

你可以有所作為。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
現在請捐!
最後更新:2021年4月9日
客觀的:描述通過六種入路對腦周池的暴露,重點是大腦後動脈及其分支的暴露。
方法12個半球的解剖暴露了腳池、周圍池和四頭池以及大腦後動脈的相關節段。使用隱形圖像引導工作站(Medtronic Surgical Navigation Technologies, Louisville, CO)比較兩種方法。
結果經sylvian入路暴露了踝間池和腳池。顳下入路暴露了踝間和腳池以及周圍池的下半部分。顳葉收縮和Labbé靜脈的位置限製了四叉神經池的暴露。枕部幕前和幕下小腦上入路暴露四周池和下三分之二的周圍池。經腎竇入路暴露了腳池的後三分之一、周圍池的上三分之二和近端四頭池。經脈絡膜入路暴露了10個半球中9個P2段(P2p)的後部分,是唯一暴露了脈絡膜後外側動脈和脈絡膜前動脈叢段的入路。枕部幕前和幕下小腦上入路均可進入P3段,暴露了10個半球中的4個半球的P2p段。顳下入路可進入脈絡膜前動脈和脈絡膜後動脈的池段和腳段,暴露出10個半球中的3個半球的點對點段。
結論:對周圍腦池病變的手術入路必須根據病理發現的部位進行調整。暴露最具挑戰性的區域是周圍池的上半部分,特別是大腦後動脈的P2p段。

接近周圍腦池內的病變對神經外科醫生提出了獨特的挑戰。這個區域的解剖結構很複雜,有許多動脈、穿孔血管、深靜脈引流通道和顱神經穿過它的邊界。該區域的病理結果是多樣化的,包括整個神經外科的光譜。腦周池位於大腦深處,部分被上麵的結構屏蔽,包括顳葉、海馬旁回、腦島門、腦幕切骨和Labbé靜脈。沒有一種單一的手術入路可以進入整個腦周池,但入路必須根據患者的病理發現的部位和類型進行定製,並對該區域的解剖學有全麵的了解。
周圍腦池的周圍部分和伴隨的大腦後動脈(PCA) P2段(P2p)的後部分是一個特別具有挑戰性的暴露區域。對於PCA的這部分,選擇合適的手術入路仍有爭議(14,16,25,35,44,51)。本研究的目的是定義周圍腦池的解剖段,描述該區域的六種入路的顯微解剖,比較使用一種新的圖像引導應用的入路,並概述該區域病灶的入路策略。
在這項研究中,來自6具注入彩色矽膠的屍體頭部的共12個半球進行了檢查。放大倍率×3到×40和顯微外科技術被用來比較6種手術入路對周圍腦池的影響。所研究的入路為經sylvian顳前、顳下、枕部幕下、幕下小腦上、經顳門經腦膜和經島葉經腦膜。通過每種方法暴露的PCA的節段和主要分支在10個半球被識別。在每一種方法中,都特別注意到限製可視化的解剖結構。
使用磁共振成像對三具屍體頭部進行研究,並使用標準協議在隱形圖像製導工作站(美敦力外科導航技術公司,路易斯維爾,CO)注冊。使用西門子Magnetom Allegra掃描儀(Siemens Medical Systems, Inc., Erlangen, Germany)獲得三特斯拉磁共振成像掃描,並轉移到Stealth工作站。掃描前,行雙側大眶顴額顳部、雙側枕部和枕下開顱術。基本上,三個骨橋在凸起處被完整保留下來,並附著在基準點上。骨橋位於上矢狀竇和頂枕皮質。注意保持硬腦膜完整。十個用於圖像配準的基準地標以統一的方式放置在骨橋上。剩餘的顱骨提供了一個穩定的平台,用於顯微解剖過程中定位和保持相對解剖位置。建立了三維模型,並將動態參考陣列固定在屍體上。將屍體與三維模型和圖像進行配準,並建立了在10厘米處優於2毫米的估計精度。 An active probe was then used to indicate the surgical exposure on the three-dimensional model and three orthogonal magnetic resonance imaging views. These images were recorded through screen captures. The limits of exposure through each of the approaches to the perimesencephalic cisterns were determined by image guidance under direct microscopic visualization. Measurements included the superior, inferior, anterior, and posterior limits of surgical exposure as well as the trajectory and working distance for each approach.
腦周池由圍繞中腦的充滿腦脊液的空間組成。我們把這個地區分成四個部分。第一部分是蹠間池,位於腦梗之間,並與鞍上池前部和上外側的椎間裂相通(3,24)。第二個部分是腳池,位於內側的腦梗、外側的鉤狀肌後段和上方的視神經束所包圍的空間內(3,24)。腳池向上與側裂相通,內側與踝間池相通,後方與周圍池相通。第三段是周圍池,從腳池的後緣延伸到中腦丘的外側緣(24)。所述環境池的壁如下:前,腦梗的後表麵;內側,中腦的外側表麵;外側有穹幕邊緣、海馬旁回、穹窿絲膜和脈膜裂;上方為丘腦枕部、外側膝狀體和視神經束(圖1)。在冠狀麵觀察時,周圍的腦池在海馬旁回周圍呈“C”形(圖1D)。 The final segment is the quadrigeminal cistern, which lies posterior to the colliculi, below the splenium, anterior to the apex of the cerebellum, and superior to the cerebellomesencephalic fissure (Fig. 1, A and D) (3, 22, 24).
