和手術入路具有重要意義。外展神經從起源至終止,沿蛛網膜下腔(Iaconetta et al., 2007),岩石斜坡區(Ozveren et al., 2002a, 2003;Iaconetta等人,2003年;Ozer et al., 2010),海綿竇(Iaconetta et al., 2001, 2007;Jittapiromsak等人,2010)和orbit (Iaconetta等人,2007;Shi等人,2007)。外展神經在顱內沿血管、神經、韌帶和骨結構走行較長,極易受到直接和間接損傷(Takagi et al., 1976;Antoniades等人,1993年;Lazow等人,1995; Ziyal et al., 2003). The abducens nerve usually exits the pontomedullary sulcus of the brainstem as a single trunk. However, it may split into duplicated branches along its course. The incidence of duplication has been reported in the literature to range from 5% to 28.6% (Nathan et al., 1974; Marinkovic et al., 1994). In the presence of duplication or variations of the abducens, care should be taken to prevent surgery-related risks and complications. Preoperative diagnosis of the duplicated abducens nerve is possible through thin slice magnetic resonance imaging (Alkan et al., 2004).
準確掌握外展神經及其周圍結締組織和神經血管結構的解剖學知識,將有助於外科醫生使用經顱和內鏡入路探索岩石斜坡區、海綿竇和眶上裂(SOF)。本解剖研究的目的是回顧外展神經從腦幹到外側直肌的整個解剖結構及其周圍的結締組織和神經血管結構。
采用10具成人頭顱(20例)進行顯微外科解剖。用甲醛固定屍體頭部後,切開頸總動脈、椎動脈和頸內靜脈,用聚乙烯導管插管,用生理鹽水徹底清除碎片或化學物質。這些血管被注射了彩色的矽膠混合物,紅色代表動脈,藍色代表靜脈。將矽酮混合物留在血管內硬化48小時。接下來,去掉頭顱骨。大腦被小心翼翼地取出,特別注意腦神經。外展神經在岩石斜坡區穿透硬腦膜。仔細解剖外展神經入口周圍的硬腦膜內層,以揭示神經的走行和靜脈口。切除硬腦膜後,逐層解剖岩石斜坡區內部結構,並拍照記錄。切除海綿竇外側壁以顯露顱神經。 After the SOF and annulus of Zinn were opened, the nerve was entirely exposed.
在OPMI手術顯微鏡(Carl Zeiss Co., Oberkochen, Germany)的光學放大下,沿10個頭顱的展神經走行,對兩個顱底區域進行間隔解剖。使用一台EOS 50D相機(佳能,日本東京)進行攝影記錄。
外展神經由蛛網膜下腔、岩斜坡、海綿體和眶部組成。硬膜間岩斜和海綿內部分在顱底硬膜層之間走行,其解剖結構較其他部分複雜。
外展神經在腦橋和延髓的交界處離開腦幹,位於麵神經內側。當神經出現在腦幹中線4.35 mm (3.0-5.8 mm)處的橋髓溝時進入蛛網膜下腔(圖1C和1D)。該段在腦橋和斜坡之間向上、向前、外側走行,然後穿過位於三叉神經硬腦膜入口孔下方的硬腦膜內層,進入硬腦膜間岩斜坡靜脈彙合處(PVC;Iaconetta等人,2003年)。該管段平均長度為15.8 mm(範圍12.8 ~ 19.1 mm),平均直徑為1.31 mm(範圍0.8 ~ 1.7 mm)。岩石斜坡硬腦膜的外部反射形成了硬腦膜入口孔和外展神經的硬腦膜套(圖1E和1F)。外展神經的硬腦膜入口孔直徑為1.63 mm(範圍1.1 ~ 2.1 mm)。蛛網膜延伸至斜坡,形成橋前池前壁,前側反射至外展神經的硬腦膜入口孔,並跟隨神經進入硬腦膜套內。
