










你可以有所作為。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
現在請捐!
最後更新:2021年4月9日
1979年,作者介紹了三條與囊狀動脈瘤解剖相關的規則,在規劃這些病變的手術入路時應考慮這些規則(18)。這三個解剖方麵在本章中回顧與每個常見動脈瘤部位的關係。首先,這些動脈瘤發生在母動脈的分支部位。該部位可能是由母動脈的側支起源形成的,如頸內動脈的後交通動脈的起源,或由主動脈幹細分成兩條主幹形成的,如發生在大腦中動脈或基底動脈的分叉處(圖3.1和3.2)。其次,囊狀動脈瘤發生在動脈的轉彎處。這些曲線通過產生血管內血流動力學的局部改變,對接受脈衝波最大力的頂端區域施加不尋常的應力。囊狀動脈瘤長在曲線的凸側,而不是凹側。第三,囊狀動脈瘤所指向的方向,是在動脈瘤處沒有曲線時血液應該流向的方向。動脈瘤穹窿或動脈瘤底指向母動脈動脈瘤前段最大血流動力推力的方向。自從最初提出這三條規則以來,我們的解剖研究揭示了第四個規則。 The fourth rule is that there is a constantly occurring set of perforating arteries situated at each aneurysm site that need to be protected and preserved to achieve an optimal result (12, 13, 18).
動脈瘤很少發生在顱內動脈筆直的無分支段。長在直的無分枝節段的動脈瘤通常有囊,囊沿動脈壁沿血流方向縱向指向動脈壁,且僅在外膜表麵以上輕微突出。具有這些特征的動脈瘤屬於解剖型,而不是先天性囊狀動脈瘤,其發展的先兆往往是缺血性神經功能缺損,而不是與先天性囊狀動脈瘤相關的蛛網膜下腔出血。在動脈曲線的凹側或指向與母動脈血流方向相反的動脈瘤是很少見的。

這四個解剖方麵,因為它們適用於內頸動脈的脊狀肌上部分動脈瘤部位,首先考慮(圖3.1-3.4)。如果將頸內動脈(C4)的脊狀肌上部分的所有部位都包括在內,它是顱內動脈瘤最常見的部位,約占顱內動脈瘤的35%(8)。這些動脈瘤發生於5個部位:眼動脈起源處的頸內動脈上表麵,垂體上動脈起源處的內側壁,後交通動脈起源處的後側壁,前脈絡膜動脈起源處的後側壁,頸動脈尖部分叉進入大腦前動脈和大腦中動脈。
頸動脈脊上肌硬膜內顯露沿蝶脊或眶頂至前床突,從近端至遠端(圖3.3和3.4)。頸內動脈和視神經都在前床突的內側。該動脈出於前床突內側的海綿竇,位於視神經下方並略外側。它經過後、上、略外側,到達視交叉的外側,在那裏向前轉完成頸動脈虹吸s形曲線的上半部分。它在前穿孔物質下麵的區域分叉,形成大腦前動脈和大腦中動脈。
根據眼動脈、後交通動脈和前脈絡膜動脈的起源地,頸內動脈的脊上部分分為三段(圖2.4和3.5)。眼段從海綿竇頂眼動脈起點延伸至後交通動脈起點;的
交通段從交通後動脈起點延伸至脈絡膜前動脈起點;脈絡膜段從脈絡膜前動脈的起點延伸到頸內動脈的末梢分支。眼段最長,交通段最短。每根頸內動脈都有3到16個(平均8.2個)穿孔支,它們的起止點都相對恒定(3)。下麵回顧一下穿孔支與每個常見動脈瘤部位的關係。

點擊這裏查看此圖像的交互模塊和相關內容。
圖3.1。囊狀動脈瘤最常見的部位。每個動脈瘤都起源於大動脈的分支部位。大多數都位於威利斯環島或附近。超過90%位於以下五個部位之一:(a)位於後交通動脈水平的頸內動脈;(b)腦前動脈與前交通動脈的交界處;(c)大腦中動脈近端分叉;(d)大腦後動脈和基底動脈的連接處,(e)頸動脈與大腦前動脈和大腦中動脈的分叉處。頸動脈上的其他動脈瘤部位位於眼動脈、垂體上動脈和脈絡膜前動脈的起源處。椎動脈和基底動脈上的其他部位包括小腦前下動脈、小腦後下動脈、小腦上動脈以及基底動脈和椎動脈的交界處的起源部位。 A.C.A., anterior cerebral artery; A.Ch.A., anterior choroidal artery; A.Co.A., anterior communicating artery; A.I.C.A., anteroinferior cerebellar artery; B.A., basilar artery; C.A., internal carotid artery; M.C.A., middle cerebral artery; Op.A., ophthalmic artery; P.C.A., posterior cerebral artery; P.Co.A., posterior communicating artery; P.I.C.A., posteroinferior cerebellar artery; S.C.A., superior cerebellar artery; S.Hypo. A., superior hypophyseal artery; V.A., vertebral artery.

點擊這裏查看此圖像的交互模塊和相關內容。
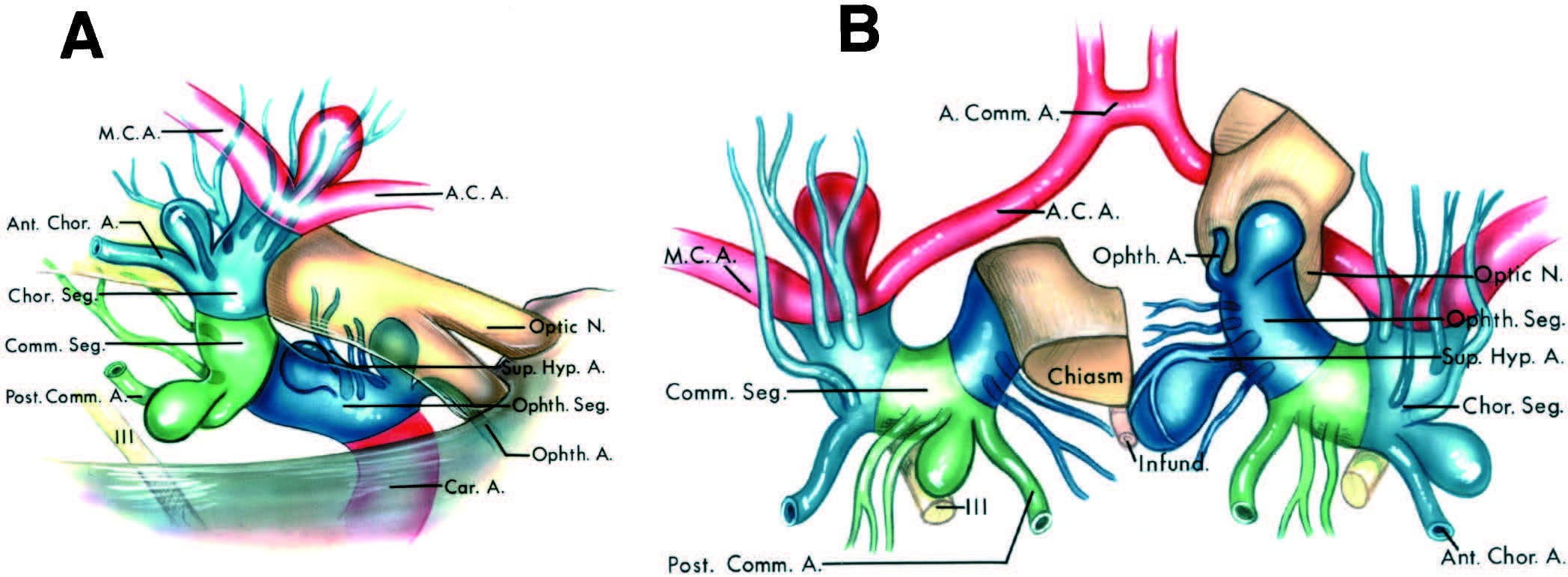
圖3.2。頸內動脈脊上部分常見動脈瘤部位的側位(A)和上位(B)視圖。A,右側頸內動脈的側位圖。B,頸內動脈上視圖,右視神經和右半視交叉向前反射,暴露眼動脈的起源。虛線顯示兩側頸動脈海綿狀內段和左眼動脈段。動脈瘤發生在動脈分支起源部位的彎曲處。動脈瘤所指向的方向(箭頭)是緊貼動脈瘤部位的最大血流動力的方向,也是在動脈瘤部位沒有曲線時血液應該流向的方向。內頸動脈上的動脈瘤部位通常位於頸動脈分支起源的遠端。起源於眼動脈起點的動脈瘤向上指向視神經。動脈瘤起源於垂體上動脈起源點視神經交叉內側下方。 Aneurysms arising near the origin of the posterior communicating artery point posteriorly toward the oculomotor nerve and are usually located superolateral to the posterior communicating artery. Aneurysms arising near the origin of the anterior choroidal artery point posterolaterally and are usually located immediately superior to the origin of the anterior choroidal artery. Aneurysms arising at the carotid bifurcation into the anterior and middle cerebral arteries point upward lateral to the optic chiasm toward the anterior perforated substance. A.C.A., anterior cerebral artery; A.Ch.A., anterior choroidal artery; C.A., internal carotid artery; M.C.A., middle cerebral artery; O.Ch., optic chiasm; O.N., optic nerve; Op.A., ophthalmic artery; P.Co.A., posterior communicating artery; S.Hypo.A., superior hypophyseal artery.