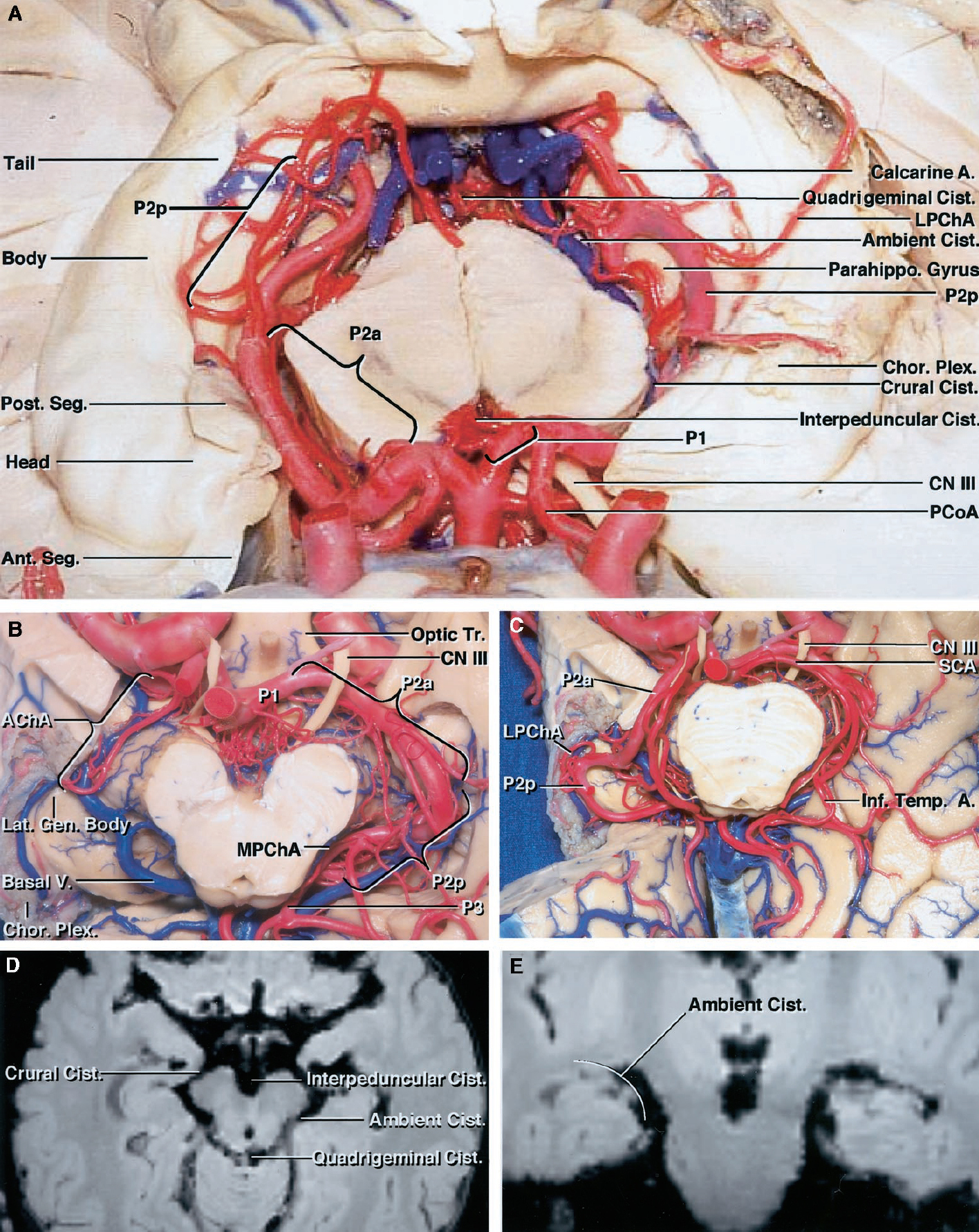
圖1。A,顯示周圍腦池上方的標本。周圍腦池包括環繞中腦的踝間池、腳池、周圍池和四頭池。腦梗間池位於腦梗之間。腳池位於鉤椎後段和腦踝之間。周圍池從腳池的後邊緣延伸到中腦丘的外側邊緣。海馬體的頭、體、尾和脈絡膜叢暴露在顳角的底部。注意,右側的點對點位於海馬旁回內側邊緣上方,而左側的點對點位於海馬旁回內側。B,標本顯示基底池下方。右邊的P2a和P2p已經被移除,以暴露腳和環境水箱的屋頂。 The lower part of the temporal lobe has been removed to expose the temporal horn and basal cisterns. The anterior choroidal artery enters the choroid plexus in the temporal horn. The lateral geniculate body and optic tract sit in the roof of the cisterns. The P1, P2, and P3 segments; inferior temporal branches; and medial posterior and lateral posterior choroidal arteries are exposed. C, specimen showing anterior inferior temporal lobe below the choroidal fissure removed to expose the relationship between the P2p and choroidal fissure. The choroidal fissure begins at the posterior edge of the posterior uncal segment at the site where the anterior choroidal artery enters the temporal horn to become the plexal portion. Note how the right P2 ascends and courses laterally to reach the upper surface of the medial edge of the parahippocampal gyrus in close proximity to the choroidal fissure. D, axial magnetic resonance imaging scan of a cadaver using the Stealth workstation demonstrating the segments of the perimesencephalic cisterns. E, coronal magnetic resonance imaging scan demonstrates the “C” shape of the ambient cistern. A., artery; AChA, anterior choroidal artery; Ant. Seg., anterior segment of uncus; Basal V., basal vein; Body, body of hippocampus; Chor. Plex., choroid plexus; Cist., cistern; CN III, oculomotor nerve; Head, head of hippocampus; Inf. Temp. A., inferior temporal artery; Lat. Gen. Body, lateral geniculate body; LPChA, lateral posterior choroidal artery; MPChA, medial posterior choroidal artery; Optic Tr., optic tract; Parahippo. Gyrus, parahippocampal gyrus; PCoA, posterior communicating artery; Post. Seg., posterior segment of uncus; SCA, superior cerebellar artery; Tail, tail of hippocampus. (Images courtesy of AL Rhoton, Jr.)
