海綿狀畸形(CMS)是腦部和脊髓血管的良好良好的血管異常。幾個術語已用於海綿狀畸形,包括cavernous hemangiomas,cavernous angiomas, 和cavernomas。
CMs, along with capillary telangiectasias, arteriovenous malformations, anddevelopmental venous anomalies(DVA),組成四類腦血管畸形。CMS組成5%至13%的中樞神經係統(CNS)血管畸形,占人口的0.02%至0.5%。
These dilated capillary vessels have an increased risk of focal hemorrhage, leading to seizures and focal neurologic deficits. The locations of CNS CMs occur proportionally to the CNS tissue volume, with 80% in the supratentorial space, 15% in the posterior fossa, and 5% in the spinal cord.
CMs autoso零星或家庭mal dominant mode of inheritance. Magnetic resonance imaging (MRI) has revolutionized their diagnosis with no need for a tissue sampling, and has also allowed a better understanding of their natural history.
The clinical manifestations, natural history, and radiographic diagnosis and classification of cavernous malformations are discussed in the following section.
ADVERTISEMENT
Atlas選擇Microsurgery Procedural Pattie Collection
Designed for your every maneuver in surgery
Unparalleled flexibility and non-stick features
每個盒子都有每個案例的所有必要餅
LEARN MORE AND SHOP ONLINE

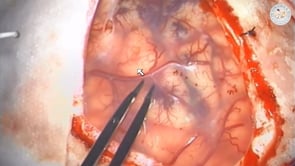
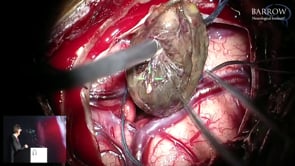
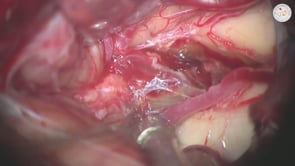
Figure 1: A typical appearance of a CM is illustrated. The abnormality has dilated sinusoids with no large feeder arteries or draining veins. These sinusoids are in various stages of bleeding, thrombosis and organization. There is no intervening neural tissue. Their lack of intervening neural tissue and prominent feeding or draining vessels pathologically distinguishes CMs fromdevelopmental venous anomalies, capillary telangiectasias, and micro-arteriovenous malformations.
Clinical Manifestations
Patients with CMs typically present with seizures, focal neurological deficits, and occasionally with acute intracerebral or intraventricular hemorrhage.Up to 20% of patients present incidentally, without symptoms related to the CM, while undergoing diagnostic tests for headaches. The presenting symptoms obviously depend on the location/size of the malformation and associated hemorrhage.
Supratentorial CMs most commonly present with seizures. In asymptomatic patients, the rate of new onset seizures has been estimated around 1.5% to 2.4% per patient-year. The development of seizures is most likely due to the deposition of iron, a known epileptogenic material found in hemosiderin and associated with recurrent episodes of hemorrhage. Focal deficits are far less common with supratentorial as compared with infratentorial lesions.
患有局灶性神經係統缺陷的患者更有可能涉及腦幹和基礎神經節的厘米。這些地區的小型出血可能因其臨近臨時上升/下降束和深核而引起急性缺陷。隨著出血吸收的症狀傾向於分解。Repeat hemorrhages may be associated with more severe neurologic deficits and an increased risk of a permanent deficit.
自然曆史
The natural history of CMs has been extensively studied, but a clear understanding of the risk of seizures and recurrent hemorrhage remains to be elucidated. The natural history is most likely similar for the familial and spontaneous forms.
Familial cavernous malformations are inherited in an autosomal dominant fashion, and there is a strong family history of seizures and presentation with multiple CMs in 80% to 90% of patients. The clinical penetrance is extremely variable with up to half of patients presenting asymptomatically. In one study by Zabramski and colleagues, six families with a familial form of CMs were followed. The symptomatic hemorrhage rates were 1.1% per lesion-year and 6.5% per patient-year. The average number of lesions shown on MRI was 6.5 lesions per patient. Del Curling and colleagues showed that the spontaneous form was associated with 1.34% risk of seizures per person-year in 26 patients who presented with a single malformation.
Asymptomatic patients have a much lower hemorrhage rate when compared with those with previous symptomatic hemorrhage. Kondziolka and colleagues showed a 0.6% hemorrhage rate among asymptomatic patients, compared with 4.5% in those with a history of symptomatic hemorrhage.
Hemorrhages that violate the lesion’s capsule indicate an increased risk for recurrent symptomatic hemorrhage. These hemorrhages are referred to asovert extra-lesional hemorrhages並且與初始事件更接近初始事件的特別高的重複出血率。
巴克和同事報告了在前28個月期間每年25.2%的恢複率和28個月後每年9.6%。Higher hemorrhage rates have also been reported after incomplete resection of the malformation.Therefore, complete resection of the CM is necessary to provide the patient with a substantial benefit.
Spinal cavernous malformations are rare, and therefore available data on their natural history is limited. Hemorrhage rates are most likely similar for spinal and other CNS CMs. Patients with symptomatic hemorrhage tend to clinically progress; resection within 3 months is advised because of high rehemorrhage rates.