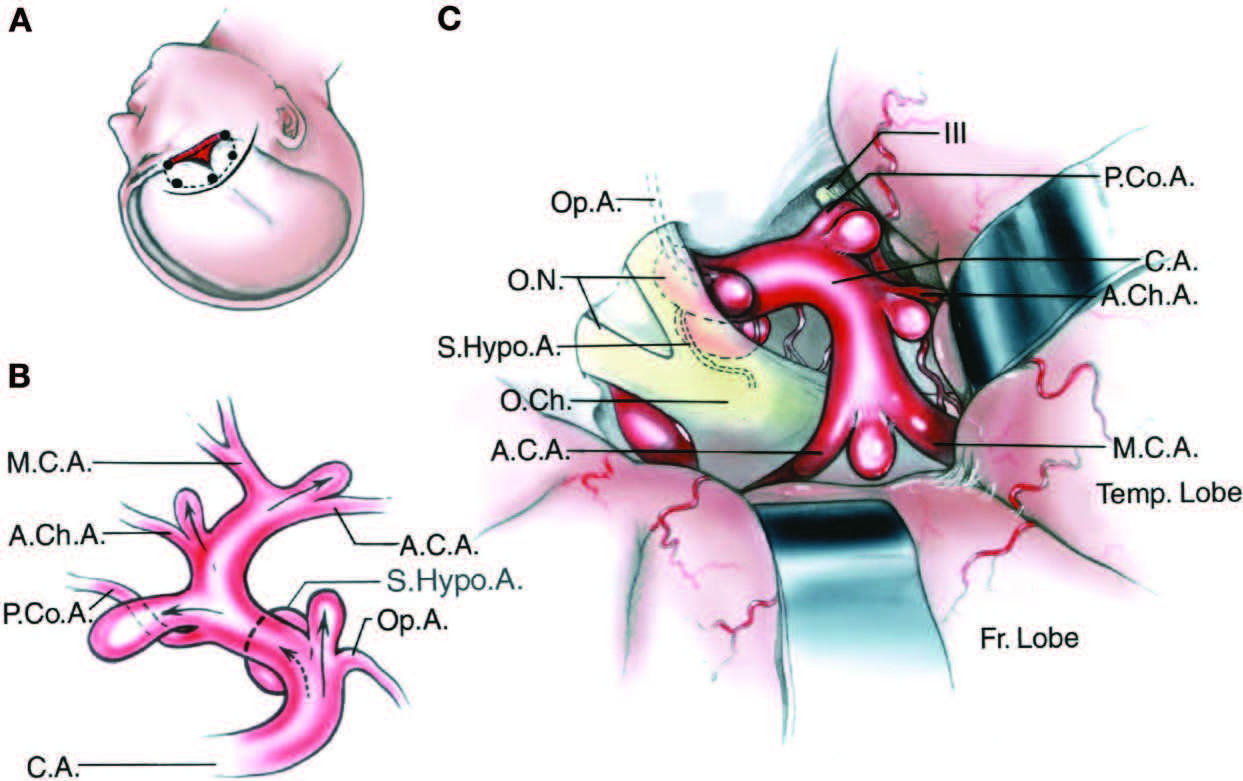
圖3.3。頸內動脈動脈瘤部位的手術視圖。A,頭皮切口(實線),骨瓣(虛線)和顱骨切除術(紅色區域),用於接近頸內動脈瘤。B,右側頸內動脈側位圖,顯示動脈瘤部位。C,右側額顳部開顱術所提供的手術視圖,腦鏟位於額顳葉。這些動脈瘤所指向的方向(B中的箭頭)是動脈瘤部位附近最大血流動力的方向,也是如果動脈瘤部位上的母動脈沒有彎曲時血液應該流向的方向。內頸動脈上的動脈瘤部位位於其分支起源的遠端。起源於眼動脈起點的動脈瘤向上指向視神經。動脈瘤起源於垂體上動脈起源點視神經交叉內側下方。動脈瘤發生於後交通動脈起點附近,指向動眼神經後方,通常位於後交通動脈上外側。 Aneurysms arising near the origin of the anterior choroidal artery point posterolaterally and are usually located immediately superior to the origin of the anterior choroidal artery. Aneurysms arising at the carotid bifurcation into the anterior and middle cerebral arteries point upward lateral to the optic chiasm toward the anterior perforated substance. Each of the aneurysms can be approached through a frontotemporal craniotomy. A.C.A., anterior cerebral artery; A.Ch.A., anterior choroidal artery; C.A., internal carotid artery; Fr., frontal; M.C.A., middle cerebral artery; O.Ch., optic chiasm; O.N., optic nerve; Op.A., ophthalmic artery; P.Co.A., posterior communicating artery; S.Hypo.A., superior hypophyseal artery; Temp., temporal.

點擊這裏查看此圖像的交互模塊和相關內容。
圖3.4。f。額顳(翼點)開顱術用於顯露威利斯圓上的動脈瘤。第一,頭皮切口的前端位於發際線後的中線附近。後端位於顴弓靠近耳屏處。B,頭皮皮瓣已經通過蓋膜下剝離術向下反射。麵部神經分支在其中的脂肪墊,暴露在照片的下緣。C,穿過覆蓋顳肌下部的顳淺筋膜的切口,使顳淺筋膜連同包裹麵神經分支的脂肪墊,隨頭皮皮瓣向下折疊。D,鎖眼,毛刺孔的位置,位於顳上線前部的後麵。鎖眼的上緣是硬腦膜前窩,下緣是眶周。 The inset shows the burr holes and bone flap. E, the sphenoid ridge has been removed leaving a thin shell of bone over the roof and lateral wall of the orbit. The bone removal is extended downward to increase access to the middle fossa floor. F, the dura and sylvian fissure have been opened to expose the supra- and parasellar areas.

點擊這裏查看此圖像的交互模塊和相關內容。
圖3.4。G-L。嗅道、視神經和動眼神經暴露在外。後交通動脈和基底動脈通過位於視神經、頸動脈和大腦前動脈之間的頸光三角可見。後交通動脈位於鞍上區動眼神經內側。G,通過額葉的進一步抬高暴露已經延伸到對麵。暴露包括視神經和同側和對側頸動脈和大腦中動脈。終板從視交叉向上延伸。垂體柄暴露在視交叉下方。H,額葉的進一步抬高暴露了對側大腦中動脈分叉處的側裂。 The pituitary stalk and contralateral oculomotor nerve are seen through the opticocarotid triangle. I, the left optic nerve has been elevated to expose the contralateral ophthalmic artery. J, the anterior clinoid process has been removed to expose the clinoid segment of the internal carotid artery. K–P, examines four routes to the apex of the basilar apex that can be accessed through a frontotemporal (pterional) craniotomy. These routes are: 1) through the opticocarotid triangle located between the internal carotid artery, optic nerve, and anterior cerebral artery; 2) through the carotid bifurcation-optic tract interval located between the bifurcation of the internal carotid artery and the optic tract; 3) through the carotid-oculomotor interval located between the carotid artery and the oculomotor nerve and above the posterior communicating artery; and 4) through the carotidoculomotor interval and below the posterior communicating artery. K and L, exposure directed through the opticocarotid triangle. K, pterional exposure of supra- and parasellar area in another specimen. The pituitary stalk and contralateral internal carotid artery are seen below the optic chiasm. L, the opticocarotid triangle has been opened by gently elevating the optic chiasm and displacing the carotid artery laterally to access the bifurcation of the basilar artery and the origin of both superior cerebellar and posterior cerebral arteries.

點擊這裏查看此圖像的交互模塊和相關內容。
圖3.4。先生。對側小腦上動脈是一條雙動脈。如果頸光三角大,如頸內動脈和大腦前動脈都很長,這種暴露是充分的,但如果頸內動脈和大腦前動脈都很短,且頸內動脈緊挨著視神經和交叉,這種暴露是不充分的。如果基底分叉特別高或位於鞍背以下,則基底分叉不能通過這條路線暴露。M和N,照射穿過頸動脈分叉視道間隔M,照射被重定向到頸動脈分叉上方的區域。N,頸動脈分岔被壓下視束被抬高暴露基底分岔。丘腦操作動脈起源於基底分支。O和P,暴露通過位於頸動脈和動眼神經之間的頸動脈動眼間隔。O,後交通動脈通過基底分支的前麵。 Gently depressing or elevating the posterior communicating artery, which crosses in front of the basilar artery, will increase access to the basilar apex. P, the posterior communicating artery has been elevated to expose the origin of the superior cerebellar arteries and the basilar bifurcation. Q and R, anterior subtemporal exposure obtained through the frontotemporal craniotomy by elevating the anterior part of the temporal lobe. Q, this oculomotor nerve arises from the medial surface of the cerebral peduncle and passes between the posterior cerebral and superior cerebellar artery to enter the roof of the cavernous sinus. R, the posterior communicating artery has been elevated to expose the basilar apex, both oculomotor nerves, and the junction of the right posterior communicating artery with the right posterior cerebral artery.

點擊這裏查看此圖像的交互模塊和相關內容。
圖3.4。sx。S和T,通過額顳開顱術暴露出高的基底動脈分叉,基底動脈可以通過光頸三角看到,但基底動脈分叉太高了,所以看不見。T,視束被輕輕地抬高頸動脈分叉被壓下露出基底動脈尖。U-X,顳下顱底下分支暴露。U,右側顳葉被抬高以暴露幕邊緣上方的視神經,動眼神經和滑車神經。後交通動脈向後穿過超內側到達動眼神經。基底分支位於鞍背後麵,就在穹幕邊緣的下方。V,幕邊緣在滑車神經與幕的連接處後麵被分開露出位於鞍背後麵的基底分叉。抬高大腦後動脈暴露丘腦工作動脈。 W, another exposure. The bifurcation is located behind the dorsum. The P1 extends upward on the medial side of the oculomotor nerve. X, the tentorium has been divided while preserving the trochlear nerve to expose the upper part of the basilar artery and the bifurcation. The posterior cerebral artery passes above and the superior cerebellar artery below the oculomotor nerve. A., artery; A.Ch.A., anterior choroidal artery; Ant., anterior; Bas., basilar; Bifurc., bifurcation; Brs., branches; Car., carotid; Clin., clinoid; CN, cranial nerve; Contra., contralateral; Dup., duplicate; Fiss., fissure; Lam., lamina; Olf., olfactory; Ophth., ophthalmic; Orb., orbital; P.C.A., posterior cerebral artery; P.Co.A., posterior communicating artery; Perf., perforating; Pit., pituitary; Post., posterior; S.C.A., superior cerebellar artery; Seg., segment; Sup., superior; Temp., temporal, temporalis; Tent., tentorial; Term., terminalis; Thal. Perf., thalamoperforating; Tr., tract.
起源於頸動脈-眼動脈交界處的動脈瘤通常起源於頸動脈上壁,位於眼動脈起源的遠端邊緣,位於海綿竇頂或以上,海綿竇頂的上向段向後轉向(圖3.2、3.3、3.5和3.6)。在這個轉彎時,最大的血流動力推力指向頸動脈上壁,離眼動脈遠一點,動脈瘤向上向視神經突出。
眼動脈的起點由於硬膜內長度較短且位於視神經下方,因此很難暴露(圖3.6)。它起源於視神經下方的頸動脈,經三種途徑之一到達眼眶。它通常通過視神經管進入眼眶。在少數病例中,它會發生在海綿竇,並通過眶上裂進入眼眶(5)。最不常見的途徑是穿透分隔視孔和眶上裂的骨支柱中的孔,或從腦膜中動脈發生(7)。
眼動脈起源地和床突前區動脈瘤是最複雜的動脈瘤之一,因為眼動脈的起源地和過程不同,並且在視神經孔和床突區域的硬腦膜皺襞被累及(圖3.6,A-C)。眼動脈瘤是相對簡單的,如果它們發生在顱底以上;然而,當它們越來越接近並涉及到頸內動脈的段(稱為側突段)時,複雜性就增加了,該段通過去除前側突暴露出來(圖3.4和3.7)(5)。側突段及其暴露將在本問題的第9章討論。床突段位於動脈海綿內段和蛛網膜下段的交界處,位於前床突上下緣的硬腦膜褶皺之間。硬腦膜從前床突頂部向內側延伸形成頸動脈周圍的硬腦膜上環。硬腦膜從前凸肌下緣向內側延伸包圍動脈形成下硬腦膜環,它標誌著下凸肌段的下緣。向內側延伸形成下硬腦膜環的這一層將床突的下緣與動眼神經的上表麵分開。上環在動脈周圍形成一個緊密的頸圈,但在手術顯微鏡下檢查發現,在硬腦膜中環與動脈前內側相包圍的位置經常有一個狹窄的凹陷,稱為頸動脈洞。洞穴,即向下的短袋,延伸到硬腦膜上環以下的可變距離(圖3.6,a和B),在動脈的前內側最突出,在那裏它可能向下延伸到下環附近。隨著年齡的增長,動脈拉長,洞穴似乎變得不那麼突出。 Carotid cave aneurysms are distinct from clinoid segment aneurysms, which arise from the clinoid segment of the internal carotid artery located between the upper and lower dural ring. Aneurysms that arise from the clinoid segment of the internal carotid artery have been referred to as clinoid segment aneurysms, and those located above the upper ring, but extending into the cave adjacent the upper ring, are referred to as carotid cave aneurysms.