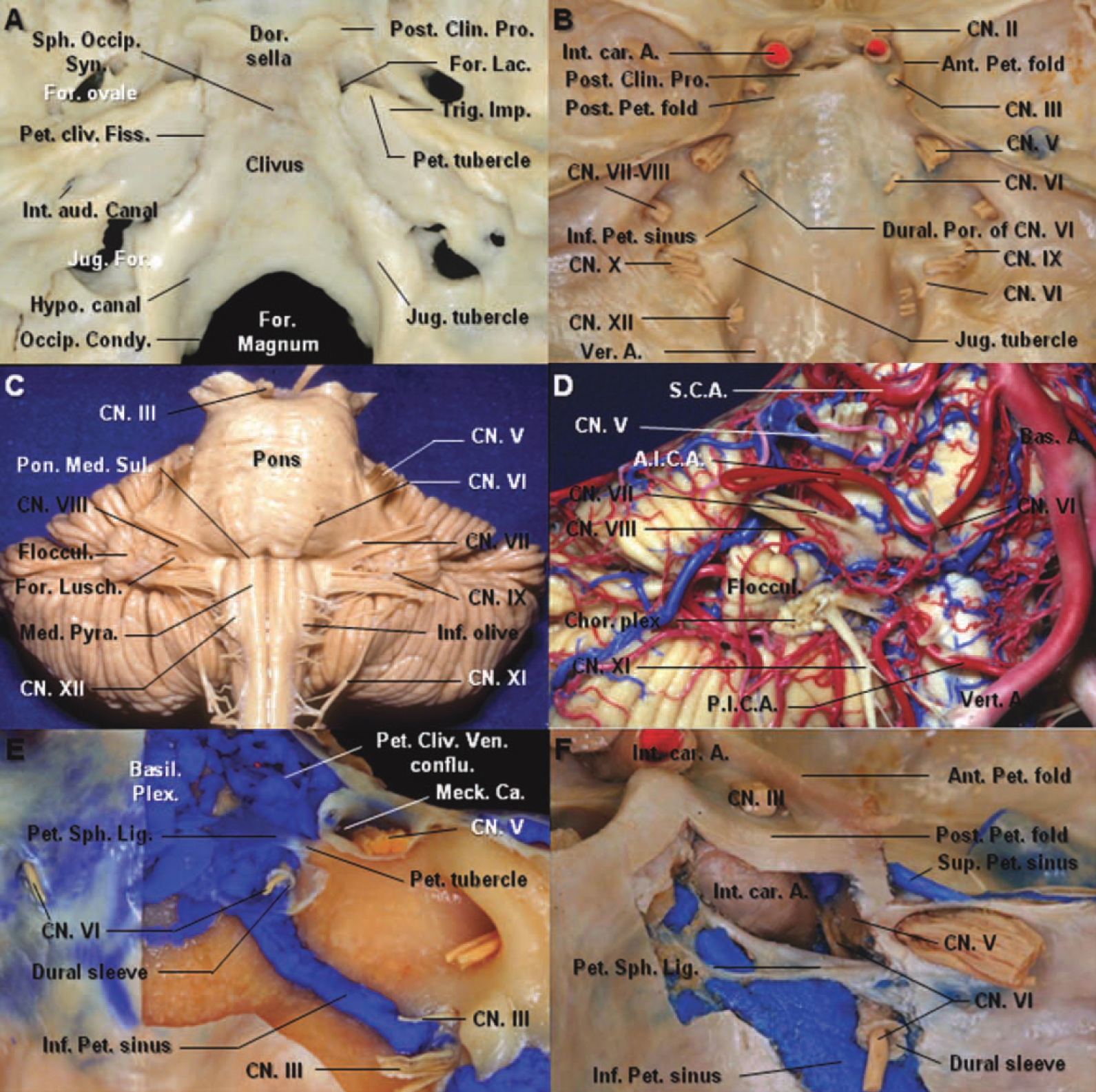
圖1。答:顳骨的岩骨尖進入枕骨的斜坡部分和蝶骨的大翼之間的角間隔。岩骨尖為頸內動脈內孔,形成裂孔後外側邊界。岩結節,岩蝶韌帶的插入處,位於三叉神經壓痕內側。B:大腦已經被切除,暴露顱孔以便腦神經。外展神經進入外展神經和多雷洛管的硬腦膜孔,位於三叉神經孔的內側和下方。岩下竇在外展神經內側。C:腦幹前視圖。外展神經在腦橋和延髓的交界處離開腦幹,位於麵神經內側。它在橋腦橋和斜坡之間向橋腦橋蛛網膜的前方和外側向上運動。 D: The anterior inferior cerebellar artery passes dorsal to the abducens nerve. The vein of the pontomesencephalic sulcus courses below the abducens nerve. E: The meningeal dural layer of the posterior aspect of the petrous apex has been removed to expose the dural sleeve of the abducens nerve, petroclival venous confluence, basilar plexus, and inferior petrosal sinus. The inferior petrosal sinus connects the petroclival venous confluence with the jugular bulb and courses medial to the abducens nerve. The abducens nerve passes under the petrosphenoid ligament. F: The petroclival venous confluence has been removed. The abducens nerve enters the cavernous sinus between the internal carotid artery and the trigeminal nerve. The cisternal space follows the nerve inside the dural sleeve. The petrosphenoid ligament is attached laterally to the petrous tubercle medial to the trigeminal nerve. A., artery; Ant., anterior; Aud., auditory; Bas., basilar; Ca., cave; Chor., choroid; Clin., clinoid; CN., cranial nerve; conflu., confluence; Condy., condyle; Dor., dorsum; For., foramen; Hypo., hypoglossal; Imp., impression; Inf., inferior; Int., internal; Jug., jugular; Lac., lacerum; Lig., ligament; Meck., Meckel’s; Med., medulla; Occip., occipital; Pet., petroclinoid; Petro., petrosal; Plex., plexus; Pon., pons; Por., porus; Post., posterior; Pro., process; Pyr., pyramid; Sin., sinus; Sph., sphenoid; Sul., sulcus; Syn., synostosis; Ven., venous; Ver., vertebral. (Images courtesy of AL Rhoton, Jr.)