我們之前已經描述了PCA的解剖結構,並將其分為相關的部分(52)。簡單地說,P1段開始於基底動脈尖,結束於後交通動脈的插入處。P2節段分為前半部分(P2a)和P2p。P2a從後交通動脈與PCA的交界處延伸,止於腦梗後緣的腳池後緣。點起於腳池的後緣,止於中腦丘的外側緣。點通常在周圍池內向上方和橫向移動,位於海馬旁回的上表麵。P3段穿過四叉腦池,而P4段由沿著其路徑由PCA產生的皮層分支形成(圖1)。
脈絡膜動脈與周圍腦池密切相關。脈絡膜前動脈起於後交通動脈從頸內動脈後表麵出發的遠端數毫米處,沿著後臍段的前端和近端,通過下脈絡膜點進入側腦室(3,8,9,45)。脈絡膜後內側動脈最常起源於P1;然而,相當多的腫瘤發生在離P2較遠的地方。內側後絨毛膜動脈向PCA的下方和內側移動,經過腳和周圍池,並向內側轉彎進入四頭池(9,23,30,45)。然後動脈向前轉進入膜間質,供應第三腦室頂部的脈絡叢(9,30,45)。脈絡膜後外側動脈最常見的分支是一個或幾個分支,在周圍池內沿著海馬旁回的上邊緣向外側延伸,穿過脈絡膜裂進入顳角和心房的後部(圖1、A和C)(8,9,24,30)。
PCA在經過腳、周圍和四頭腦池的過程中產生皮層分支。從近端到遠端,這些分支包括顳下動脈、頂枕動脈、鈣質動脈和脾動脈(52)。顳下動脈包括一組血管,包括海馬、前顳、中顳和後顳支(圖1,a - c)(52)。
頭部置於標準手術體位,通過椎側暴露接近基底動脈(4,15,34,35,49)。側裂被廣泛地剖開並沿著整個長度打開。視神經和頸內動脈周圍的腦池也被切開。在暴露視神經和動眼神經和頸動脈之間的區域後,注意到暴露的周圍腦池。顳葉後外側向遠離額葉蓋的方向收縮,暴露基底尖和PCA的起源。此時,優化頭部定位和鏡角以暴露PCA在腦梗周圍的過程。顳葉後縮極限位於Meckel’s cave後緣(圖2,A-D)。

圖2。Pretemporal transsylvian方法。A,標本顯示右側眶顴骨開顱術,暴露了側裂、額葉和顳葉。這張插圖顯示了眶顴雙瓣開顱手術的位置。B,標本顯示側裂近端廣泛打開,露出M2分支和島表麵。C:打開的頸動脈光三角,位於視神經、頸動脈和大腦前動脈A1段之間,打開的頸動脈-動眼窩,位於動眼神經和頸動脈之間。注意腦島膜阻礙了進入腳池的視野。D,標本顯示顳葉向後收縮,M1近端抬高,暴露腳池前部的P2a。P1s, P2a,脈絡膜前動脈和PCA進入視野。E-G,隱身磁共振成像掃描顯示顳前入路獲得的暴露極限(箭頭)。 Anterior exposure through the approach is excellent and provides access to the interpeduncular cistern. The posterior and superior exposures are limited by the limen insula. The posterior limit of exposure is at the posterior edge of the cerebral peduncle, and the upper limit is on the upper third of the uncus. A1, A1 segment of the anterior communicating artery; AChA, anterior choroidal artery; CN II, optic nerve; CN III, oculomotor nerve; ICA, internal carotid artery; M1, M1 segment of middle cerebral artery; M2, M2 segment of the middle cerebral artery; PCoA, posterior communicating artery. (Images courtesy of AL Rhoton, Jr.)
在使用隱身圖像製導工作站研究的六個半球中,進行了多次測量和定位。特別地,確定了周圍腦池內暴露的前、後、上、下界限。顳前入路暴露了踝間和腳池,但沒有暴露周圍和四頭肌部分。暴露的主要解剖學局限性包括腦島、內側突出的頦骨尖和到達某些區域所需的後顳葉過度回縮(圖2,E-G)。
該入路提供了良好的中腦前方暴露,包括頸內動脈、大腦前動脈和大腦中動脈複合體。所有病例均暴露PCA原點及P1、P2a。此外,我們能夠暴露脈絡膜前動脈的起源和大部分池段。內側後脈絡膜動脈起源於P1或P2a的10個半球中的9個半球。在一個半球,內側後脈絡膜動脈起源於周圍池內的點,不能暴露。絨毛膜後側血管,最常見的起源於點,不能通過經椎體入路暴露。此外,P2p和P3通過這種方式是無法訪問的(表1)。

研究了三種不同的顳下手術入路:前、中、後延伸(5,7,10,11,20,27,35,39,43)。該方法包括將矢狀線與地麵平行放置,頂點向下傾斜,以便沿腦幕麵至腦周池的最大可見性。顴骨弓和顳骨的鱗狀和岩狀部分被鑽成一個沿著中窩底的平坦軌跡。將連接顳葉中段和腦幕邊緣的蛛網膜小梁切開並取出,以暴露其下方結構(圖3,A-C)。
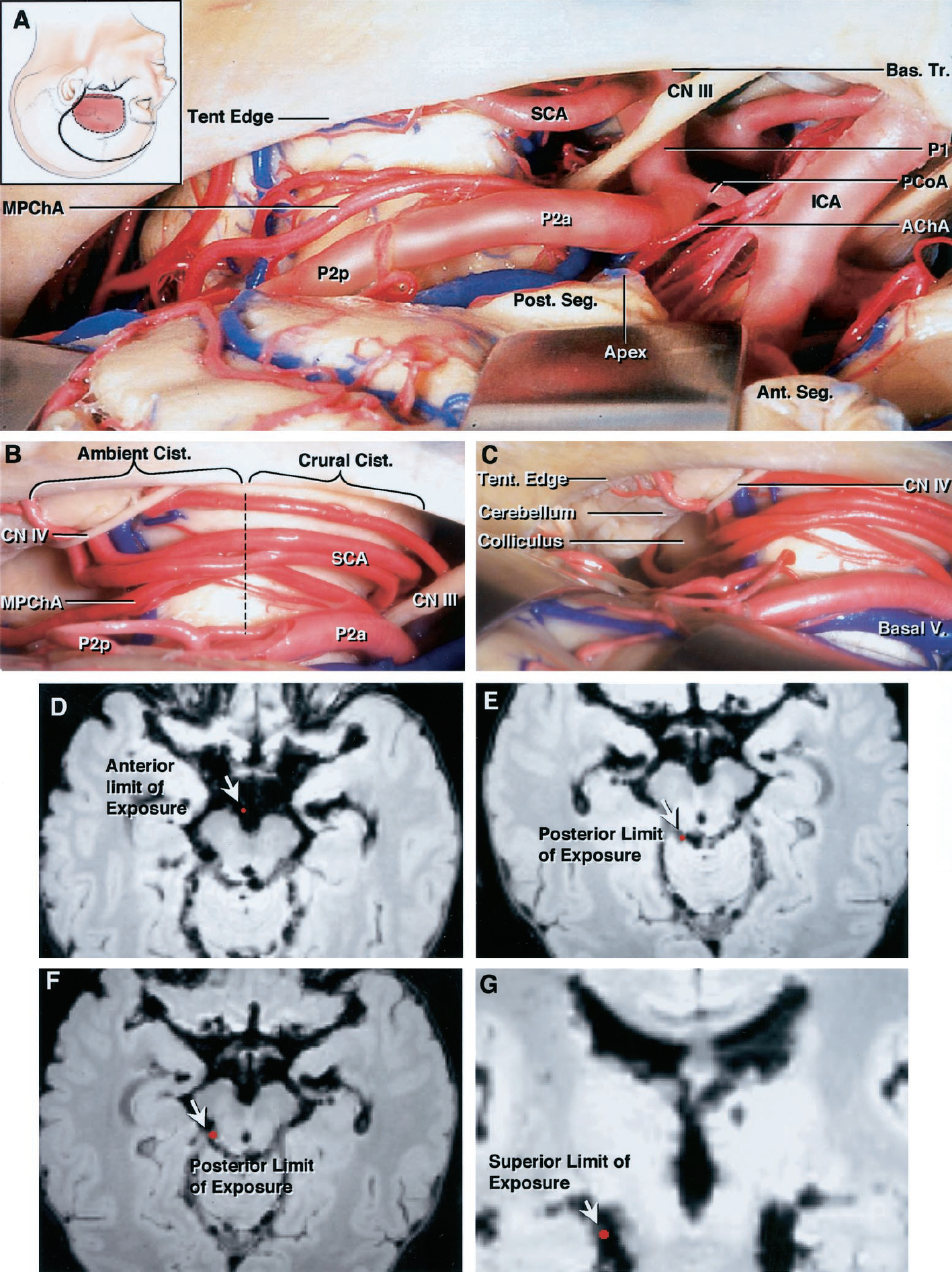