眼動脈瘤的解剖結構不同,取決於眼動脈的起源位置和路徑,以及動脈瘤是否累及床突段或頸動脈腔。如果動脈瘤長在上環上方頸動脈的上表麵,它將向上投射進入視神經,既不累及窩段也不累及床側段(圖3.6、D和E)。如果眼動脈有更長的蛛網膜下腔段,並沿頸動脈上內側出現在上環遠端,動脈瘤可能在視神經的內側位於鞍前區下方,並與位於前麵的上垂體動脈瘤相似,盡管它起源於眼動脈的起點(圖3.6,F和G)。如果動脈瘤起源於頸動脈洞,眼底將在頸動脈的前內側向上延伸出頸動脈洞(圖3.6,F和G)。眼動脈也可能在頸動脈更近端的位置出現,並穿過視神經管的異位孔(視神經管外側緣與眶上裂內側緣之間的骨橋)到達眼眶,而不是穿過視神經管(圖3.6,J和K)。視神經管中的異位孔稱為眼孔(圖7.3L)。起源於眼動脈起點的動脈瘤通過視神經支柱,其頸部沿床突段或頸動脈腔的前部或外側,並從腔內向上突出進入蛛網膜下腔。第五種眼動脈瘤與眼動脈相關,眼動脈起源於海綿竇,通過眶上裂到達眼眶(圖3.6,L和M)。該動脈瘤指向上方,但幾乎立即碰到前床突的下緣,無法進入蛛網膜下腔。
眼動脈通常起源於視神經下方頸動脈上表麵的內側三分之一處(圖3.4和3.6C)。為了看到椎間孔前段,通常需要將視神經輕微抬高遠離頸內動脈。眼動脈在離開頸動脈後,可立即進入視神經管,但在大多數情況下,有2- 5mm的椎間孔前段。切除前床突和蝶小翼的鄰近部分,切除視神經孔的頂部和眶頂的鄰近部分以使視神經有一定的活動,以及切開鐮狀突,可使動脈瘤頸部暴露出來,硬腦膜的薄褶皺,從前突向內側延伸至鞍結節,覆蓋緊靠視神經孔的視神經段。切開硬腦膜上環,有時切開下環,以動員頸動脈進行動脈瘤夾閉是有幫助的。大多數眼動脈出現在前凸突尖端的前方,在凸突內側約5mm(3)。
從眼段起的穿通動脈起源於頸內動脈的後側或內側,分布於腦垂體柄、視神經、交叉和環繞漏鬥的第三腦室束和底部(圖3.5)。眼動脈瘤通常發生在頸動脈前壁上,而不是在穿通動脈產生的一側,並指向遠離眼段的穿通分支。由於眼動脈瘤通常指向上方,遠離這些穿孔分支,所以在切除眼動脈瘤時,損傷鄰近穿孔分支的風險比在頸內動脈的其他部位要小。
頸動脈在眼動脈起點的遠端和垂體上動脈起源於此段,在垂體柄外側區域有一個內凸曲線(圖3.2、3.3、3.5和3.6N)。正是在這個中間的凸曲線上出現了垂體上動脈瘤。動脈瘤起源於垂體上動脈起源的遠端邊緣,並向內側進入視交叉下表麵和鞍膈之間的區域。側位血管造影常將動脈瘤與海綿內動脈瘤混淆,因為它們通常位於視交叉下的蛛網膜下腔,但卻位於前臥突水平以下。上麵描述的垂體上動脈和眼段穿支在動脈瘤頸周圍伸展。
垂體上動脈是小分支,通常為兩條,發源於眼段的內側或後側(圖2.4、3.2)。(3)一個分支通常占主導地位。這些動脈向內側穿過,到達第三腦室底、視神經、交叉和垂體柄。如果動脈瘤向內側擴張,穿通動脈和垂體血管供應可能受到損害。尿崩和閉經可能是由於這些分支的閉塞造成的。切除前床突和鄰近的視神經管頂部和眼窩頂部通常有助於暴露垂體上動脈瘤頸部。在某些情況下,特別是在老年人中,眼動脈和頸內動脈的脊上部分可能會拉長,從而使眼動脈瘤的頸部更靠後,從而模擬垂體上動脈瘤視交叉下的位置和內側投影。
圖3.5。位於頸內動脈脊上部位的常見動脈瘤部位的穿通動脈。側麵圖。B,上位,右視神經和右半視交叉向前反射,暴露眼動脈的起源。A和B,眼動脈瘤起源於眼動脈的起點,從眼段向上指向視神經。眼段的穿支位於動脈瘤的內側。後交通動脈瘤起源於後交通動脈的起點,從交通段起,並指向動眼神經後方。從交通段產生的穿孔分支通常在後交通動脈瘤頸部周圍伸展。脈絡膜前動脈瘤起源於脈絡膜前動脈的起點,起源於脈絡膜段,並指向後外側。它們通常位於脈絡膜前動脈起源的上方或上方外側。 Aneurysms arising at the bifurcation into the anterior and middle cerebral arteries point upward lateral to the optic chiasm and tract toward the anterior perforated substance. The perforating branches arising from the choroidal segment are usually stretched along the posterior wall of the aneurysm arising at the bifurcation. A., artery; Ant., anterior; Comm., communicating; A.C.A., anterior cerebral artery; Chor., choroidal; Car., carotid; Hyp., hypophyseal; Infund., infundibulum; M.C.A., middle cerebral arteries; N., nerve; Ophth., ophthalmic; Post., posterior; Seg., segment; Sup., superior.

點擊這裏查看此圖像的交互模塊和相關內容。
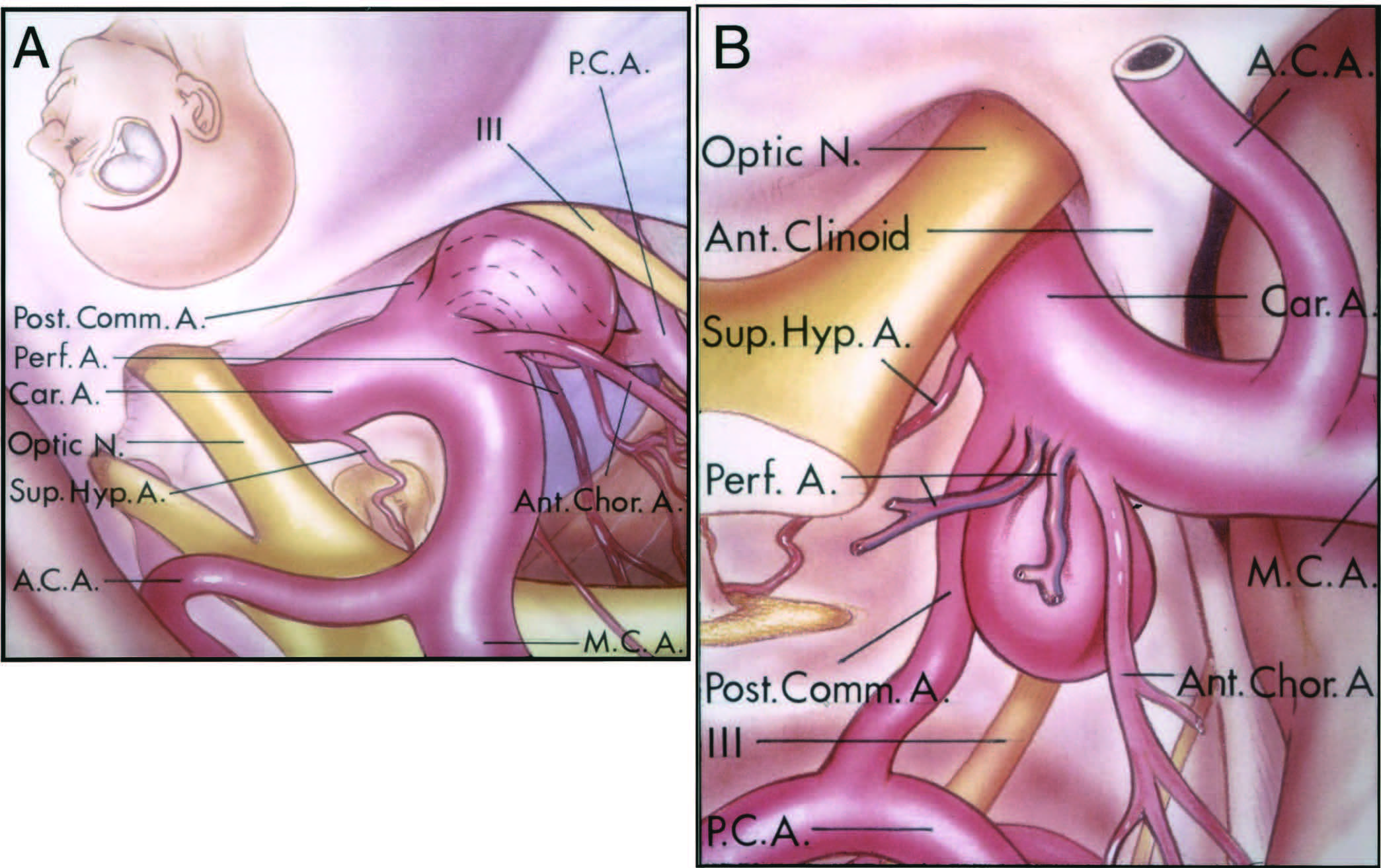
圖3.6。g。眼、垂體上動脈瘤與頸動脈床側段及頸動脈腔的關係。A,頸動脈的側突段位於前側突的內側。硬腦膜上環圍繞著側突的上緣,由硬腦膜從前側突的上緣向內側延伸而成。硬腦膜下環從前突下緣向內側延伸。眼動脈起於頸動脈最初的脊上段上表麵,在視神經下向前穿過進入視神經孔。上環似乎經常附著在頸動脈周圍形成頸圈。然而,在許多情況下,這個環和動脈的前內側之間有一個空間,向下延伸在動脈周圍形成一個洞穴,稱為頸動脈洞穴。在頸動脈前內側海綿竇頂部的洞穴最為明顯。 If the ophthalmic artery arises within the carotid cave, the neck of the aneurysm will also be located in the cave, and the aneurysm will extend upward out of the cave into the subarachnoid space. The superior hypophyseal artery arises from the medial wall of the internal carotid artery and courses toward the pituitary stalk. The optic strut is the bridge of bone that separates the optic foramen from the superior orbital fissure. This strut extends from the lower surface of the anterior clinoid process to the body of the sphenoid bone. The strut forms the inferolateral margin of the optic foramen. The anterior and middle cerebral arteries are also in the exposure. B, sagittal cross section through the clinoid segment and carotid cave. The cave extends downward between the upper dural ring and the wall of the carotid artery. The ophthalmic artery usually arises from the carotid artery immediately above the carotid cave and upper dural ring. A probe is inserted in the carotid cave, the space between the upper dural ring and the wall of the carotid artery. This clinoid segment of the carotid artery is situated medial to the anterior clinoid process. C, various patterns (1–5 in C) of the origin and passage of the ophthalmic artery that determine the degree of involvement by an aneurysm of the clinoid segment and carotid cave. 1, the ophthalmic artery arises from the superomedial wall of the artery well above the carotid cave. An aneurysm arising at the origin of this ophthalmic artery will mimic a superior hypophyseal aneurysm. 2, the ophthalmic artery arises in the carotid cave. 3, the artery arises just above the carotid cave. 4, the artery arises in the carotid cave and passes through the optic strut to enter the optic canal. 5, the artery arises in the cavernous sinus and passes through the superior orbital fissure. D and E, superior and anterior views of the most common ophthalmic aneurysm. This aneurysm arises above the clinoid segment and the carotid cave from the medial part of the superior wall of the carotid artery and projects upward into the optic nerve. The cavernous sinus is located below the anterior clinoid process in the anterior view. F and G, superior and anterior view of an ophthalmic aneurysm that mimics a superior hypophyseal aneurysm. The ophthalmic artery has a relatively long course to the optic foramen. This aneurysm projects medially below the optic chiasm and mimics the superior hypophyseal aneurysm, although it arises at the origin of the ophthalmic artery. The neck of the aneurysm is proximal to the origin of the superior hypophyseal artery. This aneurysm, on lateral angiography, may be seen medial to and below the upper margin of the anterior clinoid process.