小腦前下動脈橋前段經腹側至外展神經的比例為85%,經背側至神經的比例為15%(圖1D)。在我們的標本中,我們沒有發現任何動脈供應外展神經的腦池段。
外展神經穿入岩斜坡硬腦膜內層後,在硬腦膜入口孔向岩尖(1膝)呈水平略直的方向逐步走行,並通過硬腦膜間靜脈彙合處,稱為蝶斜坡靜脈彙合處(SPCVC;Destrieux等人,1997;Iaconetta等人,2003年)。SPCVC位於海綿竇後部、基底神經叢外側、岩上、岩下竇前部(SPS和IPS;圖1B, 1E, 1F和2A-2F)。基底神經叢的大部分位於斜坡硬腦膜層之間,從鞍背延伸至斜坡中部。在斜坡中部和枕骨大孔之間可能存在靜脈間隙島。它是橫跨中線的最大、最穩定的海綿竇間連接,連接兩個海綿竇的後部。SPS經三叉神經硬腦膜入口孔上方,位於硬腦膜與梅克爾洞背外側壁之間。它連接SPCVC和海綿竇後部與橫竇和乙狀竇交界處。 The IPS, which is situated in the petroclival fissure, connects the SPCVC with the jugular bulb (Fig. 1B, 1E, and 1F). In 16 of the 20 specimens (80%), the main portion of the IPS opening into the SPCVC is lateral to the dural porus of the abducens, and in the remaining four specimens (20%), it is medial to this dural porus. The dural entrance porus of the abducens nerve was surrounded with the blood of the IPS.

圖2。岩尖區逐步解剖。A:岩尖的前外側視圖。硬腦膜層形成海綿竇的頂部已被切除,以暴露動眼肌和滑車神經。B:已切除硬腦膜層以暴露後斜突,並縫合後內側反射。C:沿斜坡取出反射硬腦膜層,打開外展神經進入硬腦膜的入口。醫生:取出硬腦膜層後,藍色矽膠顯示岩斜坡靜脈彙合已暴露。E,F:岩石斜坡靜脈彙合處被切除,露出石油蝶骨韌帶。岩蝶韌帶外側連接岩結節,並與硬腦膜套連接下外展神經。腦膜背動脈起源於腦膜垂體幹,沿外展神經內側後方通過。 A., artery; Cav., cavernous; Car., carotid; Clin., clinoid; Cliv., clival; CN., cranial nerve; Conflu., confluence; Dor., dorsal; Gang., ganglion; Lig., ligament; Mening., meningeal; MHT., meningohypophyseal trunk; Petro., petrosal; Post., posterior; Pro., process; Seg., segment; Sin., sinus; Sph., sphenoid; Tri., triangle; Ven., venous. (Images courtesy of AL Rhoton, Jr.)
SPCVC的前緣是一個冠狀麵,上麵穿過岩狀後褶,下麵穿過海綿狀頸動脈垂直段的後壁。後緣是岩斜硬腦膜層。內側緣是一個矢狀麵,穿過鞍背外側邊緣到外展神經的硬腦膜入口孔的後方和下方。SPCVC的側限為Meckel’s cave的內側邊緣。下界是穿過外展神經和三叉神經硬腦膜入口孔的線。三叉神經入路點與外展神經之間的平均距離為9.41 mm(範圍為6.4 ~ 12.5 mm;圖2、3C、3D)。

圖3。側麵圖。海綿竇外側壁自小腦幕邊緣向下延伸,與覆蓋梅克爾穴和中窩的硬腦膜融合。硬腦膜外層已從海綿竇和梅克爾洞側壁剝離。這暴露了三叉神經。B:覆蓋梅克爾氏穴的薄層由部分蛛網膜組成,從後窩向前延伸,包圍三叉神經至三叉神經節水平。C:優越的觀點。外展神經蛛網膜下段在腦橋和斜坡之間向上、向前、向外側走行,然後穿過位於三叉神經硬腦膜入口孔下方的硬腦膜內層進入硬腦膜間岩斜坡靜脈彙合處。SPS經梅克爾穴口上方,與海綿竇後部連接。醫生:外展神經走出多雷洛管,進入海綿竇。 The abducens nerve is attached to the posterior vertical segment of the cavernous carotid artery by connective tissue. The trigeminal nerve has been retracted laterally to expose the petrolingual ligament, spanning from the lingula of the sphenoid bone anteriorly to the petrous apex posteriorly and covering the superiolateral surface of the lacerum segment of the carotid artery. The basilar plexus is located between the layers of the dura mater on the clivus and extends from the dorsum sella to the anterior rim of the foramen magnum. A., artery; ACP., anterior clinoid process; Ant., anterior; Bas., basilar; Car., carotid; Cav., cavernous; CN., cranial nerve; Conflu., confluence; For., foramen; GSPN., great superficial petrosal nerve; Hypo., hypophyseal; Inf., inferior; Lat., lateral; Lig., ligament; Ling., lingual; MMA., middle meningeal artery; Pcom., posterior communicating; PCP., posterior clinoid process; Pet., petroclinoid; Pitu., pituitary; Plex., plexus; Post., posterior; Rotund., rotundum; SPS., superior petrosal sinus; Sph., sphenoid; Tr., trunk; Ven., venous. (Images courtesy of AL Rhoton, Jr.)
