

你可以有所作為。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
現在請捐!
最後更新:2021年4月9日
對象進入第四腦室的兩種最常見的手術途徑是橫腸路和端瓣入路。本研究的目的是比較通過這些方法獲得的顯微解剖和曝光。
方法10例福爾馬林固定標本以逐步解剖的方式模擬經蟲和端瓣手術入路。利用隱身圖像製導技術比較了使用這些方法獲得的曝光和工作角度。
橫斷麵和端瓣入路提供了從導水管到obex的整個第四腦室底的喙側長度。此外,兩種入路均可進入第四腦室底的整個寬度。兩種入路的主要區別在於暴露側隱窩和Luschka孔。端瓣入路暴露了外側和上外側隱窩和Luschka椎孔,而不是橫椎入路。經蚓側入路提供了一個至少穿過蚓側下三分之一的切口,與端瓣入路相比,在進入第四腦室吻側半部分時,術者的工作角度略有增加。
結論經蟲側入路可以更好地看到第四腦室頂部上半部的內側部分。端瓣入路沒有切開小腦的任何部分,增加了外側隱窩和Luschka孔的暴露。
第4腦室最常見的兩種手術入路是經蚓入路和端瓣入路。第一種方法是切開小腦下蚓部,並將蚓部的兩半向相反的方向縮回。1、3、6、11、12在第二種入路中,形成第四腦室頂部下半部分的脈留膜和下髓膜被打開,下腦室被縮回為一個單位,以提供進入第四腦室的暴露。17日,20日22兩種入路之間的技術差異和限製兩種入路手術視野的解剖結構導致了第四腦室底、側隱窩和Luschka孔的暴露差異。本研究的目的是描述和比較經蚓和端瓣入路的顯微解剖特征,並將這些特征與通過每種入路獲得的暴露相關聯。
本研究檢查了10例福爾馬林固定標本,其中動脈灌注紅色矽膠,靜脈灌注藍色矽膠。在操作顯微鏡設置為3 - 40的輔助下,以逐步的方式解剖標本,以模擬使用橫斷麵和端瓣入路可獲得的暴露。特別注意的是在每種方法中限製可視化的解剖結構。
10具屍體頭顱中有3具使用MR成像進行研究,並使用標準協議在Stealth工作站注冊數據。使用3特斯拉磁共振成像係統(Magnetom Allegra;西門子醫療解決方案公司,馬爾文,賓夕法尼亞州),並轉移到隱形圖像製導工作站(美敦力外科導航技術公司,路易斯維爾,CO)。十個用於圖像配準的基準標記被連接到皮膚上矢狀竇和頂枕區。頭部按半仰臥位提供的方向放置,通過中線垂直皮膚切口進行枕下開顱手術。建立了三維模型,並將動態參考陣列固定在屍體上。將樣品配準到3D模型和圖像上,估計精度優於2毫米。在三維模型和三個正交的MR圖像上使用活動探針指示手術暴露。這些圖像通過屏幕捕捉記錄下來。通過每個入路到第四腦室的Luschka暴露的上、下、外側、上外側和孔在直接顯微鏡可視化下使用圖像引導確定。
我們比較了經椎弓根和端瓣入路的手術角度。從矢狀麵第四腦室底部測量角度。角的頂點被放置在沿著心室底的三個位置:渡槽,從obex到渡槽下邊界的距離的中點(50%點),以及相同距離的75%點。
第四腦室的手術入路通過小腦枕下或後表麵,位於橫竇下方和乙狀竇之間。蚓麵在小腦後切骨內折疊形成枕下皮質麵,是小腦後表麵的一個深垂直凹陷(圖1)。小腦後切骨內蚓麵形狀類似於鑽石,其上部稱為金字塔。蚓麵下半部分在扁桃體之間向下突出,稱為小舌,因此模仿口咽部的解剖結構(圖1)。扁桃體吻側部分的內側邊緣與小舌的漸細邊緣相鄰。門骨內的蚓條在金字塔和小舌的交界處是最寬的。在下方,小腦後切骨與小腦小葉相連,小葉小葉是扁桃體之間的裂口,通向Magendie孔。
扁桃體是阻斷第四腦室尾部的最突出的結構,被認為是半球形的組成部分。扁桃體是卵形結構,沿其上外側邊界附著於小腦半球的其餘部分,而每個扁桃體的其餘部分是遊離表麵(圖1)。每個扁桃體的前表麵和內表麵是重要的標誌,當接近第四腦室時可識別。前表麵麵對小腦延髓裂,這是扁桃體和延髓後表麵之間的裂縫。扁桃體的內側通過一個狹窄的裂口(小葉)相對,小葉通向第四腦室底部的下部。
第四腦室的頂部是一個帳篷狀的結構。屋頂的頂端,即尖頂,是屋頂最大高度和寬度的地方。頂板把屋頂分成上下兩部分。上半部頂板從渡槽向外側和後方擴展至頂部和側隱窩水平(圖2和圖3)。上半部頂板由上髓膜在內側形成,上髓膜在頂部與下髓膜相連,並在外側與上、下小腦梗內表麵相連。小腦上梗的纖維在齒狀核中出現,上升形成側壁上部的腦室表麵(圖3)。
頂膜的下部由脈絡膜和下髓膜膜構成(圖2和圖4)。下髓膜膜是結節和濾泡之間連接的膜性殘餘物,濾泡形成絮凝結節小葉它是一層薄薄的雙側神經組織,從結節內側延伸並融入每個側隱窩的背緣,在外側形成每個小葉的花序梗(圖2和圖4)。尾側,下髓膜附著於脈絡膜尾部。脈絡膜底部在其各層之間包含脈絡膜動脈和靜脈的血管層,脈絡膜叢從其腦室表麵突出(圖4)。重要的是,在形成第四腦室頂下部的結構中沒有已知的功能性神經組織。
端瓣連接線,即下髓膜與端脈絡膜的連接線,從結節向外側延伸至每一個側隱窩(圖4)。端瓣沿狹窄的脊(帶膜)連接到基底的下外側邊緣,並在網膜處彙合。脈絡背有三個開口通往蛛網膜下窩:位於側隱窩的成對的Luschka孔和位於第四腦室尾端內側的Magendie孔(圖4)。

圖1所示。顯示屍體大腦標本後視圖的照片。圖示小腦枕下麵和小腦髓裂。圖A和B顯示一個標本,圖C和D顯示另一個。答:枕下麵位於乙狀竇和橫竇之間的下方,是寬雙側枕下開顱術中露出的麵。蚓部位於凹陷處,小腦後切骨位於兩個半球表麵之間。小腦延髓裂向上延伸至小腦和延髓之間。小葉在扁桃體之間向上延伸,並通過Magendie孔與第四腦室相通。左異食癖沿扁桃體下極下方延伸至小腦髓裂下緣,並支配部分枕下表麵。B:左扁桃體向外側收縮,小舌向內側收縮,露出第四腦室頂的下部。 The inferior portion of the roof is formed by the tela choroidea and the inferior medullary velum. The bifurcation of the PICA into the medial and lateral trunks has been retracted to show the lateral recess. Some branches of the medial trunk, which supplies the vermis, course along the uvulotonsillar space along with the vein of the cerebellomedullary fissure. C: The right tonsil has been retracted medially from the biventral lobule. The tonsils, the most prominent structures blocking access to the caudal portion of the fourth ventricle, are attached to the cerebellar hemisphere along their superolateral borders. The fissure between the tonsil and the biventral lobule is called the tonsillobiventral fissure. D: Enlarged posterior view of the same hemisphere. Both tonsils have been retracted laterally to expose the inferior medullary velum and the tela choroidea. The choroidal arteries course along the tela choroidea, from which the choroid plexus projects into the roof of the fourth ventricle. The inferior vermian surface within the posterior cerebellar incisura has a diamond shape, the upper portion of which is called the pyramid. The lower half projects downward between the tonsils and is called the uvula. The nodule is hidden deep in relation to the uvula. The medial margin of the rostral portion of the tonsils borders the tapering edges of the uvula. The strip of the vermis within the incisura is broadest at the junction of the pyramid and uvula. The right PICA bifurcates into lateral and medial trunks, which course along the uvulotonsillar space. The lateral recess, a narrow pouch formed by the union of the roof and floor, is covered caudally by the tela choroidea. A. = artery or arteries; Cer. = cerebellar or cerebello; Chor. = choroidal, Fiss. = fissure; For. = foramen; Inf. = inferior; Lat. = lateral; Med. = medial or medullary; Post. = posterior; Tons. Bivent. = tonsillobiventral; Tr. = trunk.