點擊這裏查看此圖像的交互模塊和相關內容。
圖3.6。h n。H和I,硬腦膜上環以下,頸動脈腔內動脈瘤的上、前視圖。這個動脈瘤從頸動脈洞向視神經方向向上突出,硬腦膜上環環繞著它的基底。J和K,眼動脈瘤的上視圖和前視圖,該動脈瘤與眼動脈相連,起源於頸動脈腔,通過視神經支柱的孔到達視神經管。動脈瘤頸比典型的眼動脈瘤位於更外側的位置。動脈瘤從洞穴中向上突出進入蛛網膜下腔。L和M是海綿竇眼動脈起源處動脈瘤的上、前視圖。眼動脈穿過眶上裂到達眼眶。該動脈瘤位於床突段和頸動脈腔的下方,向上突出抵著前床突的下緣,但不到達蛛網膜下腔。 N, superior view of superior hypophyseal aneurysm. The aneurysm arises at the distal edge of the origin of the superior hypophyseal artery and points medially under the optic chiasm. A., artery; A.C.A., anterior cerebral artery; Ant., anterior; Car., carotid; Cav., cavernous; Clin., clinoid; Fiss., fissure; Hyp., hypophyseal; M.C.A., middle cerebral artery; N., nerve; Ophth., ophthalmic; Pit., pituitary; Seg., segment; Sup., superior.
頸動脈脊上肌的起始段向後,但垂體上動脈起源後的段向上轉向前穿孔物質,形成一條後凸的曲線(圖3.2、3.3、3.5和3.8)。後交通動脈和前脈絡膜動脈起源於後壁在這個凸曲線上當頸動脈向上延伸到它的分叉處。最常見的頸動脈動脈瘤發生在頸動脈-後交通動脈交界處。這些動脈瘤起源於頸動脈的後壁,靠近轉彎處,緊靠後交通動脈起源的遠端邊緣。這個區域另一個重要的關係是動眼神經與頸內動脈的關係。動眼神經進入硬腦膜,在硬腦膜後突外側硬腦膜內側從小腦幕向前棘突延伸。動眼神經穿過硬腦膜在最初的脊狀肌上段後2 - 7mm(平均5mm)處。動脈瘤起源於後交通動脈的起點,指向向下和向後,當其直徑達到4 - 5mm時,可壓迫進入海綿竇硬腦膜頂的動眼神經。
後交通動脈通常位於動脈瘤頸內側下方,前脈絡膜動脈位於動脈瘤頸上方或上外側(圖3.4、3.7和3.8)。在暴露頸動脈超過眼動脈起點時,外科醫生通常看到脈絡膜前動脈在後交通動脈之前,盡管脈絡膜前動脈出現在後交通動脈的遠端。這是因為三組解剖環境。首先,頸內動脈的頸線上段向後外側向上延伸,位於較遠端的分支,即脈絡膜前動脈的起點,比較近端的後交通動脈的起點更靠近中線。第二,脈絡膜前動脈比頸動脈後交通動脈在頸動脈後壁上的位置更靠外側。第三,脈絡膜前動脈比後交通動脈更外側;前者向視道下方的外側穿過,繞著腦梗,進入顳角,而後者則向動眼神經上方和內側的後內側方向通向踝間窩。在頸內動脈瘤閉塞時,應注意保存後交通動脈和脈絡膜前動脈。任何一條動脈的閉塞都可能導致偏癱、同位性偏盲和意識水平降低。
後交通動脈形成威氏圈的外側邊界,起於頸內動脈後內側表麵,向後伸展至蝶鞍上方,並在動眼神經上方和內側與大腦後動脈相連(圖3.4、3.7和3.8)。如果後交通動脈仍然是大腦後動脈的主要起源,則該構型稱為胎兒型。如果後交通動脈較小或正常大小,它向後內側方向與動眼神經內側的大腦後動脈連接,但如果是胎兒型,它向後外側方向在動眼神經上方或上方和外側。
與眼動脈或脈絡膜段相比,頸動脈交通段的穿支較少(圖3.5)(3)。然而,它們非常重要,因為其中一些穿支可能比脈絡膜前動脈或後交通動脈大,特別是在後動脈發育不良時。這些分支起源於動脈管壁的後半部分,位於動脈瘤頸的同一位置,通常在動脈瘤頸周圍伸展。這些分支終止於視交叉和道,第三腦室底,漏鬥,後穿孔物質和內側顳葉。

點擊這裏查看此圖像的交互模塊和相關內容。
圖3.7。A,眶顴骨開顱術和經海綿入路顱底尖。A,插圖(右上)顯示頭皮切口,插圖(右下)顯示兩片眶顴骨開顱術。額葉和顳葉被縮回以暴露視神經和動眼神經以及前、中大腦和後交通動脈。B,暴露已經被定向到視神經交叉上方的前交通動脈區域。C,頸動脈被抬高通過頸動脈和動眼神經之間的間隔暴露基底動脈尖。後床突阻斷了基底動脈的通路。D,前臥突和海綿竇的頂部已經被移除以提供通往頸內動脈的臥突段和後臥突的通道。硬腦膜上環從前床突上緣向內側延伸。E,後床突被切除以增加基底動脈上部的通路。 F, the anterior part of the tentorial edge has been removed to expose the upper margin of the posterior trigeminal root in Meckel’s cave and to provide increased access to the upper part of the basilar artery. The trochlear nerve was preserved in opening the anterior part of the tentorial edge. Note the difference in the length of basilar arteries exposed in C and F. A., artery; A.Ch.A., anterior choroidal artery; A.Co.A., anterior communicating artery; Bas., basilar; Car., carotid; Cav., cavernous; Clin., clinoid; CN, cranial nerve; Lam., lamina; P.Co.A., posterior communicating artery; Post., posterior; S.C.A., superior cerebellar artery; Seg., segment; Term., terminalis.
圖3.8。Carotid-posterior動脈瘤進行溝通。A,側位手術視圖。插圖(左上)顯示右側額顳開顱術的位置。動脈瘤起源於頸動脈後交通動脈起源的遠端邊緣,並向後向動眼神經延伸。後交通動脈在頸的下內側緣脈絡膜前動脈在頸的上外側緣。穿通動脈可能與後交通動脈或前脈絡膜動脈一樣大,出現在動脈瘤頸部周圍。暴露的其他結構包括視神經和前、中、後腦動脈和垂體上動脈。B,優越的觀點。後交通動脈位於動脈瘤頸的內下緣,前脈絡膜動脈位於動脈瘤頸的上外側緣,其穿支沿動脈瘤頸而出。 The anterior clinoid process is lateral to the carotid artery. A., artery; A.C.A., anterior cerebral artery; Ant., anterior; Car., carotid; Chor., choroidal; Comm., communicating; Hyp., hypophyseal; M.C.A., middle cerebral artery; N., nerve; P.C.A., posterior cerebral artery; Perf., perforating; Post., posterior; Sup., superior.