SPCVC包含岩蝶韌帶(Gruber’s韌帶)、岩斜坡段和外展神經的硬腦膜套,以及脊膜背動脈(圖2C-2F)。岩蝶韌帶與岩斜坡硬腦膜平行,並與岩斜坡前內側的後clinoid突和斜坡上外側部分以及後外側的岩結節(岩尖三叉神經印的內側邊界)相連(Iaconetta et al., 2001)。外展神經與岩結節之間的平均距離為2.80 mm(範圍為1.4 ~ 9.5 mm;圖2)。
岩蝶韌帶呈蝴蝶狀,中點狹窄,由致密的膠原纖維組成(圖2E和圖2F)。韌帶內側止點和外側止點寬度分別為3.85 mm (1.8 ~ 6.4 mm)和3.0 mm (1.7 ~ 5.7 mm)。韌帶中點處寬度為2.05 mm(範圍1.1 ~ 3.3 mm)。其長度為11.05 mm(範圍為7.5-14.5 mm)。岩蝶韌帶和岩斜坡硬腦膜層之間的狹窄空間充滿了血液。該韌帶將SPCVC分為兩個空間:上間隙(韌帶和後岩clinoid褶皺之間)和下間隙(韌帶和骨溝之間);在20例標本中,有5例(25%)發現骨化(圖3)。在我們的研究中,外展神經的硬膜套、脊膜背動脈或其分支以及靜脈血腔位於petro蝶韌帶下方(圖2C-2F)。
在95%的20例標本中,外展神經的硬脊膜套經過多雷洛管的外側一半,受蝶背內側外側緣、上方的岩蝶韌帶、下方的上斜坡上緣和外側的岩尖的限製。在5%的標本中,硬腦膜套通過內側半部分。硬腦膜入口孔周圍硬腦膜套管較厚,多雷洛管頂端較薄。它覆蓋著在硬腦膜入口孔和岩蝶韌帶前緣之間的展神經。其長度為9.18 mm (6.8 ~ 12.4 mm)。硬腦膜套附著於岩蝶韌帶下方,並延伸至海綿竇作為纖維層,覆蓋神經直至外側直肌(圖2E和2F)。在岩尖處,神經向下外側延伸形成第二膝並到達海綿內頸動脈垂直段的外側。展展岩斜段長度為11.34 mm(範圍8.9-13.4 mm;圖4)。

圖4。岩尖的側麵圖。答:梅克爾氏穴的蛛網膜覆蓋,向前延伸至三叉神經後根至神經節中段水平。三叉神經根後上方的岩上竇已被切除。外展神經從石化蝶韌帶外側下進入海綿竇。B:眼神經已向外側牽開。外展神經在海綿竇內延伸至眼神經的內側並在岩舌韌帶的上方平行穿過眶上裂。下外側幹起源於海綿頸動脈水平段的中間部分的外側。它穿過外展神經的外側和三叉第一分支的內側。頸內動脈穿過岩舌韌帶後,在頸動脈海綿狀垂直段近端前外側可見交感神經叢。 The plexus anastomose with the cavernous segment of the abducens nerve. C: Anterior view of a coronal section in front of the sphenoid sinus, through the orbits and pterygoid processes. The pituitary gland, intracavernous carotids, optic nerve, and cavernous sinus have been exposed by removing the bone of the sinus wall. The upper part of the clivus has been removed to expose the basilar plexus. The periarterial sympathetic plexus courses upward along the posterior vertical segment of the cavernous carotid artery. D: Anterior oblique view of the coronal section. The petroclival venous confluence has been removed to expose the abducens nerve. After entering the dura, the abducens nerve courses in a somewhat straight direction to reach the petrous apex. The abducens nerve has a pseudobranching pattern which has no intervening tissue in the cavernous sinus and anastomoses with the periarterial sympathetic plexus. A., artery; Bas., basilar; Car., carotid; CN., cranial nerve; For., foramen; Gl., gland; GSPN., great superficial petrosal nerve; Hypo., hypophyseal; Inf., inferior; Lat., lateral; Lig., ligament; N., nerve; Oph., ophthalmic; Opt., optic; PCP., posterior clinoid process; Pitu., pituitary; Plex., plexus; Sin., sinus; Sph., sphenoid; SOF., superior orbital fissure; Str., strut; Sympath., sympathetic; Tent., tentorial; Tr., trunk. (Images courtesy of AL Rhoton, Jr.)