圖3。A-C,左顳下入路到腦周圍池。A,標本顯示前顳下入路暴露踝間和小腿下半部分及周圍池。暴露的結構包括頸內動脈、脈絡膜前動脈、後交通動脈、基底動脈、小腦上動脈和脈絡膜後動脈內側動脈、P1和P2a,以及前、後節段和鉤椎頂端。B,標本顯示顳下正中入路暴露腳池內的P2a,周圍池內的P2p,內側後脈膜動脈和小腦上動脈,滑車神經和幕邊緣。C,標本顯示後顳下暴露,可看到前四叉神經池,暴露丘板、滑車神經和基底靜脈。D-G,隱身磁共振成像掃描顯示的限製(箭頭)的方法。D,左側前顳下暴露提供了進入踝間池和穿過對側腦踝內側的通道。E,不受Labbé靜脈前麵位置限製的半腦暴露後界限是入路同側的四叉神經池的外側部分。F,與入路同側半腦暴露的後界限,其中Labbé靜脈的前位置限製了顳葉的收縮。 G, superior limit of exposure within the ambient cistern was limited to the lower one-half to two-thirds of the cistern because of the prominence of the medial edge of the parahippocampal gyrus. Reaching the upper part of the cistern would require excessive temporal lobe retraction. AChA, anterior choroidal artery; Ambient, ambient cistern; Ant. Seg., anterior segment of uncus; Apex, apex of uncus; Bas. Tr., basilar trunk; Basal V., basal vein of Rosenthal; CN III, oculomotor nerve; CN IV, trochlear nerve; Crural, crural cistern; ICA, internal carotid artery; SCA, superior cerebellar artery; Tent edge, tentorial edge; MPChA, medial posterior choroidal artery; PCoA, posterior communicating artery; Post. Seg., posterior segment of the uncus. (Images courtesy of AL Rhoton, Jr.)
在所有標本中,踝間、腳和周圍池的下半部分可以在顳下暴露(圖3,D-G)。在10個標本中有6個,後顳下通路可到達四叉神經池(圖3E)。在4個標本中,Labbé靜脈阻斷了周圍池後部的暴露(圖3F)。通過這種方法暴露的另一個解剖障礙是海馬旁回。周圍池的上1 / 3至1 / 2,延伸至海馬旁回的圓形內側邊緣之上,從顳下入路無法到達(圖3G)。
所有10例標本均暴露基底動脈尖、P1、P2a和內側後脈絡膜動脈。脈絡膜前動脈的起源和大部分池段也可以通過顳下入路暴露出來。點的近、下表麵在三個半球均可到達。在7個腦半球中,P2p在腦踝後邊緣向上方延伸,並在海馬旁回內側邊緣上方隱藏起來(圖3、A和B)。所有腦半球都無法到達絨毛膜後外側動脈和P3(表1)。
檢查了兩個後入路,一個在幕上,一個在幕下。所檢查的入路為枕部小腦幕前入路和小腦上小腦幕前入路(1、2、18、19、28、29、31、32、35、37、40、46、47、51、53)。研究發現,兩者對周圍腦池和內部結構的暴露幾乎相同。每個手術都有一個穿過幕幕的中位切口。最明顯的區別是小腦的收縮和枕極的收縮(圖4和圖5)。

圖4。右枕骨幕前入路。A,顯示後視圖的標本,其中插圖展示了暴露的路徑。在直竇附近劃分幕。暴露的部位包括P2a、P2p、P3、鬆果體、丘、小腦上動脈、基底靜脈和蓋倫靜脈、滑車神經和PCA的顳下支。B,標本顯示小腦上方的放大視圖進入周圍池。入路的方向是小腦蚓部尖端的外側。P2a上升到隱藏在周圍池上部的海馬旁回內側邊緣之上。P3在四水池中再次出現。C-G,顯示暴露極限(箭頭)的隱身磁共振成像掃描。 C, anterior limit of exposure is the back edge of the crural cistern. D and E, approach provides excellent exposure of the quadrigeminal cistern. F, working distance to the deepest point of exposure in the six hemispheres averaged 8 cm. G, trajectory of approach to the anterior limit of exposure. H, superior limit of exposure in ambient cistern. Basal V., basal vein; CN IV, trochlear nerve; Inf. Temp. A., inferior temporal artery; Parahippo. Gyrus, parahippocampal gyrus; Pineal, pineal gland; SCA, superior cerebellar artery; Sup. Col., superior colliculus; Tent., tentorium; V. of Galen, vein of Galen. (Images courtesy of AL Rhoton, Jr.)