頸動脈脊上肌後凸曲線的頂端也可能位於脈絡膜前動脈起源地的水平,這使得血流動力從後交通動脈起源地遠端轉移到脈絡膜前動脈起源地(圖3.2、3.3和3.5)。起源於脈絡膜前動脈水平的動脈瘤通常位於脈絡膜前動脈起源的遠側、上側或上外側。它們指向後外側或後外側,通常遠在動眼神經之上。在打開椎間裂時,由於脈絡膜前動脈的起端和近端較外側,常先於後交通動脈暴露出來。
脈絡膜前動脈起源於頸動脈的後外側(圖3.4、3.7和3.8)(19)。它可能是兩條或兩條動脈。在這個區域產生的穿孔分支可能和脈絡膜前動脈一樣大。從它的起點開始,它在視神經束的後方延伸,並在顳角與脈絡膜叢相連而終止。閉塞引起可變的缺損,包括對側偏癱、半麻醉和偏盲。
脈絡膜段產生的動脈瘤通常比交通段或眼段產生的動脈瘤在頸部周圍有更多的穿孔支,因為脈絡膜段產生的穿孔支數量更多,而且大多數來自動脈瘤頸部所在的後壁(圖3.5和3.9)。平均有4個,但最多有9個,從這個節段的後壁產生穿孔分支。這些分支在脈絡膜段和頸內動脈分叉的後方通過,與大腦前動脈、循環動脈、大腦中動脈和脈絡膜前動脈的穿支一起進入前穿孔物質,並上升到內囊(3,19)。動眼神經缺陷,經常發生在頸動脈-後交通動脈瘤,是不常見的,很少發生在破裂前。
第五個動脈瘤位於頸內動脈的分叉處。這些動脈瘤最容易符合上述四個原則(圖3.2、3.3、3.5和3.9)。這些動脈瘤出現在t形分叉的頂端。它們向上指向動脈前分叉段的長軸方向指向前穿孔物質。起源於頸內動脈脈絡膜段和大腦前動脈和中動脈近端的穿支延伸到頸後側和動脈瘤壁周圍,應剝離動脈瘤(圖3.4、3.5、3.7和3.9)。
![圖3.9。進入前穿孔物質的動脈與常見動脈瘤部位的關係。A,側視圖,B,上位視圖。貫穿這些動脈的動脈瘤發生在四個部位:(a)位於脈絡膜前動脈起源處的頸內動脈;(b)頸內動脈末端分叉進入大腦前動脈和大腦中動脈;(c)大腦中動脈分叉;(d)前交通動脈區域。發生於頸內動脈後交通動脈水平的動脈瘤不涉及到前穿孔物質的分支,除非它們變得非常大。動脈瘤起源於頸內動脈,位於或遠於脈絡膜前動脈,指向後外側和後外側,並可能有分支與前穿孔物質分別來自頸內動脈和頸部附近的脈絡膜前動脈,以及位於下緣或內緣的脈絡膜前動脈。起源於頸動脈分叉處的動脈瘤頸動脈穿支在頸後向上穿過進入前穿孔物質,與內側紋狀體動脈和A1近端穿支進入前穿孔物質的位置相鄰。 The recurrent artery passes above the carotid bifurcation and may be incorporated into the arachnoidal bands around the neck and fundus of this aneurysm. Aneurysms arising at the bifurcation of the middle cerebral artery commonly have the origin of some of the lateral lenticulostriate arteries near their neck. If the prebifurcation segment of the M1 is very short, the intermediate lenticulostriate arteries will arise near the neck. The aneurysm arising at the level of the anterior communicating artery is located above the optic nerve and chiasm at the junction of the A1 and A2 segments of the anterior cerebral artery. This aneurysm usually arises in the setting where one A1 segment is dominant and the opposite A1 segment is hypoplastic. The A1 perforating branches and the recurrent artery arise near the neck of the aneurysm. C, operative exposure through a frontotemporal craniotomy. The sylvian fissure has been opened between the frontal and temporal lobes. The inset (upper left) shows the skin incision (solid line), the site of the craniotomy (dotted line), and the craniectomy (hatched area). A., arteries, artery; Ant., anterior; Car., carotid; Chor., choroidal; Comm., communicating; Fiss., fissure; Front., frontal; Int., intermediate; Lat., lateral; Len. Str., lenticulostriate; Med., medial; N., nerve; Perf., perforating; Post., posterior; Rec., recurrent; Temp., temporal. (From, Rosner SS, Rhoton AL Jr, Ono M, Barry M: Microsurgical anatomy of the anterior perforating arteries. J Neurosurg 61:468–485, 1984 [19].)](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Aneurysms_3.9.jpg)
圖3.9。進入前穿孔物質的動脈與常見動脈瘤部位的關係。A,側視圖,B,上位視圖。貫穿這些動脈的動脈瘤發生在四個部位:(a)位於脈絡膜前動脈起源處的頸內動脈;(b)頸內動脈末端分叉進入大腦前動脈和大腦中動脈;(c)大腦中動脈分叉;(d)前交通動脈區域。發生於頸內動脈後交通動脈水平的動脈瘤不涉及到前穿孔物質的分支,除非它們變得非常大。動脈瘤起源於頸內動脈,位於或遠於脈絡膜前動脈,指向後外側和後外側,並可能有分支與前穿孔物質分別來自頸內動脈和頸部附近的脈絡膜前動脈,以及位於下緣或內緣的脈絡膜前動脈。起源於頸動脈分叉處的動脈瘤頸動脈穿支在頸後向上穿過進入前穿孔物質,與內側紋狀體動脈和A1近端穿支進入前穿孔物質的位置相鄰。 The recurrent artery passes above the carotid bifurcation and may be incorporated into the arachnoidal bands around the neck and fundus of this aneurysm. Aneurysms arising at the bifurcation of the middle cerebral artery commonly have the origin of some of the lateral lenticulostriate arteries near their neck. If the prebifurcation segment of the M1 is very short, the intermediate lenticulostriate arteries will arise near the neck. The aneurysm arising at the level of the anterior communicating artery is located above the optic nerve and chiasm at the junction of the A1 and A2 segments of the anterior cerebral artery. This aneurysm usually arises in the setting where one A1 segment is dominant and the opposite A1 segment is hypoplastic. The A1 perforating branches and the recurrent artery arise near the neck of the aneurysm. C, operative exposure through a frontotemporal craniotomy. The sylvian fissure has been opened between the frontal and temporal lobes. The inset (upper left) shows the skin incision (solid line), the site of the craniotomy (dotted line), and the craniectomy (hatched area). A., arteries, artery; Ant., anterior; Car., carotid; Chor., choroidal; Comm., communicating; Fiss., fissure; Front., frontal; Int., intermediate; Lat., lateral; Len. Str., lenticulostriate; Med., medial; N., nerve; Perf., perforating; Post., posterior; Rec., recurrent; Temp., temporal. (From, Rosner SS, Rhoton AL Jr, Ono M, Barry M: Microsurgical anatomy of the anterior perforating arteries. J Neurosurg 61:468–485, 1984 [19].)
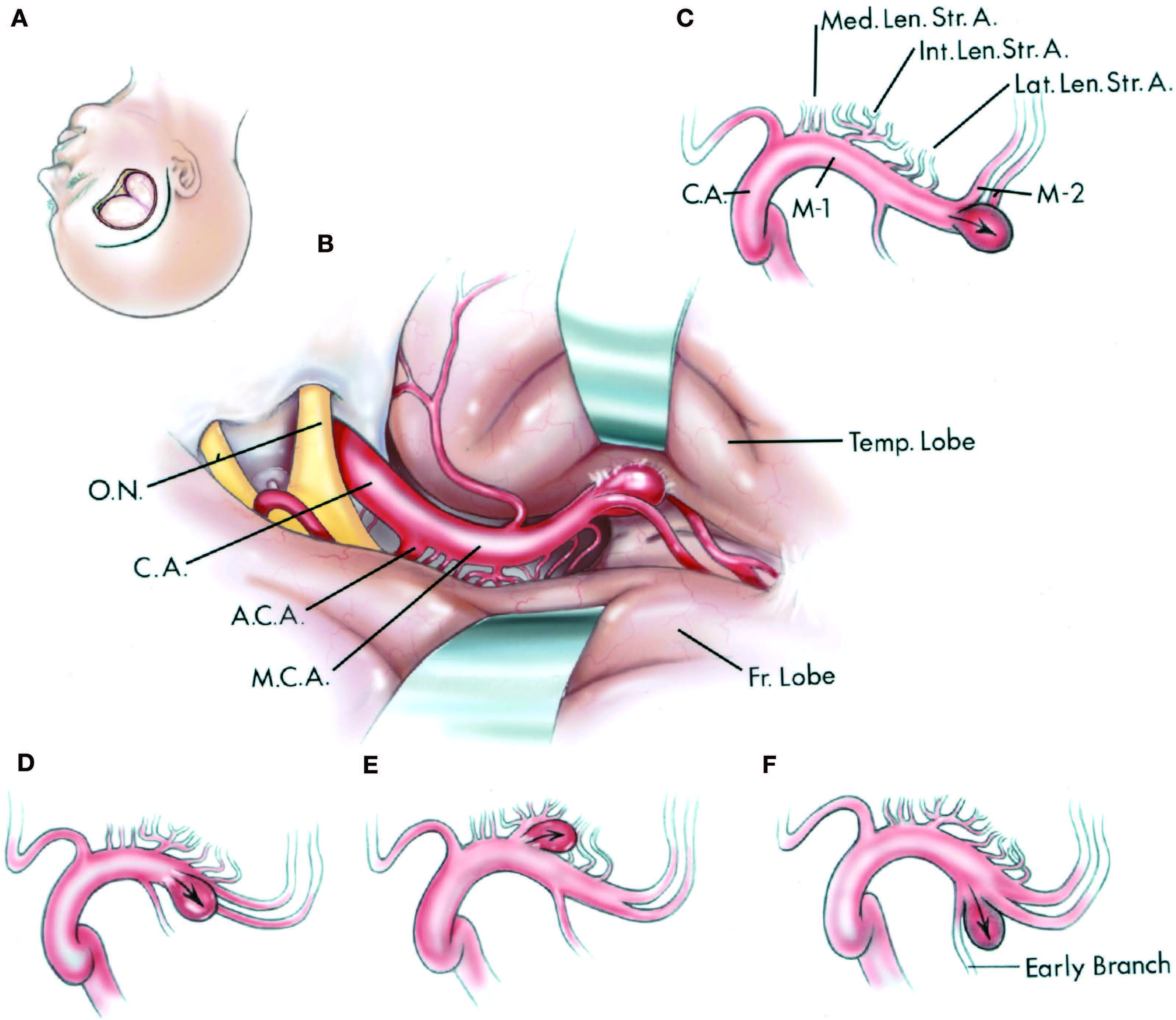
大腦中動脈是囊狀動脈瘤最常見的部位之一。這些動脈瘤也符合解剖學的四個原則(圖3.9和3.10)(2)。它們最常發生在動脈的第一個主要分岔或三分岔的水平。分叉的主幹與主幹形成的角度形成了拐彎或曲線。這些動脈瘤通常指向主幹預分叉段長軸的橫向方向。
大腦中動脈分為4段,M1到M4。M1段開始於大腦中動脈的起點,並在前穿孔物質的下方向外側延伸到M2段開始的地方,該段開始於動脈向後急轉彎的地方,在一個稱為膝的轉彎處到達腦島。囊狀動脈瘤是在M1段或M1段和M2段的交界處出現的。M1段被細分為分岔前和分岔後部分。預分岔部分由一個單一的主幹組成,從原點延伸到它的第一個主要分支,這是大多數半球的分岔。在大多數半球,分叉發生在膝的近端。分叉近端的M1段產生的小皮層分支稱為早期分支,可能是分叉近端的動脈瘤的起源部位。早期的分支指向額葉和顳葉。
大腦中動脈到前穿孔物質的分支稱為紋狀體動脈(圖2.30、2.31、3.9和3.10)。平均而言,每個半球(19個)有10個(範圍1-20個)莢狀紋狀動脈。80%的紋狀體動脈起源於M1段的分叉前部分,17%起源於M1段的分叉後部分,3%起源於M2段近膝處的近端部分。分叉越早,分叉遠端出現的分支數量越多。動脈瘤很少發生在大的莢狀紋狀分支的起源處。莢狀紋狀動脈分為內側、中間和外側組(圖2.30和3.9)(19)。每一組在前穿孔物質中都有獨特的起源、組成和特征分布。每一組的不同形態導致內側組被稱為直的,因為它們追求直線的路線,中間組被稱為燭台,因為它們接近前穿孔物質的複雜分支,而外側組被稱為S形,描述其彎曲的路線。這三組病例均發生在裂裂的側裂和動脈內側。圍繞動脈瘤頸部延伸的穿孔分支的數量和類型取決於分支的水平(圖3.9和3.10)。 If the prebifurcation segment is very short, the neck of the aneurysm may have the straight or candelabra branches stretched around the neck, whereas an aneurysm arising at the apex of a long prebifurcation segment may involve the area of the S-shaped lenticulostriate branches.