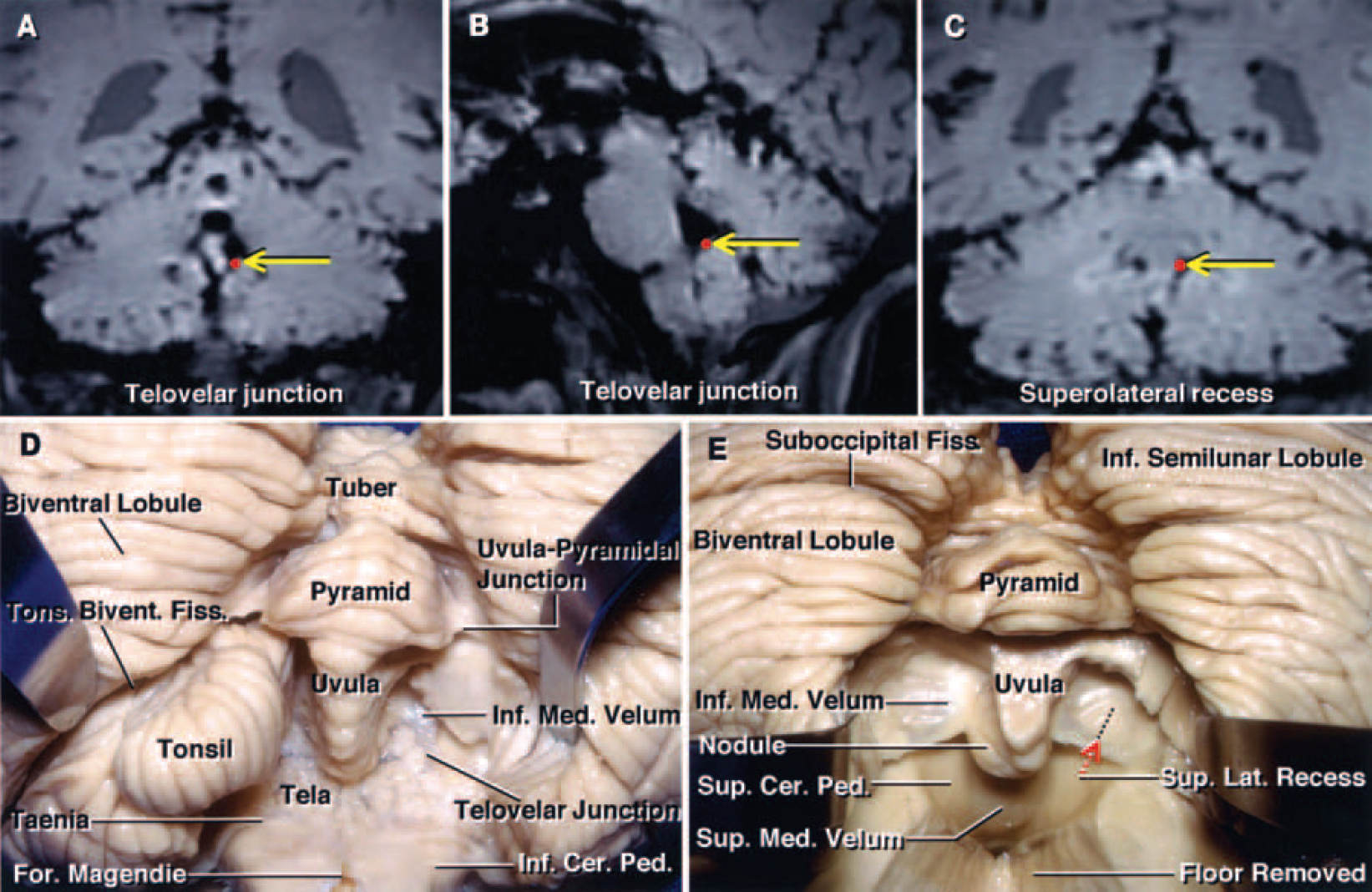
圖2所示。A - C:從隱身工作站獲得的屍體大腦的冠狀(A和C)和矢狀(B) MR圖像,顯示端velar連接處(A和B中黃色箭頭指示的紅點)和上外側隱窩(C中黃色箭頭指示的紅點)的位置。D和E:屍體大腦標本照片,顯示小腦枕下表麵和第四腦室下部的逐步剝離。D:左雙腹小葉收縮,可見扁桃體雙腹裂。右扁桃體經扁桃體上外側緣的扁桃體梗分開切除。小舌在扁桃體之間向下延伸,模仿口咽的解剖結構。小腦後切口內最寬的蚓狀帶是垂錐體連接處,它限製了扁桃體的側向收縮。端瓣連接處是端部與被膜的連接線。E:切除扁桃體和部分基底,露出上髓膜和上外側隱窩。下髓膜是一層薄薄的雙側神經組織,從結節內側延伸並與每個側隱窩的背緣混合,形成每個小葉的側梗。在經蚓側入路時,穿過蚓部下部的切口暴露了下麵的結節,必須切開才能進入第四腦室。 This incision through the vermis is limited by the position of the superior medullary velum, which is closely related to the anterior portion of the nodule. The superior medullary velum forms the medial part of the superior half of the roof and expands laterally and posteriorly from the aqueduct to the level of the fastigium and lateral recess. The superolateral recess, located within the fourth ventricle and lateral to the uvula and nodule, is medial to the superior cerebellar peduncles and lies anterior to the upper edge of the inferior medullary velum. Ped. = peduncle; Sup. = superior.