圖5。幕下小腦上幕前入路。A,顯示小腦後視圖的標本。注意橋靜脈阻塞了四叉神經池的通路。B標本顯示四腦池幕下中線視圖。暴露的結構包括鬆果體、注入Galen靜脈的靜脈複合體、P3、小腦上動脈和脈絡膜後內側動脈。C,標本顯示左側中旁入路,幕部完整,顯露丘板、第四神經和小腦上動脈。P3暴露在穹幕邊緣的上方和內側。D,標本顯示的視野與幕分開暴露在周圍池的P2p和後腳池的P2a。遠端點在周圍池的前部上升,隱藏在海馬旁回的內側邊緣之上。 E–J, Stealth magnetic resonance imaging scans demonstrating the limits (arrows) of exposure. E, anterior limit of exposure is at the back edge of the crural cistern. F and G, approach provides excellent exposure of the quadrigeminal cistern. H, trajectory of approach to the anterior middle portion of the ambient cistern. I, working distance from the posterior cortical surface to the most anterior point of exposure averaged 7 to 8 cm. J, superior limit of the exposure extended into the upper one-third of the ambient cistern, similar to that obtained through the occipital transtentorial approach. Basal V., basal vein of Rosenthal; Cist., cistern; CN IV, trochlear nerve; Colliculi, superior and inferior colliculi; Inf. Temporal A., inferior temporal artery; Inf. Vermian Vein, inferior vermian vein; Int. Cerebral V., internal cerebral vein; MPChA, medial posterior choroidal artery; Parahippo. Gyr., parahippocampal gyrus; PICA, posterior inferior cerebellar artery; Pineal, pineal gland; Sup. Colliculus, superior colliculus; Tent. Edge, tentorium; Transv. Sinus, transverse sinus; V. of Galen, vein of Galen. (Images courtesy of AL Rhoton, Jr.)
枕部小腦幕前入路和小腦幕上入路都可以很好地暴露四頭池和周圍池,也可以到達小腦幕邊緣以下的病灶(圖4和圖5)。兩種入路都可以到達腳腦池的後部,通過小腦上走路暴露程度略有增加(圖4C和5E)。與更靠前的入路相比,進入前周圍池和後腳池時的工作距離明顯更大(圖4F和5I)。後入路從皮質表麵到前周圍池的平均工作距離約為8 cm,而前入路的工作距離在4 - 5 cm之間。
這些後側入路可以很好地暴露P3。通過這些方法P1是無法到達的,隻有P2a的後三分之一可以暴露。在四個半球中,可暴露點的下表麵。在兩個半球,P2p以兩個主幹的形式存在,一個是上級主幹,一個是下級主幹。在這些腦半球中,下幹可以被觸及,而上幹則隱藏在海馬旁回的內側邊緣之上。在其餘的四個半球中,點位於海馬旁回內側邊緣以上(圖4B和5D;表1)。
兩種方法對脈絡膜血管的通路相似。脈絡膜前動脈在任何半腦內都無法進入,因為它進入顳角,在腳後池暴露的前方。內側後脈絡膜動脈周圍部和四叉部可以被觸及,但P1的起始部不能被觸及。脈絡膜後外側動脈起源於點對點段的上表麵或外側表麵,隨後外側流向海馬旁回上方的顳角(表1)。
經顳角脈絡膜裂可進入腦周池(16,24,25,26,30,45)。脈絡膜裂是位於丘腦枕部和穹窿的絨毛膜之間的裂口,顳角的脈絡膜叢就是沿著這個裂口連接的。裂隙始於脈絡膜下點,脈絡膜前動脈在該處進入顳角,位於腳池的後側和後臍段的後緣,標誌著動脈叢部的開始。除了脈絡膜前動脈外,脈絡膜後外側動脈分支通過顳角和心房後部的裂隙進入心室係統(24,30,45)。我們檢查了通過脈絡膜裂的兩種入路,一種是通過下顳葉,另一種是通過腦島下限製溝(圖6-9)(12,16,25,26,36,42,45,50)。

圖6。Transtemporal transchoroidal方法。A,標本顯示右側顳下回開顱術。插圖顯示了頭皮切口和開顱的位置。B,標本顯示側腦室顳角通過顳下回2厘米的皮質切開術進入,暴露海馬頭、脈絡叢和脈絡裂。C,標本顯示脈絡膜裂隙在穹窿側打開,通過將脈絡膜叢與穹窿的絲膜分離,以保存穿過裂隙的丘腦側的引流靜脈和穿通動脈。注意膝狀體外側,前後脈絡膜動脈和基底靜脈。D,標本顯示位於顳角前尖海馬體和杏仁核之間的恥骨隱窩。脈絡膜前動脈在位於海馬頭後麵的脈絡膜下點進入顳角並支配脈絡膜叢。E,標本顯示放大的P2p,絨絡膜後外側動脈和基底靜脈在周圍池中移動。 F, specimen showing quadrigeminal cistern and P3 accessed through the posterior portion of the approach directed through the choroidal fissure. G, specimen showing retraction of the hippocampus exposing the inferior temporal artery originating from the P2p. H, specimen showing transamygdala extension of the transchoroidal approach. An incision has been carried forward through the amygdala to expose the structures within the crural and interpeduncular cisterns, including the P2a; amygdala; posterior communicating, internal carotid, anterior choroidal, and medial posterior choroidal arteries; and optic and oculomotor nerves. AChA, anterior choroidal artery; Basal V., basal vein; Cer. Ped., cerebral peduncle; Chor. Fiss., choroidal fissure; Chor. Plex., choroid plexus; CN II, optic nerve; CN III, oculomotor nerve; Hip. A., hippocampal artery; ICA, internal carotid artery; Inf. Temp. A., inferior temporal artery; Inf. Temp. Gyrus, inferior temporal gyrus; Lat. Gen. Body, lateral geniculate body; LPChA, lateral posterior choroidal artery; MPChA, medial posterior choroidal artery; Parahippo. Gyrus, parahippocampal gyrus; PCoA, posterior communicating artery; Pulvinar, pulvinar of thalamus; Quadrigeminal, quadrigeminal cistern; Sphenopar. Sinus, sphenoparietal sinus. (Images courtesy of AL Rhoton, Jr.)