腦膜背動脈及其分支起源於頸動脈海綿體後膝的腦膜下幹,經外展神經內側,75%的病例經石油蝶韌帶下。雖然我們已經知道脊膜背動脈為這段外展神經提供血液供應,但我們沒有發現在硬膜間岩斜坡區神經和動脈之間有任何直接的聯係(Dolenc, 1987)。
外展神經離開多雷洛管,進入海綿竇。海綿竇外側壁的外層(骨膜層)較厚,呈珍珠灰色,而內層(腦層)較薄,透明,包含動眼肌、滑車、該神經向外側彎曲,繞海綿竇近端(第3膝),向前進入眼神經內側的海綿竇內,在頸內動脈外側緩慢上升。神經向內側接觸頸動脈海綿狀段外側壁,向外側接觸梅克爾穴內側壁。外展神經位於海綿竇壁神經進入的最內側位置,並通過海綿竇保持該位置(圖3C和圖4)。外展神經在海綿竇內繼續走行於眼神經的內側和下方,在通過SOF離開前走行於岩舌韌帶的上方並平行於岩舌韌帶(圖4A和圖4B)。
動脈周圍交感神經叢是一個神經纖維網絡,與ICA的岩石段附著在一起,形成一層非常薄的動脈周圍結締組織。頸動脈通過岩舌韌帶後不久,在海綿狀頸動脈垂直段近端前外側可見交感神經叢。外展神經在硬膜套末端與頸動脈海綿狀段外側壁交感神經叢分支和三叉神經吻合,形成第3膝(圖4)。然後,交感神經叢與眼神經一起,通過鼻乳頭神經的分支——睫狀長神經到達瞳孔擴大器(Ozveren et al., 2001)。外展神經通過結締組織與海綿狀頸動脈垂後段及前彎起點相連。在該區域,近端外展神經的圓形改變為扁平垂直形態,神經可能分裂成多個束。在我們的標本中,展神經海穴段分成兩束(25%)和三束(10%)。在離開海綿竇之前,複製的神經在ICA的水平部分融合為一根幹(圖4B-4D)。
下外側幹(海綿竇下動脈)起源於距腦膜垂體幹起源6.30 mm(範圍,3.8-8.5 mm)的海綿竇內頸動脈水平段中段外側。它經過外展神經外側(90%)或內側(10%),提供外展神經分支,並向下行至三叉神經第一分支的內側,供應海綿竇下側壁硬腦膜。外展神經與下外側幹起點之間的平均距離為2.65 mm(範圍為1.3-4.1 mm;腦膜垂體幹距離外展神經7.1 mm (3.9-12.8 mm),距離多雷洛管7.58 mm (5.4-12.0 mm)。下外側幹的腹側支通向SOF並供給在SOF附近的外展神經海綿狀段的前部。外展神經海綿狀段平均長度為27.23 mm(範圍為23.1 ~ 30.2 mm)。
該段始於神經穿過SOF和Zinn環的那部分,止於神經進入外側直肌(圖5和圖6)。外展神經通過SOF進入眶。SOF是一個很小但在地形上很重要的區域,它連接中顱窩和眼眶。它分為上外側和下內側。外展神經與動眼神經和鼻睫神經一起穿過SOF的下內側(圖5A-5D)。外展肌在眼神經內側的海綿竇內向前移動,並在鼻睫神經下方橫向移動,因為它穿過SOF的內下部分和環狀肌腱進入外側直肌的內表麵。外展神經在鼻睫神經的下外側,在動眼神經上段的下側,在SOF的下段的上外側。有一個纖維間隔將外展神經和動眼神經的上段隔開,動眼神經的運動部分和鼻睫神經的感覺部分(圖5D)。

圖5。答:優越的觀點。眶頂、眶周和脂肪被切除,露出位於眶周下方眶脂肪內的滑車神經、額神經和淚神經。視神經管已無頂蓋,右側前斜突已切除。硬腦膜位於顱中窩底部,海綿竇經眶上裂延伸至眶周。覆蓋眶尖骨的眶周,襯著眶上裂和視神經管的硬腦膜,以及視神經鞘的纖維成分融合形成津環,即直肌產生的常見腱環。排列前斜突下緣的左側硬腦膜層已被切除,並向外側反射以暴露滑車神經和額神經。B:左側眶上裂側麵片。眶上裂的側緣被保留。外展神經穿過眼神經內側的海綿竇。 The abducens nerve passes through the central region of the superior orbital fissure inferomedial to the nasociliary nerve. C: Lateral view of the left orbital apex. The frontal, lacrimal, and trochlear nerves pass outside the annulus of Zinn, and the nasociliary, oculomotor, and abducens nerves pass through the tendon. D: An incision has been made in the annulus of Zinn along the medial aspect of the nasociliary nerve, which lies outside the annulus. The oculomotor nerve and its divisions are located deep and medial to the abducens nerve. The fibrous septum separates the abducens nerve from the nasociliary nerve in the annulus of Zinn. The nasociliary nerve gives rise to short ciliary nerves to the ciliary ganglion located inferolateral to the optic nerve. E: Superior view of the right orbit. The levator and superior rectus muscles have been retracted medially to expose the nasociliary and the abducens nerve. From the superior orbital fissure, the abducens nerve enters the medial surface