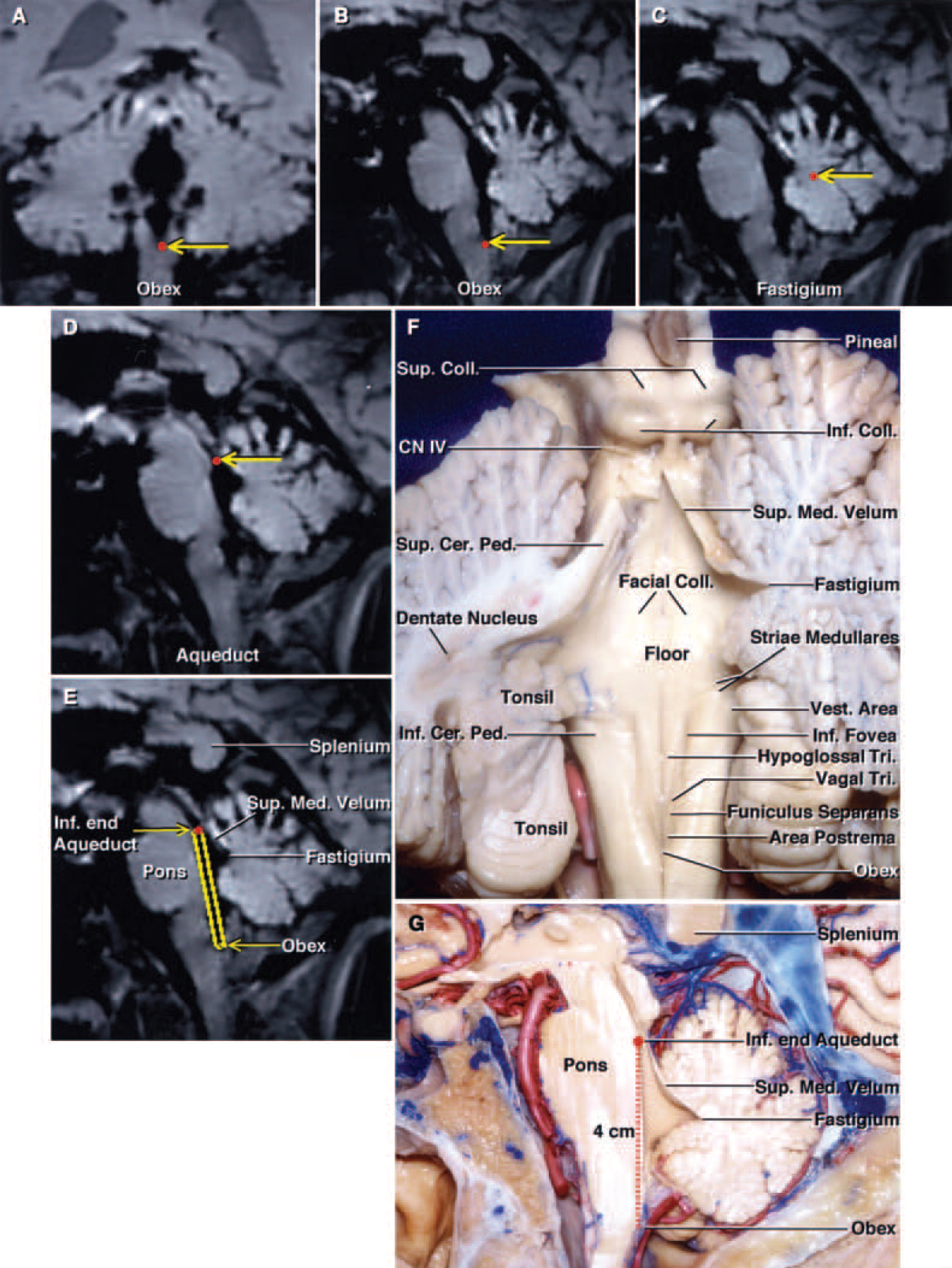
圖3所示。A-E:隱形磁共振圖像顯示沿第四腦室底部和頂部的解剖標誌(黃色箭頭指示的紅點)。冠狀麵(A)和矢狀麵MR圖像(B)顯示了obex的位置。矢狀麵MR圖像(C和D)顯示了頂部和導水管。矢狀麵MR圖像(E)顯示第四腦室底部及其與上髓膜和頂膜的關係。(該大腦部分與圖g所示的屍體矢狀麵幾乎位於同一水平麵上)F:小腦在中線處被切開,左半部分在斜冠狀麵上被進一步切片,以顯示扁桃體吻端極與齒狀核的關係。齒狀核似乎包裹著扁桃體。小腦上脛纖維起於齒狀核,並在小腦上脛內側上升。骨髓紋穿過地板的中部。 The vestibular area, the portion of the floor that is lateral to the median eminence and the sulcus limitans, is located at the lateral limit of the floor of the fourth ventricle. The inferior fovea is a depression in the sulcus limitans located lateral to the hypoglossal triangle. The median eminence contains the facial colliculi in its upper part and the hypoglossal and vagal triangles and the area postrema in its lower portion. The median eminence is crossed by the funiculus seperans. The trochlear nerves arise below the inferior colliculus. G: Sagittal section of a hemisphere. The full length of the floor of the fourth ventricle from the inferior edge of the aqueduct to the obex is approximately 4 cm. The roof of the fourth ventricle is a tent-shaped structure. The apex of the roof, the fastigium, is the site of the roof’s greatest height and width. The superior half of the roof expands posteriorly from the aqueduct to the level of the fastigium. This sagittal section corresponds to the Stealth MR image in panel E. CN = cranial nerve; Coll. = colliculi or colliculus; Tri. = triangle; Vest. = vestibular.