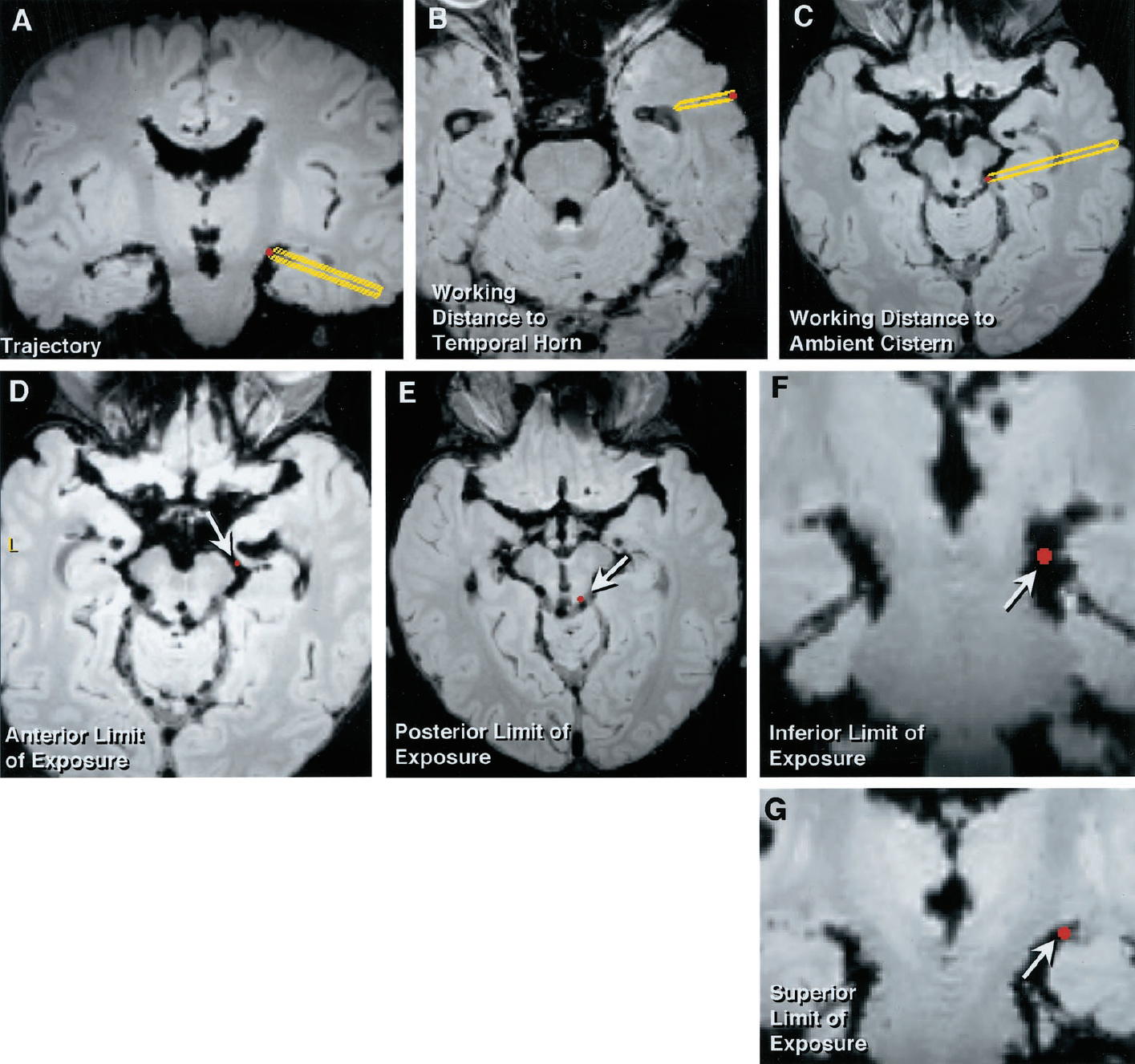
圖7。隱形磁共振成像掃描顯示通過經顳-經腎竇入路獲得的暴露。箭,暴露的極限。A,軌跡通過顳下回和顳角到達周圍腦池。B,外側皮層到顳角的距離平均為2 ~ 2.5 cm。C,從皮質切開術的後緣經過顳下回進入後周圍池。從皮質表麵到周圍池的距離約為4.0 ~ 4.5 cm。D,在脈絡膜下點暴露的右側前界限。E,四叉神經池近端暴露的左側後界限。F,環境池中暴露的下限。 Note the inability to access the lower ambient cistern. G, upper limit of exposure at the choroidal fissure. (Images courtesy of AL Rhoton, Jr.)

圖8。經島島經腦皮質入路至周圍腦池。A,標本顯示右側眶顴骨開顱術,沿側裂暴露額葉和顳葉。插圖顯示了頭皮切口和開顱的位置。B,側裂廣泛打開,暴露大腦中動脈M2段的島葉皮層和島葉分支。C,標本顯示放大視圖。腦島的下極限溝已經顯露出來。D,標本顯示皮層切口,穿過與M2分支平行的下限製溝前部,進入顳角,暴露脈脈絡叢和海馬頭部。顳角通常位於下極限溝約0.5厘米深。E,標本顯示脈絡膜裂隙打開,將脈絡膜叢的連接處與穹窿的絨毛膜分開,並將脈絡膜叢向丘腦縮回,暴露外側膝狀體、基底靜脈和點。 F, specimen showing P2p elevated to expose the depths of the ambient cistern and an inferior temporal branch of the P2p passing to the lower surface of the temporal lobe. Basal V., basal vein; Cent. Insular Sulcus, central insular sulcus; Chor. Plexus, choroid plexus; Fimbria, fimbria of fornix; Hippo., hippocampus; Inf. Limiting Sulcus, inferior limiting sulcus of insula; Inf. Temp. A., inferior temporal artery; Lat. Gen. Body, lateral geniculate body; LPChA, lateral posterior choroidal artery; M2, M2 segment of middle cerebral artery; Sylvian Fiss., sylvian fissure; Sylvian V., sylvian vein. (Images courtesy of AL Rhoton, Jr.)