of the lateral rectus muscle. F: The optic nerve has been retracted medially to expose the inferior division of the oculomotor nerve and the ciliary ganglion. The ciliary ganglion is situated on the inferolateral aspect of the optic nerve and on the medial side of the lateral rectus muscle. It receives three branches: the motor root from the inferior division of the oculomotor nerve, the sensory root from the nasociliary nerve, and sympathetic fibers from the plexus around the ophthalmic artery. G: The abducens nerve is divided into several branches to innervate the muscle on the medial aspect of the lateral rectus. ACP., anterior clinoid process; Cili., ciliary; CN., cranial nerve; Div., division; Fib., fibrous; Gang., ganglion; Inf., inferior; Lac., lacrimal; Lat., lateral; Lev., levator; M., muscle; N., nerve; Nasocili., nasociliary; Obl., oblique; Oph., ophthalmic; Opt., optic; Post., posterior; Rec., rectus; Str., strut; Sup., superior; V., vein. (Images courtesy of AL Rhoton, Jr.)

圖6。A,B,C:經眶尖平行於斜坡的冠狀切麵。切除蝶竇壁和斜坡,露出海綿內頸動脈和外展神經。外展神經在蛛網膜下腔向上、向前、向外側伸展,然後穿過岩斜硬腦膜進入岩斜靜脈彙合處。外展神經的岩斜段逐漸向水平和直線方向前進。外展神經的第一個角在硬腦膜入口孔的水平。第二個角在岩尖上。第三個角位於頸動脈垂直後段的外側壁。外展神經在鼻睫神經的下方橫向移動通過眶上裂和環狀肌腱進入外直肌的內表麵。D:右軌道的下視圖。 The inferior rectus muscle has been retracted medially to expose the optic nerve, the ciliary ganglion, and the central retinal artery. The abducens nerve runs medial to the surface of the lateral rectus muscle. E: The intraorbital portion of the optic nerve has been removed. The inferior division of the oculomotor nerve is divided into three branches, innervating the medial rectus, inferior rectus, and inferior oblique muscles. F: Anterior view of the right orbit. The intraorbital portion of the optic nerve and the globe has been removed. The abducens nerve passes through the annulus of Zinn and then enters the medial surface of the lateral rectus. The nasociliary nerve crosses medially between the two divisions of the oculomotor nerve and above the optic nerve to reach the medial part of the orbit. A. artery; Bas., basilar; Car., carotid; Cen., central; Cili., ciliary; CN., cranial nerve; Div., division; Eust., Eustachian; Gang., ganglion; Gl., gland; Hypo., hypophyseal; Inf., inferior; Int., internal; Lac., lacrimal; M., muscle; Med., medial; N., nerve; Nasocili., nasociliary; Obl., oblique; OCR., opticocarotid recess; Pitu., pituitary; Oph., ophthalmic; Rec., rectus; Ret., retinal; Sup., superior; Sympath., sympathetic. (Images courtesy of AL Rhoton, Jr.)