Diagnosis
For diagnosis, MRI is the preferred imaging method for CMs. Before the advent of MRI, diagnosis of CMs was made using computed tomography (CT) and some small CMs were easily overlooked.
The typical CT findings are a well-circumscribed heterogeneously hyperdense mass with variable calcification and little to no enhancement. Based on these imaging characteristics, the differential diagnosis includes other vascular malformations, a hematoma, and a calcified or hemorrhagic neoplasm. Angiography may be used if there are concerns for abnormal vascularity, particularly given that CMs are often associated with DVAs.
CMs are typically avascular with no detectable feeding arteries or draining veins on imaging. Despite the use of MRI and magnetic resonance angiography (MRA), catheter angiography may be occasionally necessary to differentiate extra-axial CMs from other malformations or extra-axial tumors such as meningiomas. Parasellar CMs have minimal or rare feeding arteries, whereas parasellar meningiomas have hypervascularity and even rarely arteriovenous shunting. Single-photon emission computed tomography (SPECT) imaging may also be useful because CMs have low uptake, whereas meningiomas demonstrate high uptake. Sylvian and insular CMs may mimic a partially thrombosed MCA aneurysm on MR imaging.
On MRI, the appearance of CMs is often quite unique. Dilated sinusoids lack large feeding arteries or draining veins and are in various stages of thrombosis and organization from bleeding. These changes have been referred to as a “popcorn” or “berry” appearance and tend to be most striking on the T2-weighted sequence. There is no intervening neural tissue within the CM.
The hemosiderin, which demonstrates prominent low signal intensity blooming on gradient echo (GRE), susceptibility weighted imaging (SWI) and even T2-weighted sequences, is most prominent in the rim of CMs, but is also often present within septae throughout the lesions.
Many lesions can mimic the appearance of CMs and must be ruled out. These lesions include thrombosed arteriovenous malformations, thrombosed aneurysms, calcified low-grade gliomas, and hemorrhagic neoplasms.Metastatic diseaseis an important consideration in the setting of multiple CMs but can usually be excluded based on the lack of surrounding edema seen with most quiescent CMs. Follow-up imaging after the hemorrhage has resolved is important to identify the underlying lesion, often not apparent on the initial scans.

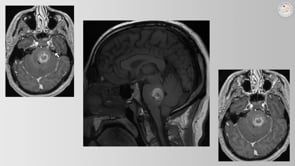
圖2:CMS的典型成像特性已被稱為“爆米花”或“漿果”外觀(左上圖像)。更突出的骨折出血灶通常存在於症狀病變(中間排)中。左側凸起厘米(左下圖像)的前後左側ICA血管儀揭示了“隱匿”畸形;然而,發育靜脈異常是明顯的(右下圖像箭頭)並且暗示診斷。請注意,CMS可以模擬膠質瘤(中左圖像)或部分血栓形成動脈瘤(左下圖像)。注意除左上圖像之外的所有上述MR圖像中具有明顯突出的出血的證據。
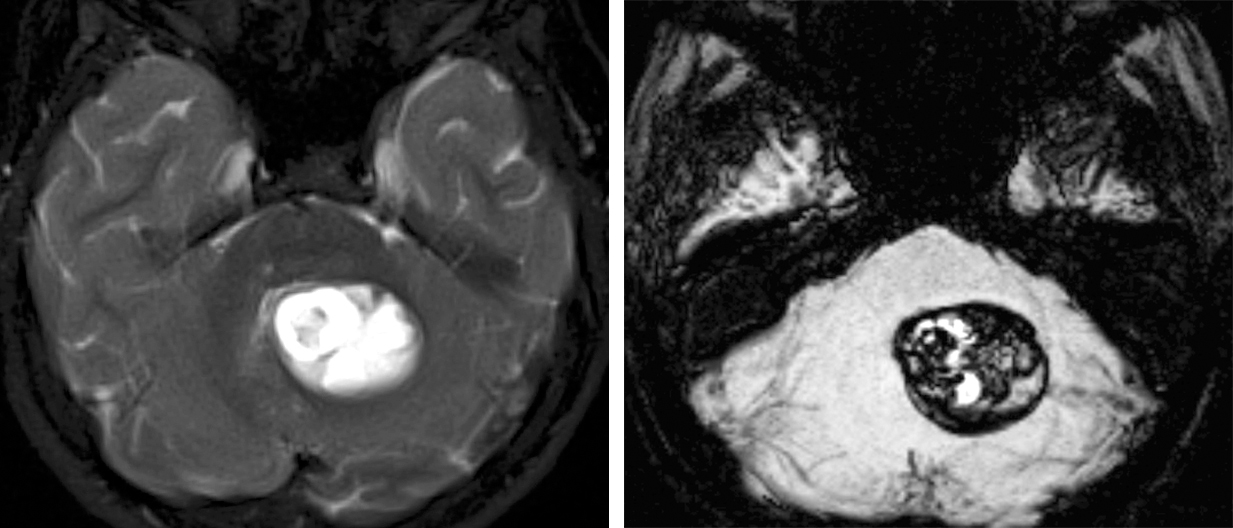
Figure 3: Susceptibility weighted imaging (SWI) and gradient echo (GRE) sequences often play an important role in the diagnosis of CMs. In the T2-weighted left image, a cerebellar cyst was suspected, but upon the review of the minimum intensity projection (mIP) reformats of the SWI sequence, the appearance of the hypointense lesion is most consistent with a CM.