有助於解剖頸部和從動脈瘤壁分離穿通動脈的工具包括40度角淚滴夾層和1、2或3毫米寬的鏟式夾層(圖3.11)(14,15)。1.5毫米杯的小角刮匙在去除床突上的硬腦膜時是有用的。一個5法吸,10厘米長提供了一個有用的吸解剖器。切割蛛網膜帶的合適長度是刀柄為9.5厘米的刺刀剪刀。為了抓取和分離蛛網膜粘連,需要使用針尖內側有細鋸齒的卡口組織鉗。腦鏟從基部的10或15mm到尖端的5或10mm逐漸變細,適用於在大多數動脈瘤部位抬高大腦。
圖3.10。大腦中動脈瘤。A,頭皮切口和開顱術,以接近大腦中動脈上的動脈瘤。B,右額顳開顱術的手術視圖。右邊的神經裂已經被切開以提供視神經和頸動脈以及大腦中動脈和前動脈的圖像。腦鏟位於顳葉和額葉。C,中腦動脈瘤通常位於動脈膝附近的分叉處。箭頭顯示動脈瘤部位血流動力的方向。內側、中間和外側紋狀動脈起源於大腦中動脈。D,動脈瘤起源於早期分岔。 E, aneurysm arising at a large lenticulostriate branch. F, aneurysm arising at an early branch. A., arteries, artery; A.C.A., anterior cerebral artery; C.A., internal cerebral artery; Fr., frontal; Int., intermediate; Lat., lateral; Len.Str., lenticulostriate; M.C.A., middle cerebral artery; Med., medial; O.N., optic nerve; Temp., temporal.

圖3.11。動脈瘤剝離的器械。A, 40度角淚滴解剖器從基底動脈動脈瘤頸部分離出穿支和蛛網膜帶。5法氏大小的鈍頭吸力提供吸力,並有助於動脈瘤頸部的收縮進行剝離。暴露的結構包括小腦上動脈、後交通動脈、後腦動脈、丘腦操作動脈和動眼神經。B,用抹刀解剖器將動脈瘤壁收縮,用微剪刀將頸部周圍堅硬的蛛網膜帶分開。C, 40度角淚滴解剖器,用於確定頸部並從動脈瘤頸部分離穿孔血管。D,帶1.5 mm罩杯的角型微刮匙,用於從前床突移除硬腦膜。E:用於定義頸部和從動脈瘤壁分離穿孔血管的鏟刀解剖器。F,鈍頭抽吸5法尺大小用於抽吸和動脈瘤夾層。 A 7- or 9-French blunt tip suction may be needed if heavy bleeding should occur. G, bayonet forceps with 9.5-cm blades and 0.5-mm tips with small serrations (inset) inside tips for grasping arachnoidal and fibrous bands around an aneurysm. H, bayonet microscissors with 9.5-cm shafts and straight and curved blades (inset) for dividing adhesions around the neck of the aneurysm. I, the brain spatulas most commonly used to elevate the brain in aneurysm surgery are tapered from 10 or 15 mm at the base to 5 or 10 mm at the tip. A., arteries, artery; Bas., basilar; Com., communicating; P.C.A., posterior cerebral artery; Post., posterior; S.C.A., superior cerebellar artery; Th.Perf., thalamoperforating.
大腦前動脈上最常見的動脈瘤部位位於前交通動脈的水平(圖3.12)。這些動脈瘤由於解剖結構的變化和難以完全顯示該區域的主幹和穿通動脈而變得複雜(12)。大腦前動脈在頸內動脈與前交通動脈之間的那段稱為A1段,前交通動脈與胼胝體口之間的那段稱為A2段。動脈瘤通常發生在一個A1段發育不良,而占主導的A1段長出兩個a2段的情況下(圖3.12)。動脈瘤發生在主要的A1段在前交通動脈的水平分岔處,產生左右A2段。這些動脈瘤通常從主動脈瘤段指向另一側。它們也可能投射到其他方向。眼底點的方向是由大腦前動脈與前交通動脈連接處近端的路線決定的。動脈的彎曲可能會造成血流動力推力不同的情況,因此這些動脈瘤不僅會向相反方向投射,也會向前、後或下方向投射(圖3.12)。
大腦前動脈產生大量的穿支(圖2.16、2.24、3.9和3.13)。這些分支有兩個來源。首先,A1節段產生直接通向前麵穿孔物質的分支;第二,A1段和A2段的近端形成了返動脈。大腦前動脈的返支是通向前穿孔物質的最大最長的分支。這可能是在額葉向上靠近前交通動脈瘤時看到的第一根動脈(圖3.13)。它在動脈中是獨特的,因為它在其母血管上加倍,穿過頸動脈分叉上方,在進入前穿孔物質之前,伴隨大腦中動脈進入側裂。如果A1段發育不良,一側的複發動脈可能與發育不良的A1段一樣大,甚至可能與A1段混淆,因為兩者都將沿著頸動脈分叉和半球間裂之間的區域穿過(圖2.24和3.13)。再發動脈可以位於A1段的任何方向。它的起源可能附著在前交通動脈瘤的壁上。 The inverting adventitia of A1 may so obscure the recurrent artery that inadvertent occlusion by a clip may easily occur, even under the operating microscope. The recurrent artery pursues a long, redundant path, looping forward on the gyrus rectus or the posterior part of the orbital surface of the frontal lobe where it could be damaged and occluded in removing the posterior 1 or 2 cm of the gyrus rectus, as is common practice in exposing anterior communicating aneurysms (Fig. 3.9). It may arise from a common stem with the frontopolar artery (Fig. 3.13). Ischemia in the area supplied by Heubner’s artery may cause hemiparesis with facial and brachial predominance, because of compromise of the branch supplying the anterior limb of the internal capsule, and may cause aphasia if the artery is on the dominant side (19).
前交通動脈是通向視交叉背表麵和視交叉上區域的多達四個穿孔分支的起點(圖2.16和2.24)(11)。這些穿孔分支遍布穹窿、胼胝體和鼻中隔區。它們的閉塞會導致人格和記憶障礙。
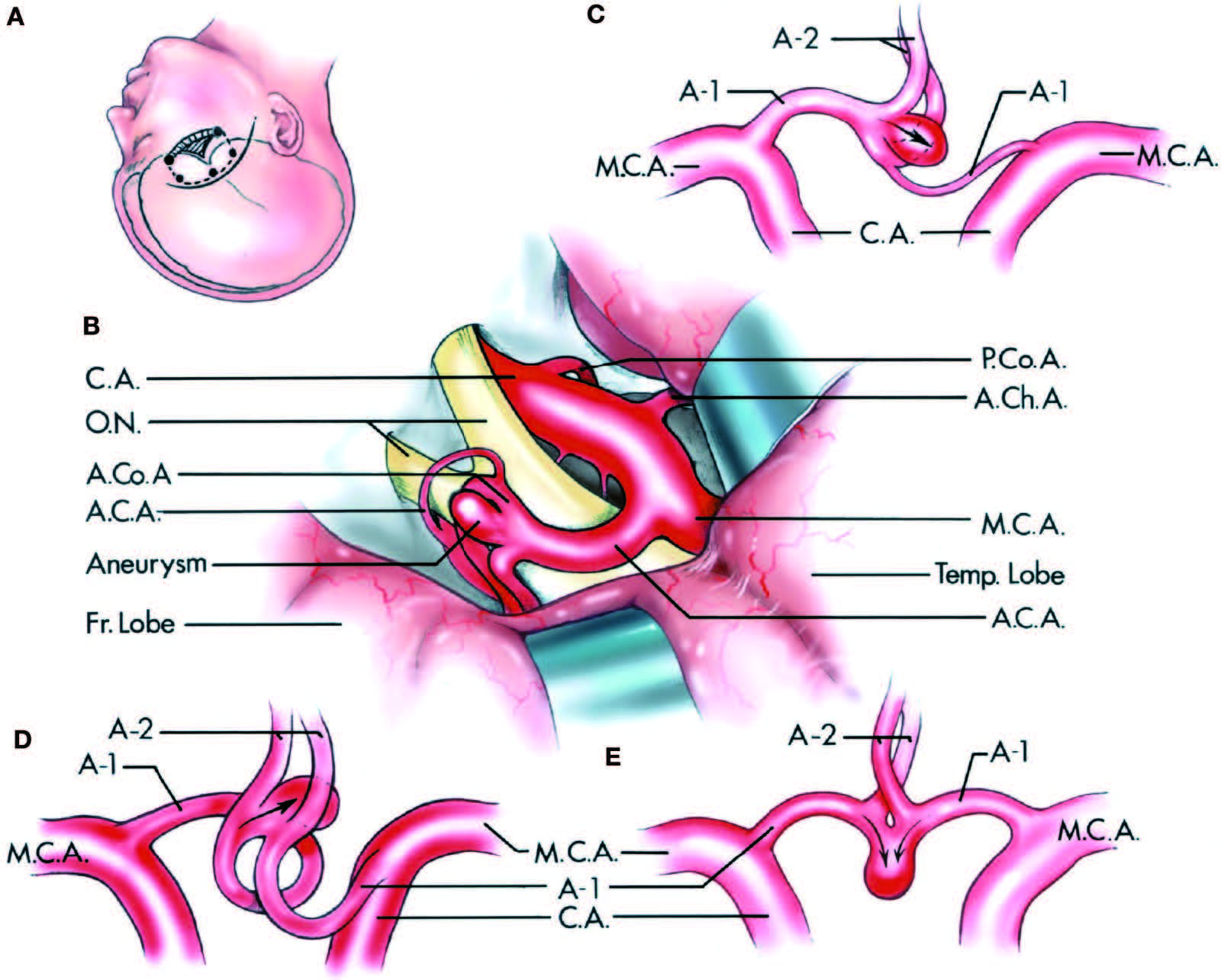
圖3.12。前交通動脈瘤。A,頭皮切口(實線),骨瓣(虛線)和顱骨切除術(孵化區)。B,最常見的前交通動脈瘤的手術視圖。動脈瘤向下和向前指向遠離大腦前動脈。暴露的結構包括頸動脈,前大腦,中大腦,前通信,後通信,前脈絡膜動脈,視神經,額葉和顳葉。C, D和E,前視圖顯示了大腦前動脈近端和遠端不同大小和形狀的血流動力(箭頭)所形成的三種不同動脈瘤構型。最常見的動脈瘤(C)與A1段發育不良有關。較不常見的動脈瘤突出部位為後(D)或直前(E)。眼底指向的方向由動脈與前交通動脈連接處的近端方向決定。A.C.A,大腦前動脈; A.Ch.A., anterior choroidal artery; A.Co.A., anterior communicating artery; C.A., internal carotid artery; Fr., frontal; M.C.A., middle cerebral artery; O.N., optic nerve; P.Co.A., posterior communicating artery; Temp., temporal.