在SOF水平,鼻睫神經起源於眼神經內側,向外側緩慢上升至動眼神經下段,然後在動眼神經兩段之間的中間穿過並在視神經上方到達眶內側部分。在眶尖處,當外展神經向外側移位到達外直肌內側麵時,鼻睫神經和動眼神經下段向內側彎曲(圖5和圖6)。外展神經被分為3至5支,支配外直肌內側麵的肌肉。80%的外展神經分支在外側直肌後1 / 3處結束,其餘20%的外展神經分支在中間1 / 3處結束。外展神經眶段長度為13.35 mm(範圍10.2 ~ 17.5 mm;圖5、6)。
外展神經(VI)在顱內的病程較長,因此會受到許多病理病變的影響,包括引起顱內壓改變的情況(Takagi等,1976;布萊克和查普曼,1981年;Umansky等人,1992年;Berlit等人,1994;Krisht等人,1994;Ziyal等人,2003;Ayberk等人,2008)。然而,滑車神經起源於中腦頂蓋後方,其路徑也較長,因此腦積水患者很少損傷滑車神經。這就是為什麼外展神經麻痹的發生與其他機製有關,而不是顱神經的長度(Hanson et al., 2004)。本研究的目的是探討整個外展神經沿其走行路徑及其周圍的解剖關係。
Umansky等人(1991,1992)認為,外展神經顱內走行較長,其彎曲性以及在岩尖水平與顱底的緊密連接,解釋了神經在某些病理條件下的脆弱性。最近的解剖報告顯示,外展神經岩石斜坡段被膜覆蓋,在神經穿過多雷洛管時剛性固定,因此不允許任何運動(Tubbs et al., 2011)。我們觀察到神經從外腦幹到海綿竇有三個角度,並與周圍結構有幾個附著。第一個角度在硬腦膜入口孔水平。
神經在蛛網膜下腔向上、向前和向外側運動,然後穿過硬腦膜進入SPCVC。它的方向在彙流中改變,並逐漸沿水平和直線方向運動。第二成角在岩尖上,在這裏神經向下向外側走行,到達海綿狀頸動脈垂直後段的外側壁。第三角位於頸動脈垂直後段的外側壁,在這裏外展神經與動脈周圍交感神經叢相連。Umansky等人(1992)觀察到最嚴重的成角和主要固定點在岩石頂點,即第二成角。外展神經岩斜部和海穴部的固定被認為是栓係點,導致顱內腫瘤患者神經麻痹作為錯誤的定位標誌(Ro et al., 1995;Ayberk等人,2008;Tubbs等人,2011年)。據報道,改變腦幹的病理條件,如自發性顱內低血壓或治療腦積水的分流手術繼發低血壓,可通過拉伸力導致外周神經麻痹(Black and Chapman, 1981;Ayberk等人,2008)。 The mechanism of these nerve palsies is thought to be compression of the abducens nerve against the dural entrance porus and petrous apex by retraction related to the downward migration of the brainstem (Rush and Younge, 1981; Miller et al., 1982).
外展神經麻痹可能在經靜脈途徑的IPS血管內手術中發生(Oishi等,1999)。如果外展神經占據多雷洛管的內側半段,神經在導管的路徑上,可能會導致神經損傷(Ozveren et al., 2002a)。在20例標本中,隻有5%的標本在多雷洛管的中側發現外展神經。此外,經靜脈途徑經IPS後孤立性外展神經麻痹的發生率相對較低,可能與外展神經的硬膜套保護有關。在導管引起的神經損傷中,外展神經的硬腦膜套厚度可能很重要(Ozveren et al., 2002a)。岩斜區外展神經的膜性保護使神經具有抵抗病理的能力。然而,在岩尖以外的海綿竇內,這種膜性覆蓋減弱。因此,與海綿體病變相比,外展神經似乎可以抵抗岩斜坡腫塊的侵襲,因為它有膜覆蓋(Ozveren等,2002b)。
盡管神經外科知識不斷提高,但對多雷洛管邊界的定義仍存在爭議。多雷洛管最早被格魯伯(1859)描述為位於岩骨頂端的骨纖維管,包含外展神經和IPS。1905年,Dorello將該運河描述為岩石頂點和岩蝶韌帶之間的解剖區域(Dorello, 1954)。Nathan等人(1974)將椎管定義為由岩尖、岩clinoid韌帶和鞍背所限製的小空間。早期研究將Dorello 's canal描述為岩石頂點和Gruber 's (petro蝶骨)韌帶之間的短的骨纖維通道(Dorello, 1954;Piffer和Zorzetto, 1980;Tsitsopoulos等人,1996;朗,2001)。雖然有報道稱外展神經穿過petro蝶韌帶下方,但一些研究表明外展神經的分支在其上方(Jain, 1964;Nathan等人,1974年)。 Later, investigators defined Dorello’s canal as a larger anatomic space of the petrous apex between the inner and outer layer of the petroclival dura mater (Umansky et al., 1991; Fukushima et al., 1996; Destrieux et al., 1997; Ono et al., 2004). Destrieux et al. proposed to name the area, located between the cerebral and periosteal layers of the petroclival dura mate, the PVC instead of the Dorello’s canal. The abducens nerve courses from the dural entrance porus to the posterior part of the cavernous sinus through the PVC (Destrieux et al., 1997). Classically, Dorello’s canal is defined as being located inside a PVC formed by the junction of the posterior cavernous sinus, basilar sinus, and the IPS. Therefore, the petrosphenoid ligament is immersed in the venous confluence (Iaconetta et al., 2003).