圖4所示。A - C:從隱身工作站獲得的屍體頭部的冠狀(A),矢狀(B)和軸向(C) MR圖像,顯示了側隱窩(黃色箭頭表示的紅點)。三幅圖像上的點都是一樣的而且都來自同一具屍體。D和E:另一具屍體標本的照片顯示小腦枕下表麵的階梯式剝離。兩個扁桃體都已向上外側縮回,脈絡膜下半部的左側已打開(D)。脈絡膜叢從脈絡膜下側的室麵延伸至第四腦室。脈絡膜側向小腦下梗上方延伸,形成外側隱窩的後壁。D (E)片顯示的結構視圖。脊膜側向右側收縮,暴露出第四腦室的整個底部和導水管。第四腦室與橋小腦角相連,通過側隱窩的Luschka孔。頂的上半部在內側由上髓膜形成,外側由上小腦梗的內表麵形成。下髓膜向外側與小葉的花序梗混合,向內側與結節表麵混合。 F: The left cerebellar hemisphere, the vermis, and the medial portion of the right cerebellar hemisphere have been removed to expose the full length of the floor of the fourth ventricle. The trochlear nerves arise inferior to the inferior colliculus. The superior and inferior cerebellar peduncles face the surface of the ventricle. The median sulcus divides the floor vertically in the midline. The sulcus limitans divides each half of the floor of the fourth ventricle longitudinally into a medial strip, the median eminence, and a lateral portion, the vestibular area. The sulcus limitans is most prominent at the level of two dimples, the superior and inferior fovea. The facial colliculus is medial to the superior fovea and median eminence. The locus ceruleus, a darkened area of cells, is located at the rostral end of the sulcus limitans. G: Anterolateral view of the brainstem and petrosal surface of the cerebellum, corresponding to the area demonstrated by the Stealth MR image in panel A. The choroid plexus protrudes from the lateral recess and foramen of Luschka behind the glossopharyngeal and vagus nerves. The trigeminal nerve arises from the midpons. The abducent nerve arises in the medial portion and the facial and vestibulocochlear nerves at the lateral end of the pontomedullary sulcus. The hypoglossal nerves arise anterior to the olives and the glossopharyngeal, vagus, and accessory nerves arise posterior to the olives. The anterior inferior cerebellar artery arises at the pontine level and courses by the abducent, facial, and vestibulocochlear nerves. The right PICA arises at the level of the vertebrobasilar junction, courses in relation to the lower cranial nerves, and passes dorsally around the medulla oblongata near the lower portion of the tonsil. H: Enlarged view of the foramen of Luschka with the glossopharyngeal and vagus nerves retracted to expose the foramen and the structures forming the lateral recess. The flocculus protrudes laterally from the inferior margin of the middle cerebellar peduncle dorsal to the facial and vestibulocochlear nerves. The rhomboid lip, a sheet of neural tissue attached to the lateral margin of the floor of the fourth ventricle, has been retracted to show the choroid plexus protruding from the lateral recess and the foramen of Luschka. A.I.C.A. = anterior inferior cerebellar artery; Bas. = basilar; Mid = middle; Plex. = plexus; Sul. = sulcus; V. = vein; Vert. = vertebral.
第四腦室頂的下半部分與小腦髓裂密切相關。裂隙有腹壁和背壁。腹壁由髓質後表麵、下髓質膜和脈絡膜背壁組成(圖1)。背壁由小舌、扁桃體和雙腹小葉組成。小腦延髓裂向上延伸到側隱窩的水平,並通過Magendie孔和環繞扁桃體上表麵的大池與第四腦室相連;該裂通過Luschka孔與橋小腦裂相通(圖4)。
異食癖與小腦延髓裂、第四腦室頂下半部分和枕下表麵密切相關。PICA起源於延髓前外側緣的椎動脈,靠近下顱神經,並通過位於扁桃體、蚓部和小腦半球之間的一係列深裂(圖1)。PICA分為五個節段:前延髓、外側延髓、扁桃體延髓、端速扁桃體和皮質節段。15在經椎體和端瓣入路時,最常暴露的異食性腺節段是端速扁桃體節段,它位於扁桃體(下圖)和端部脈絡膜和軟膜(上圖)之間的裂口中。pica在扁桃體周圍的通道中分叉為內側主幹和外側主幹(圖1)。內側主幹供應蚓部,外側主幹供應大部分半球和扁桃體表麵。在接近第四腦室的過程中,經常會碰到兩個軀幹。