圖3.13。複發動脈起源和路徑的變異。A,返動脈起於A1和A2節段的交界處,並在頸動脈分叉的上方向外側穿過,分布在前穿支物質的長條上。它通常在直回向前循環,在那裏,當切除一小塊回以暴露前交通動脈瘤時,它可能會受傷。B,在頸動脈分叉和半球間裂之間的區域內,返動脈可能和發育不良的A1段一樣大或更大。當從頸動脈分叉向內切開到前交通動脈區域時,這可能是在額葉上升時看到的第一根動脈。它經常在直回向前循環,很容易被破壞,因為直回的後厘米被切除,暴露出A1和A2節的交界處。C,返動脈與額極動脈是共同的主幹,向外側穿過直回。D,返動脈起源於A1段。一個,動脈; Ant., anterior; Car., carotid; M.C.A., middle cerebral artery; N., nerve; Olf., olfactory; Perf., perforated; Rec., recurrent; Subst., substance.
大腦前動脈遠端下一個最常見的動脈瘤部位是胼胝體動脈起源於胼胝體周動脈的水平,通常靠近胼胝體前部,靠近在膝處的動脈最大角度處(圖2.22和3.14)。這條曲線是由分支的成角和動脈繞過胼胝體的端部形成的。動脈瘤遠端指向胼胝體周動脈和胼胝體小動脈的交界處。不尋常的變異,如兩根胼胝體周動脈在其主要分叉處的連接,可能通過產生血流動力學的改變而引起動脈瘤。
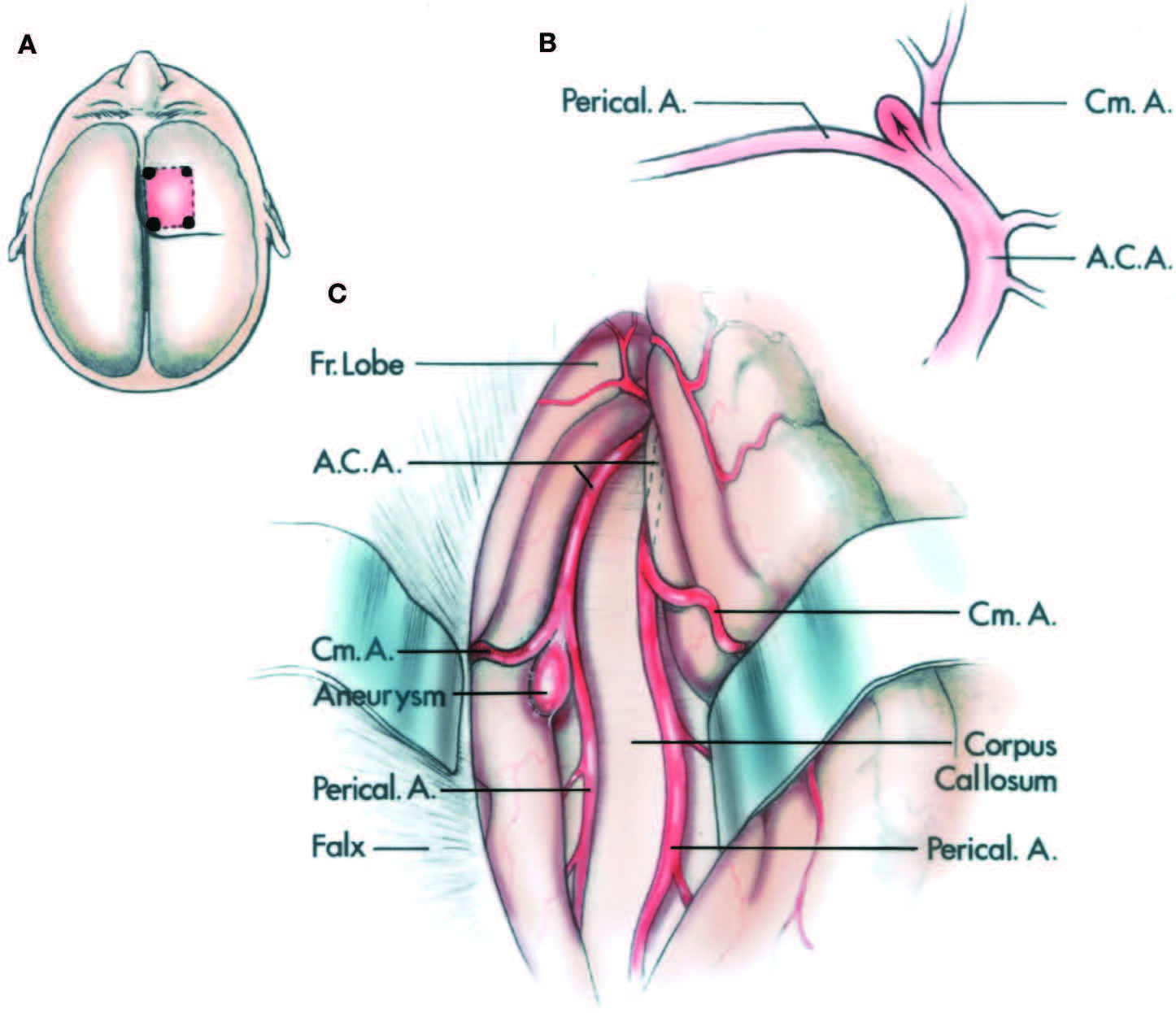
圖3.14。大腦前動脈遠端最常見動脈瘤部位的側位和手術視圖。A,頭皮切口(實線)和骨瓣(虛線)。B,右大腦前動脈的內側表麵。動脈瘤位於胼胝體前緣額葉內側表麵。血流動力學推力(箭頭)和動脈瘤指向遠端在胼胝體周動脈和胼胝體動脈之間。C,右額葉收縮,露出大腦前動脈,鐮狀動脈,以及胼胝體上方的動脈瘤,位於胼胝體和胼胝體周圍動脈的起源處。如果胼胝體和動脈瘤的起源位於胼胝體以下,則暴露的中心可能在前額下方。一個,動脈;A.C.A,大腦前動脈; Cm., callosomarginal; Fr., frontal; Perical., pericallosal.
大約15%的囊狀動脈瘤發生在椎基底動脈係統,其中大部分(63%)發生在基底動脈分支。與正常組相比,動脈瘤中發育不良或胎兒後腦起源的異常發生率更為常見。發生在椎動脈和基底動脈分支上的動脈瘤也具有上述的四個解剖學方麵。它們出現在曲線上的根尖分支位置,指向如果曲線不存在,血液會沿著的方向,並被一組不斷出現的穿孔分支包圍(圖3.15)。基底動脈尖動脈瘤發生在大腦後動脈從基底動脈分支處,並向上指向基底動脈長軸方向(圖3.15和3.16,A和B)。由於這些變化,在頸動脈和椎動脈造影上可以看到大腦後動脈動脈瘤,特別是當P1段發育不全(胎兒型)時。
起源於小腦上動脈或小腦前下動脈起源地水平的基底動脈,或起源於小腦後下動脈起源地水平的椎動脈的動脈瘤,最初似乎不符合適用於其他動脈瘤的前三個解剖麵,因為基底動脈和椎動脈通常被描繪成直動脈,而小腦動脈與它們呈直角起源地(圖3.15)(18)。然而,大多數動脈瘤的動脈是彎曲的,與彎曲相關的血流方向的變化在基底動脈或椎動脈靠近小腦動脈起源處的動脈壁上產生了血流動力學應力。這些動脈瘤所指向的方向是,如果在受損傷分支的起始位置沒有曲線,血液就會流向這個方向。
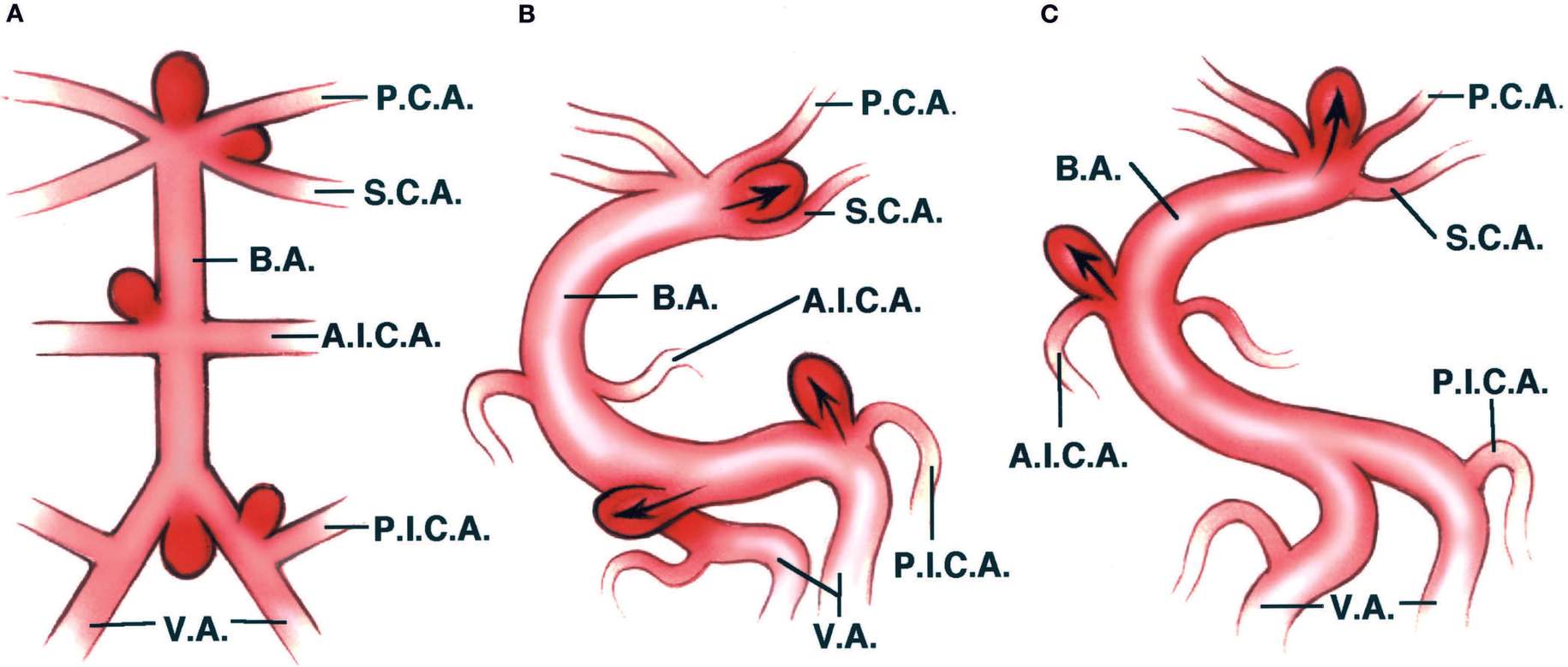
圖3.15。椎動脈和基底動脈上的動脈瘤部位。A,常用的椎動脈、基底動脈和動脈瘤部位的圖解表示,通常被證明是不正確的。椎動脈和基底動脈常顯示為直血管,腦後動脈、小腦上動脈、小腦前下動脈和小腦後下動脈顯示為與母動脈成直角突起,動脈瘤與母動脈的流動方向呈近直角突起。B和C,與動脈瘤相關的常見結構,基底動脈和椎動脈的彎曲產生的血流動力指向分支部位附近的管壁,動脈瘤指向動脈瘤部位近端的血流動力推力方向。椎動脈的動脈瘤出現在其連接與下方壓迫小腦動脈和基底動脈的基底動脈的動脈瘤(B)。出現後大腦和小腦上動脈之間(B),在基部的頂端(C),下小腦動脈的起源(C),所有點的方向長軸的preaneurysmal段動脈和最大血流動力學推力的方向(箭頭)動脈瘤的網站。A.I.C.A,小腦前下動脈;學士,底動脈;腦後動脈;P.I.C.A,小腦後下動脈; S.C.A., superior cerebellar artery; V.A., vertebral artery.