石油蝶骨韌帶(Gruber’s韌帶)是岩石斜坡區的一個重要結構,不僅從解剖學角度,而且在外科和血管內實踐中都是如此。這條韌帶固定了外展神經的鞘。在岩骨鑽孔時,外展神經由岩蝶韌帶保護(Ozveren et al., 2002a)。該韌帶與岩斜坡硬腦膜平行,在鞍背外側水平附著於後斜突下方,並向岩頂點移動。岩舌韌帶從前蝶骨舌骨延伸至後岩尖,覆蓋頸內動脈裂孔段的上外側。上蝶骨(Gruber’s)韌帶和下蝶骨(岩舌)韌帶的複合物構成了惡性韌帶(Iaconetta et al., 2003,2007)。
外展神經的變化可能有一些實際的手術相關的含義。外展神經通常離開腦幹作為一個單獨的幹。然而,據報道,雙展神經的發生率從8%到18%不等(Jain, 1964;Nathan等人,1974年;Iaconetta等人,2001年)。Nathan等人提出了外展神經的三種走行模式。在I型(86.5%)中,神經從腦幹以單一主幹的形式出現,到達外側直肌。II型展神經(6%)以單一主幹的形式離開腦幹,並在其腦池段分裂為兩個分支。它們分別刺穿硬腦膜,合並成一個主幹,然後進入眶內。在III型(7.5%)中,神經起源於兩個獨立的幹再次融合入海綿竇(Nathan et al., 1974)。 Jain (1964) identified another anatomical variation in which the abducens nerve emerges from the brainstem as two branches that travel anteriorly, and innervate the lateral rectus muscle separately. In this study, we found the incidence of a duplicated abducens nerve to be 35% in the cavernous segment. Based on the classification proposed by Nathan et al., our all specimens belonged to the Type I. In Types II and III, the abducens branches pierce the dura through separate entrance porus and travel independently with intervening tissue and then reunite. The branching anatomy of the abducens nerve at the cavernous portion which has no intervening tissue is labeled ‘‘pseudobranching.’’ Pseudobranching is perhaps caused by pressure of the ICA against the nerve at its angulation at the carotid angle (Ozer et al., 2010). True branching and duplication are probably congenital (Iaconetta et al., 2001).
外展神經的血液供應是眾所周知的(Dolenc, 1987;Krisht等人,1994;Marinkovic等人,1994)。Marinkovic等人報道,蛛網膜下段的血液供應來自於前外側動脈(85.71%),尤其是來自基底動脈穿支的動脈。小腦前下動脈占蛛網膜下段的14.29%,橋腦動脈僅占7.14% (Marinkovic et al., 1994)。岩斜部分由腦膜垂體幹的脊膜支支配。海綿竇和眶部的血供來自下外側幹的眼支,即海綿竇下動脈。然而,在本研究中,在岩斜坡彙合處,沒有腦膜背動脈分支通過硬腦膜和蛛網膜覆蓋穿透外展神經。Yasargil(2002)描述了顱神經及其動脈和靜脈以蛛網膜包的形式在其自身的椎間孔中前進。蛛網膜下腔延伸至多雷洛管表明外展神經是通過蛛網膜下腔的小動脈或腦脊液供應的,或兩者兼有(Ozveren等人,2002b, 2007)。
從外科角度看,外展神經位於岩結節的正下方和內側,是岩尖三叉神經壓痕的前邊界。在進行顳下-經顳-經岩骨入路切除顱後窩和中窩病變時,岩結節是避免外展神經損傷的最佳術中標誌(Icke等,2010)。我們應該記住,在梅克爾穴的內側唇處,岩結節被岩蝶韌帶的外側插入處覆蓋,在它後麵是外展神經。術中對岩結節和外展神經的早期識別可減少手術相關的風險和並發症。
外展神經不同於其他顱神經,特別是在前囟和海綿竇內的神經固定和沿其整個行程的成角方麵,在許多間接情況下會使神經有麻痹的風險。第六神經顱內走行時間較長,與頸動脈的空間關係密切。外科醫生必須對岩斜坡區和海綿竇的顯微外科解剖有詳細的了解,以避免損傷外展神經和ICA,此外,還應了解外展神經沿其走行可能出現的解剖變異,以防止神經功能障礙。
貢獻者:Wonil Joo, Fumitaka Yoshioka, Takeshi Funaki和Albert L. Rhoton, Jr.
內容來自朱偉,吉岡F, Funaki T, Rhoton AL, Jr.展神經的顯微外科解剖。中國阿娜特2012:25; 1030 - 1042。doi.org/10.1002/ca.22047.
神經外科188bet手机app圖譜很榮幸能夠繼承Albert L. Rhoton, Jr, MD的遺產。
請登錄發表評論。
一定要在社交媒體上關注我們的精彩內容並保持更新生活與科恩醫生的會議,關於手術技術的問題,以及更多!



您必須登錄才能查看這些材料。
的188bet手机app這幾乎完全取決於你的捐款。
沒有你們的大量捐贈,我們無法繼續進行地圖集。
請承諾每年至少捐款250美元給地圖集。如果沒有這個承諾,Atlas將很快需要付費訂閱,世界上許多病人的治療依賴於它的外科醫生將無法獲得它。
現在請捐!
沒有你們的大量捐贈,我們無法繼續進行地圖集。請承諾每年至少捐款250美元給地圖集。
如果沒有這個承諾,Atlas將很快需要付費訂閱世界各地的許多外科醫生將無法獲得它,他們的病人的治療依賴於它。現在請捐!