在患有家族或多種CMS的患者中,GRE或SWI序列有利於鑒定常規脈衝序列忽略的病變的數量。
Classification
The most commonly used classification system divides CMs into four subcategories based on their pathologic correlation and CT/MRI appearance. This system was described by Zabramski and colleagues in 1994 by means of their prospective study of 128 CMs. Type I lesions are homogeneously hyperintense on T1WI and predominately contain subacute hemorrhage. With more chronic hemorrhage, a hypointense rim on T2WI develops as a result of hemosiderin-laden macrophages and iron deposition associated with hemoglobin breakdown.
Type II lesions are more multinodular, heterogeneous lesions typically referred to as having a “popcorn” core. This heterogeneous pattern on T1WI and T2WI occurs as a result of hemorrhage in various stages of breakdown septated by fibrocollagenous tissue and calcifications. Similar to type I lesions, type II lesions harbor a hypointense rim on T2WI.
Type III lesions appear as chronic hemorrhagic masses and therefore are isointense to hypointense on T1WI and hypointense on T2WI.
Type IV lesions are punctate hypointense lesions on GRE images.
Zambraski和他的同事們指出,病人with hyperintense lesions (evidence of acute or subacute hemorrhage: type I or II lesions) had a much higher chance of being symptomatic as compared to those with hypointense lesions (evidence of chronic hemorrhage: type III or IV lesions). In addition, hyperintense lesions also demonstrated a tendency for recurrent symptomatic hemorrhages. Although this classification has some prognostic worth,大部分病變症狀present with evidence of recent hemorrhage based on MR signal intensity and surrounding edema, which correlates with a higher risk of future hemorrhage.
DOI:https://doi.org/10.18791/nsatlas.v3.ch04.1
References
Badhiwala JH, Farrokhyar F, Alhazzani W, et al. Surgical outcomes and natural history of intramedullary spinal cord cavernous malformations: A single-center series and meta-analysis of individual patient data.J Neurosurg Spine。2014;21:662-676.
Barker FG, Amin-Hanjani S, Butler WE, et al. Temporal clustering of hemorrhages from untreated cavernous malformations of the central nervous system.Neurosurgery。2001;49:15-24.
Del Curling O Jr, Kelly DL Jr, Elster AD, Craven TE. An analysis of the natural history of cavernous angiomas.J Neurosurg。1991:75:702-708.
Kondziolka D, Lunsford LD, Kestle JR. The natural history of cerebral cavernous malformations.J Neurosurg。1995年; 83:820-824。
Labauge P,Brunereau L,Laberge S,Houtteville JP。33例無症狀患者的前瞻性隨訪,具有家族性腦海綿狀畸形的無症狀患者。Neurology。2001;57:1825-1828.
Labauge P, Brunereau L, Levy C, Leberge S, Houtteville JP. The natural history of familial cerebral cavernomas: a retrospective MRI study of 40 patients.Neuroradiology。200; 42:327-332。
McCormick WF. Pathology of vascular malformations of the brain, in: Wilson CB, Stein BM, (eds):Intracranial Arteriovenous Malformations。Baltimore: Williams & Wilkins; 1984:44-63.
Moriairty JL, Clatterbuck RE, Rigamonti D. The natural history of cavernous malformations.Neurosurg Clin N Am。1999:10:411-417。
Moriarity JL, Wetzel M, Clatterbuck RE, et al. The natural history of cavernous malformations: A prospective study of 68 patients.Neurosurgery。1999;44:1166-1173.
Otten P, Pizzolato GP, Rilliet B, Berney J. [131 cases of cavernous angioma (cavernomas) of the CNS, discovered by retrospective analysis of 24,535 autopsies]Neurochirugie。1989;35:128-131.
Robinson JR, Awad IA, Little JR. Natural history of the cavernous angioma.J Neurosurg。1991;75:709-714
Simard JM, Garcia-Bengochea, Ballinger WE, et al. Cavernous angioma: A review of 126 collected and 12 new clinical cases.Neurosurgery。1986;18:162-172.
Wakai S, Ueda Y, Inoh S, Nagai M. Angiographically occult angiomas: A report of thirteen cases with analysis of the cases documented in the literature.Neurosurgery。1985;17:549-556.
Zabramski JM, Feiz-Erfan I. (2011) Natural History of Cavernous Malformations. In HR Winn (Eds),Youmans Neurological Surgery。Saunders, Philadelphia, PA.
Zabramski JM, Wascher TM, Spetzler RF, et al. The natural history of familial cavernous malformations: results of an ongoing study.J Neurosurg。1994;80:422-432.
Available Through the Atlas
Unavailable Through the Atlas
Pleaselogin發表評論。