圖9。經島島經類固醇入路的隱身磁共振成像掃描。A和B,通過椎間裂和下極限溝進入周圍池的軌跡。C,通過脈絡膜裂隙暴露到周圍池的上限值。D,腳池後端的脈絡膜下點暴露的前界限。E,暴露的後極限,在大多數半球,在後環境池。F,環境池下部的暴露下限。注意,如圖7所示,經島島入路的上至下軌跡比經顳盂經腎竇入路更能暴露周圍池的下側。箭,暴露的極限。(圖片由AL Rhoton, Jr.提供)
在研究的10個半球中,顳角位於顳葉前尖後方2.5 - 3.5 cm處,距顳中回表麵約2 - 2.5 cm處(圖7B)。經顳窩經腦膜入路包括在顳下回切除2cm的皮質,並打開顳角的外側壁(圖6、a和B)。進入顳角後,在絨毛膜和脈絡膜叢之間打開脈絡膜裂隙,以避免穿過裂隙的丘腦側的丘腦引流靜脈和穿通動脈(圖6C)。在這一點上,腳後池的上部和周圍池暴露出來。在大多數半球中,位於池頂的外側膝狀體和基靜脈是裂隙初始開放後最先遇到的結構(圖6C)。在海馬體下方的最小回縮情況下,周圍池的上半部分和PCA的相關節段可以暴露出來(圖6D)。更廣泛的回縮和剝離會使周圍池暴露更多,腳後池和前四頭肌池暴露更多(圖6,E-G)。經stemportransocoroid入路的主要缺點是需要在顳葉進行皮質切除術。有幾位作者報道了使用該入路治療周圍池病變的成功,發病率極低(16,25,26,36)。該方法的另一個局限性是Labbé的脈絡。在10個腦半球中的4個,Labbé靜脈向前延伸足夠遠,限製了顳葉皮層切口。
進入顳角脈絡膜裂的另一條途徑是通過腦島的下限製溝(50)。入路包括在下限製溝做一個2厘米的切口以進入顳角。切口通常位於大腦中動脈的島狀分支之間(圖8D)。顳角距島表麵約5mm。一旦進入顳角,絨毛膜裂被打開的方式與經stemportransocoroid入路相同(圖8,A-F)。在顳葉癲癇的杏仁體海馬切除術以及周圍腦池病變的切除中,經島島經腦池入路的一種變體已被廣泛使用和描述(50)。鑒於該入路在臨床實踐中的廣泛應用,人們預計沿下界限溝前部切口繼發的發病率最低(12,42,50)。
經脈絡膜入路可以很好地暴露脈絡膜後外側動脈,它通過脈絡膜裂進入顳角。此外,P2p在被檢查的10個半球中的9個經顱麵暴露。在一個半球,點位於海馬旁回的下表麵,不能經顱側暴露。兩種經腦竇入路都暴露了周圍池的上半部分、腳池的後三分之一和四頭池的鄰近部分(圖7和圖9)。鑒於入路的上到下軌跡,經島骨的變化允許更多的暴露周圍池的下部(圖7F和9F)。此外,我們還能夠通過這兩種變體進入P2a後段和P3前段。脈絡膜前動脈的叢部暴露於顳角內(表1)。
經脈絡膜裂入路的局限性包括不能到達脈絡膜內側後動脈、脈絡膜前動脈的起源段和池段、P1、P2a和P3的大部分。內側後脈絡膜動脈位於PCA下方周圍池的深處,並與多個腦幹穿支混雜在一起,使得通過這些入路識別困難(表1)。
腦池內及周圍的病變對神經外科醫生提出了獨特的挑戰。要想取得成功,需要對解剖學有全麵的了解,並了解用於進入該區域的方法的局限性。深的位置,狹窄的邊界,以及極其重要的血管結構的密度增加了挑戰。在本研究中,我們檢查了6種入路,試圖定義該區域的外科解剖,並描述各種入路的局限性(圖10)。

圖10。複合圖顯示通過六種入路對腦周圍池的暴露。軸向(左)和冠狀(右)圖像顯示。左圖顯示了經顳前(粉色)、枕部小腦幕前和小腦上小腦幕前(藍色)入路獲得的軸向曝光。右圖顯示了枕部小腦幕前入路和小腦上小腦幕前入路對周圍腦池的冠狀暴露。顳前入路暴露了踝間池和腳池,但沒有暴露周圍池或四頭池(左側,粉紅色)。枕部小腦幕前和小腦上小腦幕前入路暴露四頭池和周圍池,但不暴露腳和踝間池(左側,藍色)。枕部幕前和小腦上幕前入路可到達周圍腦池的下三分之二(右圖),而周圍腦池的上三分之一被海馬旁回的內側邊緣所掩蓋。B,左圖顯示經顳下入路軸向暴露的周圍腦池。顳下入路持續暴露踝間、腳和周圍池(橙色固體)。 Exposure of the posterior ambient and quadrigeminal cisterns is more variable and depends on the position of the vein of Labbé (orange hatched). The right image, in the coronal plane, demonstrates the extent of exposure of the ambient cistern through the subtemporal approach. The lower one-half of the ambient cistern was exposed subtemporally in all specimens (orange solid). The exposure of the upper one-half of the ambient cistern was blocked in the subtemporal approach by the medial edge of the parahippocampal gyrus and the position of the vein of Labbé. Excessive retraction would be required to expose the upper part of the ambient cistern. C, left image, transinsular and transtemporal transchoroidal approaches provided access to the ambient cistern in all hemispheres (green solid). Exposure of the quadrigeminal cistern was more variable and was limited by the position of the tail of the hippocampus (green hatched). In the right image, both the transinsular (upper green arrow) and transtemporal transchoroidal (lower green arrow) approaches exposed the upper one-half to two-thirds of the ambient cistern (solid green). The transinsular transchoroidal approach accessed the lower ambient cistern (green hatched). The added inferior exposure gained through the transinsular approach is a result of the superior-to-inferior trajectory through the inferior limiting sulcus of the insula (right image, upper green arrow). (Images courtesy of AL Rhoton, Jr.)