小腦延髓裂靜脈是穿過第四腦室下部的最大靜脈。它起源於小葉結節和小舌的外側邊緣,沿端瓣連接處向外側延伸,並向尾端延伸至小腦梗,到達橋小腦角。它流入靜脈然後流入上岩竇。18小腦延髓裂靜脈的支流引流扁桃體、下蚓部、下髓膜、脈絡膜和附屬脈絡膜叢的部分,以及心室白質和齒狀核。
第四腦室的底部是一個菱形結構,其吻端位於腦橋後方三分之二處,尾端位於延髓後方三分之一處(圖2和圖4)。其顱尖位於大腦導水管的水平,尾端止於腦管,腦管位於Magendie孔的前方和深部。第四腦室底部的中間部分延伸到側隱窩。前庭區位於第四腦室底部的外側界限(圖3)。前庭核位於前庭區下方,形成一個圓形凸起,直接延伸到側隱窩。延髓紋位於前庭區吻側,從側隱窩區域穿過小腦下梗向中線橫向延伸(圖3)。
第四個腦室與橋小腦角通過側隱窩的Luschka孔相連,側隱窩是一個由屋頂和地板結合而成的狹窄袋(圖4)。每個側隱窩的腹壁是由地板的連接部分和菱形唇構成的,菱形唇是一層片狀的神經組織。吻側部分由小腦梗的尾緣組成。每個側隱窩的尾部由脈絡膜端組成,從帶絛蟲的外側延伸到小葉(圖4)。
最古老和最廣泛使用的第四腦室手術入路包括在枕下表麵劈開下蚓部。1, 11、12通過下蚓部的切口範圍描述得很差。根據病變區域的位置和大小,切口通過小舌、錐體、塊莖和蚓部的小葉延伸可變的距離。大多數作者主張將蚓部切口限製在必要的最小長度,以避免與蚓部分裂相關的並發症。23同樣,在我們的研究中,通過下蚓部切開並延伸至第四腦室。我們將橫斷麵的切口擴大到最大,包括下蚓部直到頂部,但沒有延伸到上髓膜的下邊緣。在功能上,小腦上梗的交叉纖維位於上髓膜的深處,上髓膜是小腦上梗之間的一層薄薄的白色物質。蚓部切口暴露了下麵的結節,必須將其與脈留膜端和下髓質膜一起切開,以進入第四腦室(圖5)。
下蚓部兩半的收縮在下蚓部的兩個邊緣之間提供了大約1到2厘米的工作空間。蚓體和扁桃體橫向收縮後,可以遵循的telovelotonsillar段之間的雙邊異食癖,在左、右段不犧牲任何的主要分支血管的靜脈(圖5)。cerebellomedullary水平裂縫追逐的中線蠕蟲的切口沿紗布choroidea偽劣髓軟齶在三個半球的紗布後(圖5)。choroidea偽劣髓軟齶通過中線已經打開切口,從渡槽到obex的整個地板長度(平均長度4厘米)可以暴露(圖5)。側向,暴露的極限在髓紋水平最大。前庭區的初始內側部分是暴露的外側極限。上髓膜中段為暴露極限。在此時的解剖過程中,在我們的任何標本中,通過經蟲入路暴露側隱窩和Luschka孔都是不可能的。暴露側隱窩需要切除一部分蚓麵,而暴露Luschka孔則需要進一步收縮扁桃體極。3、13
在我們通過第四腦室獲得最大曝光量後,將隱形圖像引導引入解剖場(圖5)。在沿著第四腦室底部的三個位置測量的橫斷麵入路的平均手術角度在渡槽處為38英尺,在從obex到渡槽距離的中點為84英尺,在75%點為72英尺。上髓膜是限製矢狀麵工作角度的主要解剖結構。當我們暴露第四腦室的四分之一吻側時,局限性最為明顯,當我們向中外側移動時,手術視野減小。頂部和上髓膜的下部限製了導骨與渡槽距離的75%處的工作角度。在第四腦室底部長度的中點處,工作角度急劇增加。此時,暴露僅局限於蚓部切口上緣。

圖5所示。A-D:屍體標本照片顯示經蟲麵進入第四腦室。小腦枕下麵(A)。最古老和最廣泛使用的第四腦室手術入路包括在枕下麵切開下蚓部。圖A (B)所示部分解剖結構的放大視圖。兩個扁桃體已向外側縮回,露出蚓部下部、錐體和小舌。經蚓部入路進入第四腦室的切口通常被描述為穿過蚓部下部(虛線)。兩種pica都繞過扁桃體的下極到達小腦髓裂的下緣。切割蚓部下部,蚓部和扁桃體橫向縮回(C)。穿過蚓部的切口暴露了下麵的結節,必須切開該結節才能暴露頂板的下部。下蚓部兩半的收縮在下蚓部的兩個收縮邊緣之間提供了大約1 - 2cm的工作空間。隨著蚓體和扁桃體的橫向收縮,可以沿著雙側PICAs的左右端慢扁桃體節段進行工作,而不犧牲血管的任何主要分支。小腦髓裂靜脈沿下髓膜橫向延伸。 Retraction of the two halves of the nodule and the opening of the tela choroidea and inferior medullary velum through a midline incision provide access to the full length of the floor (mean length 4 cm) from the aqueduct to the obex (D). The transvermian approach provides a wide exposure of the midline superior half of the roof of the fourth ventricle and the superior medullary velum. E–H: Stealth MR images of the transvermian dissection demonstrating the superior, inferior, and lateral limits of exposure (red dots indicated by yellow arrows). The superior limit of the transvermian exposure is at the inferior edge of the aqueduct (E). The inferior limit of the transvermian exposure is at the obex (F) and the right and left lateral limits are at the level of the striae medullaris (G and H). The medial edge of the vestibular area is the lateral limit of exposure. I and J: Sagittal (I) and coronal (J) Stealth MR images obtained during the dissection, demonstrating the trajectory of the transvermian approach (yellow rectangles leading to red dots). The fastigium and the inferior portion of the superior medullary velum are the main anatomical structures that limit the working angle to the rostral one fourth of the floor of the fourth ventricle during the transvermian approach and this is demonstrated in the sagittal plane.
暴露小腦枕下表麵後,打開兩側的懸垂扁桃體和髓扁桃體間隙,同時在扁桃體和雙腹小葉周圍進行外側和深部解剖,不分離任何神經組織(圖6-8)。扁桃體下緣暴露,剝離延伸到扁桃體內側和小舌鄰近邊緣之間。對著小舌的扁桃體表麵向上外側向入路一側收縮,小舌向另一側收縮,露出下髓膜和脈絡膜。特別注意異食癖的位置和分叉進入內側和外側主幹。在這10個標本中,有3個異食癖分岔暴露於懸垂扁桃體空間下端附近,在端瓣連接處附近。如果分叉沿切口位置出現,在我們沿著掌部和下髓膜切開之前,向外側收回分叉比向內側收回分叉更容易(圖6和圖8)。
端瓣切口可分為三部分。切口的第一部分打開了脈絡膜背部,從腦室頂下部靠近Magendie孔的下方開始,向上延伸到腦室背部與下髓質膜的交界處(圖6)。在我們打開脈絡膜背部後,在某些半球可以看到第四腦室底的完整長度。第二部分是將切口向上延伸穿過下髓質膜,暴露在懸垂扁桃體間隙的深處。在一些標本中,橫斷小腦髓裂靜脈,它穿過下髓膜。切開下髓膜暴露了同側上外側隱窩,並提供了通向所有半球第四腦室整個底部的通道(圖6和圖8)。打開下髓膜也增加了上髓膜靠近頂端的下部的暴露。通過一側的懸垂扁桃體空間打開tela和下髓膜,可以限製對另一半地板外側部分的暴露;然而,將暴露移到對麵的懸垂扁桃體空間,並打開tela和velum提供了與另一側相同的暴露。第三個切口在扁桃體和延髓之間,通過形成外側隱窩下後壁的端部,提供了通往外側隱窩全長和Luschka孔的額外通道(圖8)。
使用隱形圖像引導來展示通過端瓣入路獲得的解剖暴露(圖7和圖9)。在沿著第四腦室底部的三個位置,端瓣入路的平均手術角度在渡槽處為30°,在75%處為67°,在中點為84°。該入路暴露的主要局限性是上髓膜和錐體與小舌的交界處(圖7-9)。小舌和錐體的交界處是後切膜間隙內最寬的蚓部帶,它分別限製了扁桃體和小舌在懸垂扁桃體間隙的外側和內側回縮(圖3和圖8)。在端瓣入路時,所有標本的手術角度都受到懸垂錐體交界處的限製。
在橫髓和端瓣入路中,手術入路角度受上髓膜的限製,當患者向中外側移動時,上髓膜的結構並不均勻。上髓膜與第四腦室底部在中線處形成的角度比其橫向形成的角度大。在端瓣入路中,第四腦室從中線通過上外側隱窩入路,這是手術角度減小的部分原因。兩種入路手術角度的平均差異不超過8°,有利於經肝入路。
經椎弓根和端瓣入路可以很好地暴露第四腦室的整個底部。經蚓麵入路采用蚓麵中線切口,可以更好地暴露第四腦室頂部中線上半部和頂部。在所有標本中,端velar入路提供了進入Luschka側隱窩和孔的額外通道。
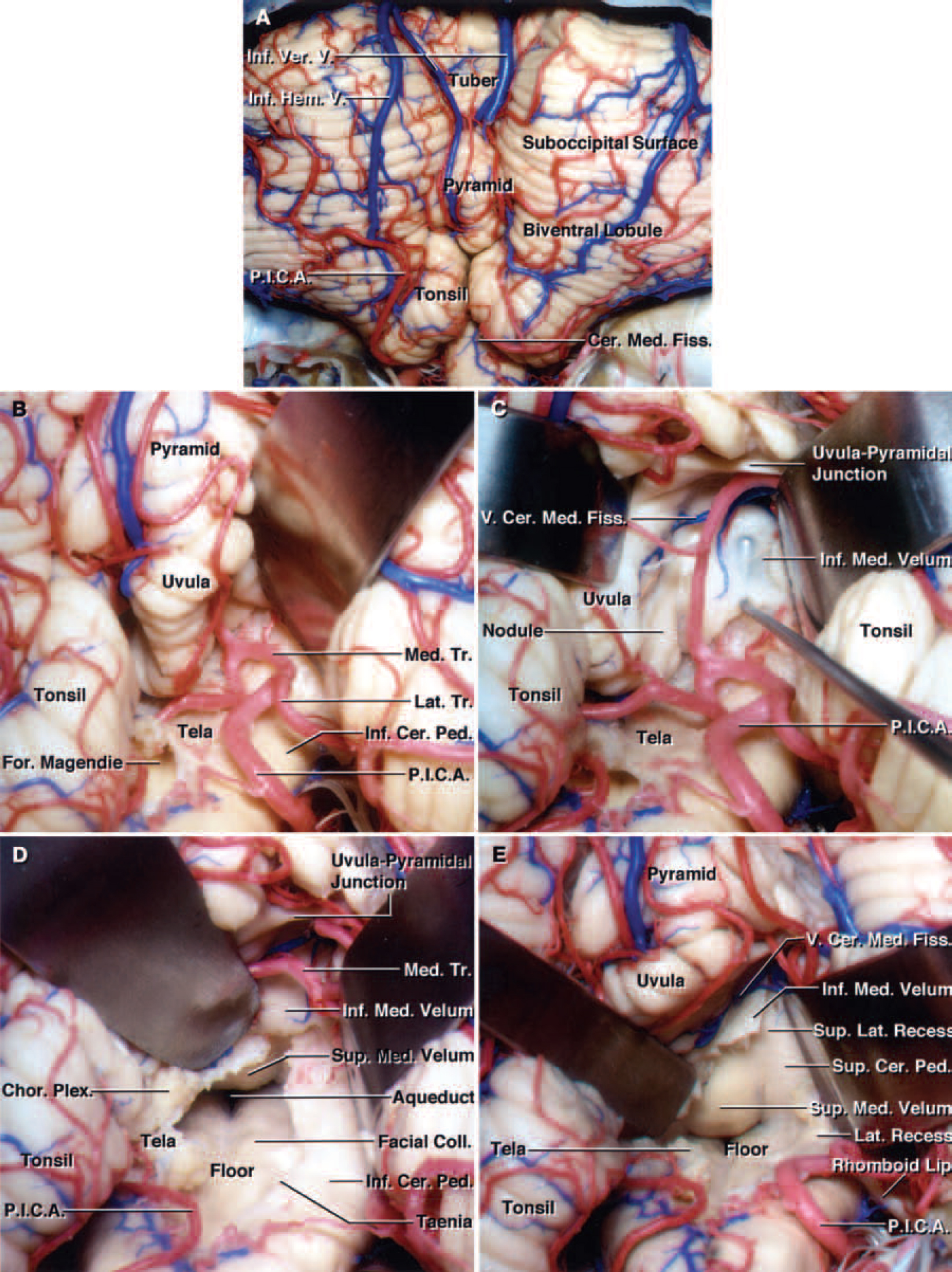
圖6所示。屍體大腦標本照片顯示端瓣入路至第四腦室。答:暴露扁桃體和雙腹小葉後,打開兩側的懸垂扁桃體和髓扁桃體間隙。B:扁桃體已向外側縮回,暴露右側懸垂扁桃體間隙,特別注意保存異食癖及其進入內側和外側主幹的分支。異食癖分岔位於懸垂扁桃體空間下端附近,靠近端瓣連接處,約30%的標本中有異食癖分岔。C:右扁桃體向上外側收縮,小舌向內側收縮,露出右小舌扁桃體空間。將直角神經鉤的尖端置於上外側隱窩的下髓膜下。鉤的尖端可以透過薄的下髓膜看到。D:小舌已向超內側收縮,右扁桃體向超外側收縮,以達到最大程度的顯像。PICA分支已向外側縮回,而不犧牲血管的任何分支。 If the PICA bifurcation is present at the uvulotonsillar space along the site of the telovelar incision, it is easier to retract it laterally before creating an incision along the tela than to retract it medially in most hemispheres. The incision along the tela choroidea in the right half of the roof has been extended to the telovelar junction. The entire floor of the fourth ventricle from the obex to the aqueduct has been exposed. E: The right half of the inferior medullary velum has been divided to expose the superolateral recess and maximize the exposure along the medial superior half of the roof and superior cerebellar peduncle. Opening the inferior medullary velum increases the exposure of the lower portion of the superior medullary velum near the fastigium. The vein of the cerebellomedullary fissure, which crosses the upper end of the inferior medullary velum, has been preserved. Retracting the right tonsil superolaterally provides access to the lateral recess and exposes the rhomboid lip. Hem. = hemispherical; Ver. = vermian.
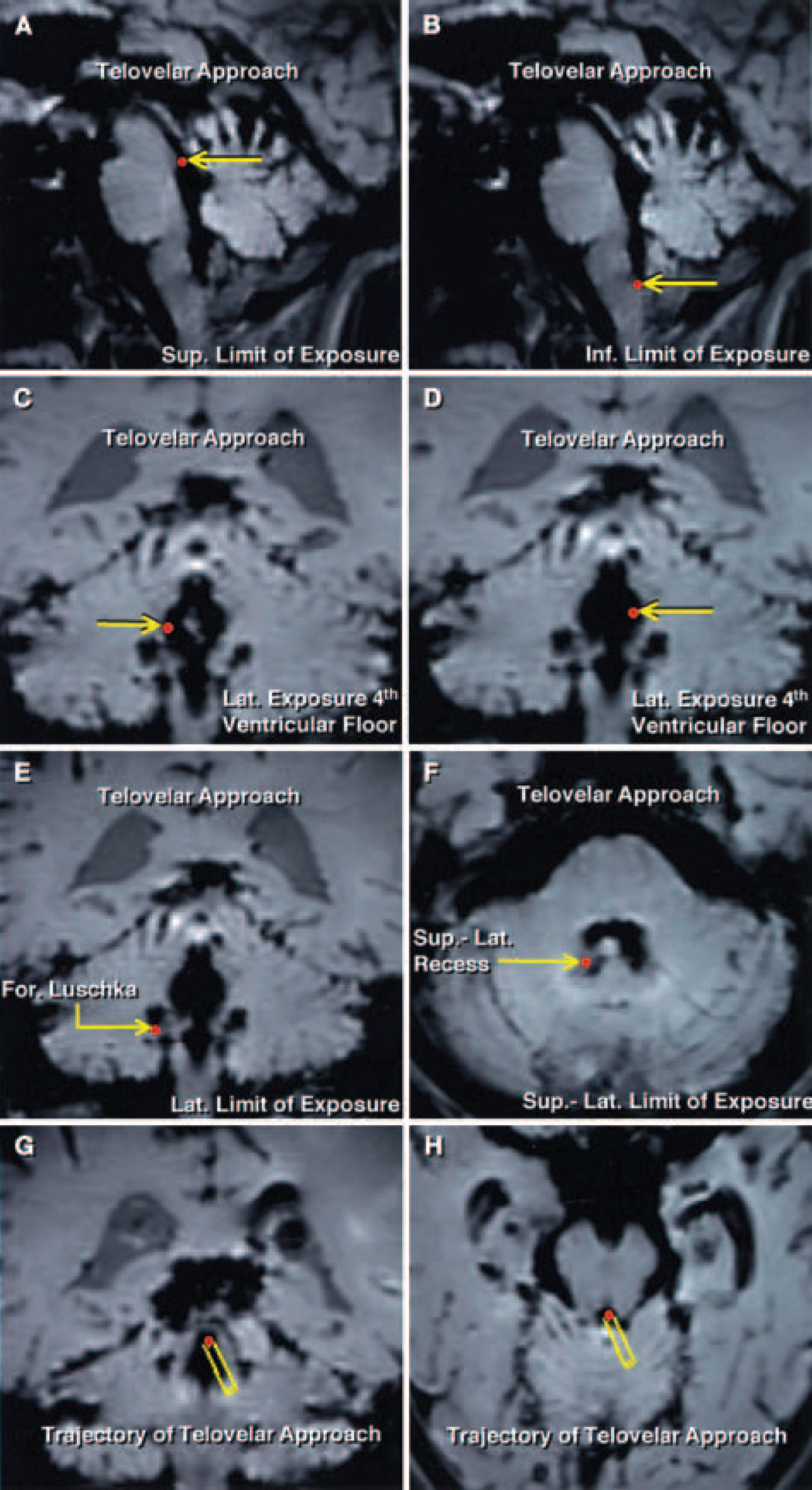
圖7所示。Telovelar方法。矢狀位、冠狀位和軸向隱身MR圖像的手術暴露極限(紅點由黃色箭頭表示)。A:沿著第四腦室底部暴露的上限值是導水管。B:端瓣入路提供了從導水管到腹壁的第四腦室底部的整個長度,這是暴露的下極限。C和D:第四腦室底部暴露的外側界限位於髓紋水平,靠近外側隱窩的內側邊緣。E:將扁桃體上外側抬高,暴露出外側隱窩的全長和外側隱窩下外側端的Luschka孔。F:上外側暴露極限為上外側隱窩,隻有切開下髓膜才能暴露。G和H:在解剖過程中獲得的冠狀麵和軸向隱身MR圖像顯示了端瓣入路的軌跡(黃色矩形通向紅點)。在端瓣入路中,第四腦室從中線穿過懸垂扁桃體間隙,通過打開端脈絡膜和小舌外側的下髓膜進入。

圖8所示。屍體大腦標本的照片,顯示在逐步解剖中橫向和端velar暴露的比較。A和B:橫向入路。穿過蚓部下部的橫切切口暴露了底層的結節,必須切開才能進入第四腦室(A)。穿過蚓部的切口受限於位於結節前上邊緣的上髓膜的位置。下蚓部成對半部分的收縮提供了切口蚓部邊緣之間約1至2厘米寬的暴露。放大視圖(B)。隨著脈絡膜尾部和下髓質膜通過橫貫切口的打開,從導水管到腹壁的完整長度(平均長度4厘米)可以暴露出來。上髓膜限製了暴露的上部。經蟲側入路可以更好地暴露第四腦室頂部上半部的中線部分。橫斷麵暴露的外側界限延伸到髓紋和前庭區域的內側邊緣。氟:Telovelar方法。 