PCA是周圍腦池的主要血管結構。PCA的節段根據其所在的池命名,每個節段都需要獨特的手術入路(6,16,25,36,44,52)。基底動脈尖、p1 -後交通動脈和後交通動脈- p2a動脈瘤可通過經顱或前顳下入路進入(4 - 7,11,15,20,33 - 35,38,49)。枕部幕前和幕下小腦上入路被認為是治療P3段動脈瘤的最佳入路(36,44)。
P2動脈瘤,特別是P2p動脈瘤,曆來是最具挑戰性的病灶(16,25,36,44)。點在周圍池內運行,與海馬旁回密切相關。P2通常在周圍池內上升,通常位於海馬旁回的上表麵。周圍池在冠狀截麵上呈“C”形,因為它圍繞海馬旁回的圓形內側邊緣延伸。當點位於“C”的上部時,當從下麵通過顳下、枕部、幕下和小腦上入路接近時,腦回限製了這部分的暴露。在10個半腦中,隻有近端和下端可通過顳下通路進入。在其他7個半球,必須切除海馬旁回的一部分,以暴露下顳下點(14)。經枕部幕後和幕下小腦上入路,在10個半球中有4個半球成功暴露了點。在兩個半球中,點分為下幹和上幹,下幹可能暴露在海馬旁回下方,上幹隱藏在海馬旁回上方。在其餘的4個半球中,由於P2p位於海馬旁回的上表麵,因此無法通過枕部幕前和幕下小腦上入路到達。
經動脈入路可進入上部環境池。在10個半球中有9個是經顱側暴露的。其中一個半球的P2p位於周圍池的下半部分,不能經顱向暴露,因為海馬旁回的上半部分阻擋了P2p的進入。一些作者認為,血管造影顯示的P2段動脈瘤與脈絡膜下點的位置是選擇合適手術入路的關鍵標誌(16,44)。Ikeda等人(16)建議當PCA位於或高於下脈絡膜點水平時,對P2遠端動脈瘤使用經脈絡膜路徑。基於我們目前的研究,我們認為海馬旁回內圓邊緣的中點也提供了同樣重要的地標。從內側邊緣中點往上移動可改善經肩膜入路的暴露,但會惡化經顳下、枕部、幕前和小腦上入路的暴露。相反,從腦回中點往下移動可以改善經顳下、枕部和小腦上入路的暴露,但會惡化經腦膜入路的暴露(圖10)。
脈絡膜前動脈、內側後動脈和外側後動脈與周圍腦池密切相關(8,24,45)。需要特殊的手術方法來暴露這些動脈。脈絡膜前動脈起源於頸內動脈,位於PCA的遠端,在進入下脈絡膜點的顳角之前,穿過腳池的前三分之二。起源和腦池段隻能通過經sylvian顳前和前顳下通路接近。神經叢部分隻能經顱側進入。內側後脈絡膜動脈是三條脈絡膜動脈中最長的一條,任何單一入路都不能暴露全部血管段。該動脈典型地從P1發出,作為單一的主幹,在進入第三腦室後頂之前,穿過主腦室內側和下方的腳池、周圍池和四頭池。經側顳前入路可暴露血管的起源和小腿段。在研究的10個半球中,有一個半球的血管起源來自於下丘腦,不能通過經椎體通路到達。顳下入路暴露了研究的所有10個半球的內側後脈絡膜動脈的起源以及腳段、周圍段和近端四頭肌段。 Access to the distal quadrigeminal portion of the artery was limited because of the need for excessive temporal lobe retraction and/or the position of the vein of Labbé. Exposure of the medial posterior choroidal artery through the two transchoroidal approaches was difficult because of the fact that the artery has a relatively low-lying position within the cistern and visualization is obstructed by the overlying PCA and multiple brainstem perforators. The lateral posterior choroidal artery proved to be the most difficult artery to identify and expose. The artery typically arises as one or several branches off the distal P2 and courses directly lateral on the superior surface of the parahippocampal gyrus to enter the temporal horn. Only the transchoroidal approaches could reliably expose the artery.
當病灶累及P3或病灶延伸至四腦池相當長的距離時,應選擇枕部小腦幕前或幕下小腦上入路。其他的方法都沒有可靠地暴露這些結構。
所有檢查的方法在暴露周圍腦池內關鍵結構的能力上都有局限性。這些限製可能在術前影像學檢查中不容易表現出來,但可能在手術過程中變得明顯。這些方法可以在同一個開顱手術中結合使用,以擴大手術野。例如,將經sylvian顳前入路與經島島經甾體入路相結合,可以使外科醫生進入周圍池。此外,通過這種經腰椎聯合入路,外科醫生可以到達脈絡膜前動脈和脈絡膜後外側動脈的起源、池和叢部分,以及P1、P2a和P2p。當處理複雜的動靜脈畸形或接受多個脈絡膜動脈血液供應的腫瘤時,聯合暴露可能是至關重要的(13,14,17,21,41,42,48)。
另一種聯合入路在手術中提供了更大的暴露和靈活性,是顳下入路和經stemportransocoroid入路的組合。顳下入路在暴露上周圍池、頸動脈、脈絡膜後外側動脈和脈絡膜前動脈叢部分的能力方麵受到限製。然而,該入路可以很好地暴露出踝間池、P1、P2a、周圍下池、內側後脈絡膜動脈和前脈絡膜動脈的起源。在顳下入路過程中,通過打開顳葉和顳角的下部,增加經顱鏡暴露的能力,可以極大地促進處理複雜的動靜脈畸形、腫瘤和點狀動脈瘤的能力。
在手術過程中可擴展經顳部經腦膜入路,以提供進入前腦的通路。與顳葉切除術一樣,通過杏仁核切開,可進入頸內動脈、P1、P2a、PCA、脈絡膜前動脈、脈絡膜後內側動脈以及腳和踝間池(圖6H)。通過杏仁核的延伸可用於處理暴露病理結果時意想不到的困難,或在處理動脈瘤時提供近端控製。
在計劃對周圍腦池的手術入路時,外科醫生必須預測暴露所需要的關鍵結構。有了這種認識,就可以選擇適當的方法或方法的組合。在手術過程中,可以增加經椎體經顳前和顳下入路的經頸動脈延伸,以擴大這些標準入路的暴露範圍。
接近周圍腦池內的病變對神經外科醫生提出了獨特的挑戰。這個區域的解剖結構很複雜,有許多動脈、穿孔血管、深靜脈引流通道和顱神經穿過它的邊界。腦周池位於大腦深處,部分被上麵的結構屏蔽,包括顳葉、海馬旁回、腦島門、腦幕切骨和Labbé靜脈。沒有一種單一的手術入路可以進入整個腦周池,但入路必須根據特定患者的病理結果,並對該區域的解剖學有全麵的了解。我們提出了該區域六種入路的顯微外科解剖,特別注意PCA及其主要分支的暴露。利用一種新的圖像製導方法對上述方法進行了比較。
貢獻者:Arthur J. Ulm,醫學博士,Necmettin Tanriover,醫學博士,Masatou Kawashima,醫學博士,Alvaro Campero,醫學博士,Frank J. Bova博士,和Albert L. Rhoton, Jr醫學博士
Ulm AJ, Tanriover N, Kawashima M, Campero A, Bova FJ, Rhoton AL, Jr.的內容。采用顯微外科手術入路切開腦周池和大腦後動脈相關節段:使用一種新的圖像引導應用進行比較。神經外科2004; 54:1313 - 1327。doi.org/10.1227/01.NEU.0000126129.68707.E7.經牛津大學出版社代表神經外科醫師協會批準。©神經外科醫生協會。
神經外科188bet手机app圖譜很榮幸能夠繼承Albert L. Rhoton, Jr . MD的遺產。
請登錄發表評論。
一定要在社交媒體上關注我們,獲取精彩內容並保持更新生活科恩醫生的會議,關於手術技術的問題,以及更多!



您必須登錄才能查看此材料。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
現在請捐!
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。請承諾每年至少捐贈250美元給Atlas。
如果沒有這個承諾,Atlas將很快需要付費訂閱世界上許多病人的護理都依賴於它的外科醫生將無法使用它。現在請捐!