The tonsils have been retracted superolaterally to expose the tela choroidea, inferior medullary velum, and both lateral recesses (C). The lateral limit of the exposure achieved is the foramen of Luschka, where the choroid plexus protrudes behind the glossopharyngeal and vagus nerves. The uvula has been retracted medially and the right tonsil laterally, and the tela and inferior medullary velum have been opened to expose the entire length of the floor of the ventricle (D). The aqueduct and the obex are the superior and inferior limits of the exposure along the floor. View of structures shown in panel D (E). The lateral limits of the exposure along the floor of the fourth ventricle are similar to those provided by the transvermian approach and located at the level of the striae medullaris, near the medial edge of the lateral recesses. Incising the inferior medullary velum provides access to the superolateral recess and most of the midline superior half of the roof of the fourth ventricle formed by the the superior medullary velum. View of another specimen (F). Both tonsils have been elevated to expose the full length of the lateral recesses. The rhomboid lip at the lateral end of the lateral recess has been exposed on the right side. The left PICA bifurcates into medial and lateral trunks at the inferior end of the uvulotonsillar space.

圖9所示。疊加在屍體大腦切片照片上的圖表,展示了沿著第四腦室底部的橫貫入路和端瓣入路的手術角度比較。沿第四腦室底矢狀麵測量角度。角的頂點被放置在沿著第四腦室底部的三個位置:渡槽,從obex測量到渡槽下邊界的距離的中點(50%點),以及該距離的75%點。A:矢狀麵顯示小腦枕下表麵蚓部。蚓部突出的部分是去裂體(橙色)、小葉(紫色)、塊莖(藍色)、錐體(黃色)、小舌(綠色)和結節(淺紅色)。頂脊是第四腦室頂的頂端,它將腦室頂分為上、下兩部分,位於中點和75%點之間,接近矢狀麵中段。切口的上限(虛線)通過小舌、錐體、塊莖和小葉的下部延伸到頂部,但沒有進入上髓膜的下邊緣。B:經腹膜入路和端瓣入路可以很好地暴露從腹壁到導水管的第四腦室的整個底部。渡槽測得的橫斷麵和端麵入路的平均手術角度分別為38′(角A)和30′(角B)。 In the sagittal plane the exposure gained at the aqueduct when the telovelar approach is used is shaded green. The mean difference between the operative angles of the two approaches at the aqueduct did not exceed 8 ̊ in favor of the transvermian approach (shaded light red). In both the transvermian and telovelar approaches, the operative angle of approach was limited by the superior medullary velum in the sagittal plane. The limitation was most significant when exposing the rostral end of the fourth ventricle near the aqueduct. The working angle decreases when moving away from the midline. In the telovelar approach, the fourth ventricle is approached off the midline, which accounts in part for the decrease in operative angle. The uvulopyramidal junction, the broadest strip of vermis within the posterior incisural space, limited the lateral and medial retractions of the tonsil and the uvula at the uvulotonsillar space, respectively. C: The mean operative angles of the transvermian and telovelar approaches measured at the 75% point were 72 ̊ (Angle A) and 67 ̊ (Angle B), respectively. In the sagittal plane, the exposure at the 75% point for the telovelar approach is shaded green. The mean difference in the working angle gained through the transvermian approach at the 75% point is shaded light red. The lower edge of the superior medullary velum limited the working angle at the 75% point in both approaches and the uvulopyramidal junction accounts for the decrease in the operative angle in the telovelar approach. D: The operative angles of the transvermian and telovelar approaches measured at the midpoint along the length of the floor of the fourth ventricle were identical, 84 ̊ (Angle A). At the midpoint, the working angle gained in the sagittal plane is shaded blue. At the midpoint along the floor of the fourth ventricle, the working angle increased dramatically compared with the working angle at the aqueduct.
由於第四腦室的位置較深,且與腦幹的重要結構有關,因此接近第四腦室具有挑戰性。經腸壁入路是進入第四腦室病變最常用的方法。3、11、12另一種經小腦髓裂至脈絡膜底和下髓膜的入路提供了進入第四腦室的另一種途徑,已被越來越多的神經外科醫生使用。8、16、17、20、21、28盡管文獻中有一些關於端齶入路的顯微外科解剖及其臨床應用的報道,8,20,28其與更傳統的經椎弓根入路的比較尚未被研究。
關於端瓣入路的一個常見誤解是,由於工作角度減小和該區域暴露有限,難以接近延伸到第四腦室上半部分的病變。本研究的目的是比較橫向入路和端瓣入路的工作角度和限製暴露的解剖結構。
因為花花公子的聲明3.關於蚓部分裂而不影響功能的問題,帶蚓部分裂的經蚓入路已被廣泛使用。14日,25然而,經蟲側入路需要切開小腦皮層和功能區。小腦下蚓部分裂可引起蚓尾綜合征,導致軀幹性共濟失調的平衡障礙、步態障礙、頭部和軀幹的擺動以及眼球震顫。6、7此外,由於齒狀核位於與扁桃體上極相鄰和吻側的第四腦室頂部的後外側邊緣,當小腦蚓部分裂時,該核可能受損。28當齒狀核受損時,所產生的平衡紊亂比僅蚓部病變所觀察到的更為嚴重,並且常常伴隨著肢體自主運動時的有意震顫。蚓部下部的分裂也可能在小腦緘默症中起作用,小腦和第四腦室腫瘤切除後的一過性並發症。雖然小腦緘默症的確切解剖學基礎尚不清楚,但蚓部的下部,包括錐體、小舌和結節,已被涉及。2、4、5、21、24
在發表了該區域顯微外科解剖的詳細描述後,開始使用小腦髓裂的天然裂縫接近第四腦室。17日,19顯微26日,27日描述了沿“扁桃體ouveal”溝的中位下枕下入路治療第四腦室病變;然而,Matsushima等人首次報道了使用小腦延髓裂進入第四腦室而不分裂蚓部的方法。16隨後,不同的作者報道了該方法和令人滿意的結果。10日,28日資深作者(A.L.R.)在他的實踐中使用端齶入路超過20年,並沒有觀察到因打開端和軟膜而導致的臨床缺陷。我們最近介紹了通過端瓣入路暴露第四腦室的方法。20.
跨膜入路和端膜入路在幾個關鍵方麵是不同的。這些明顯的特征包括入路的方向和路線,縮回和犧牲的結構,縮回的方向,限製暴露的結構,以及暴露的區域。第四腦室或腦幹病變的生長位置和方向在理想入路的選擇中起著重要作用。病變主要位於蚓部並延伸至第四腦室,可通過經蚓部入路進入。位於室管膜表麵和第四腦室底的腫瘤通常不侵犯小腦,可通過端瓣入路進入。第四腦室腫瘤常延伸到側隱窩,最好的方法是抬高同側扁桃體並采用端瓣入路。橫斷切口的優點是位於中線,但小舌向另一側的輕微回縮使端瓣入路非常接近中線。obex,延髓後正中溝,Magendie孔在端瓣和橫斷麵暴露的下緣提供了有價值的標誌,將手術視野定位到中線。
在接近第四腦室底的四分之一吻側時,經橫斷麵入路在矢狀麵提供了稍大的工作角度。此外,通過經腸管入路可以更好地看到上髓膜和頂的中線下方部分。然而,經肝入路的主要缺點是側向暴露有限。暴露的外側界限是經蚓側入路中沿著第四腦室底部的前庭區初始部分,除非切除蚓部或扁桃體的一部分,否則無法到達外側隱窩。經蚓入路的另一個缺點是,由於蚓部切口、蚓部或扁桃體切除和蚓部分裂的兩半回縮所引起的醫源性神經損傷可能導致並發症。
Matsushima, et al .,17最近關於小腦延髓裂的解剖方法的報道,提出了三種不同的經小腦延髓裂入路的開放程序:廣泛型、外側壁型和外側隱窩型程序。在完全剝離懸垂扁桃體和髓扁桃體間隙後,我們能夠通過使用類似的切口獲得最大限度的暴露。我們的初始切口位於端脈絡膜沿線,與帶絛蟲相鄰,向上外側延伸至端瓣連接處。在開掌後沿著下髓膜和外側隱窩壁的後緣開一個切口。端瓣入路以類似於橫臥入路的方式完全暴露第四腦室底。此外,上外側隱窩和沿外側隱窩的結構,包括Luschka孔,可以在不切除大腦或調整牽開器的情況下進入。
由於兩種解剖結構,可以預期在上髓膜下部靠近頂部處的暴露受限和工作角度降低。這種局限性部分是由於與中線相比,上髓膜在外側與第四腦室底形成更窄的角度。此外,位於懸垂扁桃體空間吻端的懸垂錐體連接處限製了暴露。上髓膜和懸垂錐體連接處限製了導水管和沿第四腦室底部75%點的工作角度。兩種入路的工作角度的差異小於8英寸,在第四腦室底中點處,端瓣入路工作角度的適度減小消失了。在地板的中點,兩種方法的工作角度與引水渠的暴露相比增加了一倍多。
與橫臥入路相比,端瓣入路可使第四腦室底部暴露,並增加上外側隱窩和Luschka孔的暴露,而在接近腦室吻端四分之一時,工作角度僅略有下降。然而,這種暴露不需要切除或切開小腦功能區,可能與較低的緘默症發生率和其他術後神經後遺症有關。
貢獻者:Necmettin Tanriover, MD, Arthur J. Ulm, MD, Albert L. Rhoton, Jr, MD,和Alexandre Yasuda, MD
這篇文章最初發表於這裏:Tanriover N, Ulm AJ, Rhoton AL, Jr, Yasuda A.第四心室經橫裂和端velar入路的比較。J Neurosurg101:484 2004; 498年,doi.org/10.3171/jns.2004.101.3.0484,並通過與神經外科雜誌》及其母公司美國神經外科醫生協會(AANS)。AANS保留全部版權。本材料的出現並不意味著由任何其他方開放獲取或免費使用。
神經外科188bet手机app圖譜很榮幸能夠繼承Albert L. Rhoton, Jr . MD的遺產。
請登錄發表評論。
一定要在社交媒體上關注我們,獲取精彩內容並保持更新生活科恩醫生的會議,關於手術技術的問題,以及更多!



您必須登錄才能查看此材料。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
現在請捐!
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。請承諾每年至少捐贈250美元給Atlas。
如果沒有這個承諾,Atlas將很快需要付費訂閱世界上許多病人的護理都依賴於它的外科醫生將無法使用它。現在請捐!