圖3.16。常見動脈瘤位置在後顱窩。右上方的圖表顯示了基底動脈、椎動脈、腦後動脈、小腦上動脈、小腦後下動脈和小腦前下動脈;動脈瘤的位置;以及動脈瘤部位血流動力的方向(箭頭)。左上角的圖表顯示了用於暴露動脈瘤的頭皮切口(虛線)和骨瓣(實線)或顱骨切除術(蛋殼區)。A,右側前顳下開顱術顯示腦後動脈起源處有顱底尖動脈瘤。注意頭皮切口和骨瓣或顱骨切除術。牽開器位於顳葉上,小腦幕被切開,暴露基底動脈、腦後動脈、小腦上動脈、後交通動脈、頸內動脈以及動眼神經、滑車神經和三叉神經。B,額顳入路暴露基底尖動脈瘤。 The sylvian fissure has been split and the frontal and temporal lobes are retracted to expose the aneurysm. The middle cerebral, anterior cerebral, and anterior choroidal arteries and the optic nerves are also exposed. The carotid artery is retracted with a spatula dissector to expose the aneurysm. C, anterior subtemporal exposure of a basilar aneurysm arising between the origin of the superior cerebellar and posterior cerebral arteries. The basilar artery curvature creates a hemodynamic thrust (arrow) against the wall of the artery at the junction of the upper two branches of the basilar artery. The aneurysm projects laterally below or into the oculomotor nerve. D, anterior subtemporal exposure of a basilar aneurysm arising at the origin of the anteroinferior cerebellar artery. The abducens nerve is below the anteroinferior cerebellar artery. The tentorium is split laterally above the trigeminal nerve to expose the facial and vestibulocochlear nerves. The curvature of the basilar artery creates a hemodynamic thrust (arrow) against the wall of the artery at the junction of the basilar and anteroinferior cerebellar arteries. E, suboccipital exposure of an aneurysm arising at the junction of the vertebral and basilar arteries. Although shown here in the upright position, the operation shown in E and F is performed in the three-quarter prone position. The right half of the cerebellum is elevated to expose the facial, vestibulocochlear, glossopharyngeal, vagus, and spinal accessory nerves and the internal acoustic meatus. One of the vertebral arteries often joins the other in a configuration resembling the branching seen at other aneurysm sites or is associated with a fenestration in the lower basilar artery. Angiographic views in multiple projections reveal the aneurysm pointing in the direction of flow in the preaneurysmal segment of the larger vertebral artery. F, suboccipital exposure of an aneurysm arising at the origin of the right vertebral and posteroinferior cerebellar arteries. The angulation of the vertebral artery creates a hemodynamic thrust (arrow) in the direction in which the aneurysm points. The flocculus and choroid plexus protrude into the cerebellopontine angle. A.C.A., anterior cerebral artery; A.Ch.A., anterior choroidal artery; A.I.C.A., anteroinferior cerebellar artery; B.A., basilar artery; C.A., internal carotid artery; Ch., choroid; Fr., frontal; M.C.A., middle cerebral artery; O.N., optic nerve; P.C.A., posterior cerebral artery; P.Co.A., posterior communicating artery; P.I.C.A., posteroinferior cerebellar artery; Pl., plexus; S.C.A., superior cerebellar artery; Temp., temporal; Tent., tentorium; V.A., vertebral artery.
15%的動脈瘤發生在椎-基底動脈係統中,其中大部分位於基底動脈分叉處的Willis圓的後部(圖3.4、3.15和3.16,A和B)。基底動脈尖動脈瘤發生在大腦後動脈與基底動脈的分支處。動脈瘤部位的曲線與基底動脈的垂直方向向腦後動脈的側向方向的變化有關。這些動脈瘤沿基底動脈長軸方向向上突出。基底分叉最常位於足間窩對麵,但也可能位於橋腦前部的橋腦-腦腦交界處以下1.3 mm處,或遠至乳頭體吻側處(20)。高分叉可使乳頭狀體和第三腦室底向上擠壓。高或低分叉最好由顳下路徑接近,而不是翼點路徑。
在基底動脈瘤的顳下入路中,最好沿著大腦後動脈的下側內側繞著椎弓根彎曲,找到分叉處的動脈瘤頸部,因為下表麵是穿孔分支最不常見的起始部位,因此是P1和基底動脈瘤分叉最安全的入路(圖3.17和3.18)。
基底分岔區域可能是多種異常的部位(20,22)。大腦後動脈在基底分支和後交通動脈之間的部分稱為P1,而在交通動脈遠端的部分稱為P2。一個正常的後圓,定義為兩個P1節段的直徑大於它們的後交通動脈,後者沒有發育不良,在大約一半的病例中被發現。在其餘病例中,發現的異常包括發育不良的後交通動脈或胎兒排列,其中P1段發育不良,後交通動脈為大腦後動脈提供主要供血。
發育不良的後交通動脈,或大腦後動脈主要起源於頸動脈的胎兒形態,可在一側或兩側發現(圖2.8和2.34)。假設基底分岔動脈瘤的分支較少,建議通過橫斷發育不良的後交通動脈或P1段進入基底分岔動脈瘤。然而,射孔分支的數量和直徑是相對恒定的,與主幹尺寸無關;因此,低發育段雖然尺寸較小(20),但提供的射孔麵積與較大的導管相同。
威利斯圓的後部有一係列穿通動脈進入間腦和中腦,這些穿通動脈可能在基底尖動脈瘤周圍伸展。其中最重要和最大的是丘腦工作動脈,它起源於基底尖動脈瘤區域的P1(圖3.18和3.19)(20,22)。它們起源於P1,並通過後穿孔物質進入上頜體後的大腦,在腦梗間窩和內側腦梗。它們都是P1的最大分支,在大多數情況下也是離分支最近的分支。一個P1可能不會產生丘腦操作動脈,在這種情況下,對側發育良好或占主導地位的丘腦操作支將供應由兩個P1分支正常灌注的區域。阻塞這些重要的穿孔血管的風險包括視力喪失、癱瘓、軀體感官障礙、虛弱、記憶缺陷、自主和內分泌失調、異常運動、複視和意識壓抑。
基底動脈上厘米的後外側表麵也是穿孔動脈的豐富來源。平均有8個分支(範圍3-18)從上部厘米生長(圖2.34和2.35)(20,22)。大約一半來自後表麵,四分之一來自兩側。基底動脈前表麵很少出現穿支。顱底分岔動脈瘤的患者比其他部位動脈瘤的患者被觀察得更嚴重,因為在動脈瘤剝離和夾閉中更容易出現重要的穿支。在基底分岔動脈瘤中,動脈瘤越靠後,預後越差,因為隨著動脈瘤向後方突出,重要的穿支的浸潤傾向就越大(1)。基底分岔的前表麵很少是穿支的位置,因此前突出動脈瘤的手術效果更好。位於顱底後表麵,分支下方2 - 3mm的豐富神經叢,進入椎間窩並終止於中腦內側,使此部位成為最危險的部位。顱底尖處於中等危險,因為在手術中更容易識別丘腦動脈,並且比分支的後側穿支少。
位於腦後動脈起源遠端的動脈瘤是不常見的。最常見的位置是在第一主幹的起源處,因為大腦後動脈在腳池或周圍池的P1或P2上環繞中腦。遠端大腦後動脈動脈瘤在被識別之前往往比其他動脈瘤更大,通常與該區域的腫瘤相似。腦後動脈瘤最常見的神經功能障礙是部分或完全的動眼神經功能障礙。

點擊這裏查看此圖像的交互模塊和相關內容。
圖3.17。基底動脈和大腦後動脈的前和中顳下暴露。A,開顱瓣和硬腦膜開口暴露了顳葉和中顱窩底。圖示頭皮切口的位置。B,顳葉被抬高以暴露大腦後動脈和小腦上動脈。大腦後動脈在上方小腦上動脈在動眼神經下方。小腦上動脈分支與滑車神經沿腦幹側走行。C,大腦後動脈被壓下露出基底動脈。脈絡膜前動脈起源於頸內動脈,通過腦梗和鉤椎之間進入顳角。D幕在岩脊後麵被分開露出基底動脈上部,小腦上動脈,三叉神經和滑車神經。 The medial posterior choroidal artery also passes around the lateral side of the brainstem. E, enlarged view to show the increased length of basilar artery exposed by dividing the tentorium. F, an anterior petrosectomy has been completed. The petrous apex in the area behind the internal carotid artery and medial to the semicircular canals has been removed. The dural opening has been extended downward to expose the lateral edge of the clivus and the inferior petrosal sinus coursing along the petroclival fissure. The abducens nerve and the anteroinferior cerebellar artery are in the lower margin of the exposure. G, the angle of view has been changed to show the vertebral arteries in the lower margin of the exposure. The facial and vestibular nerves and the labyrinth and semicircular canals, which are to be avoided in the anterior petrosectomy approach, have been exposed to show their relationship to the approach. A., artery; A.Ch.A., anterior choroidal artery; A.I.C.A., anteroinferior cerebellar artery; Bas., basilar; Br., branch; Car., carotid; CN, cranial nerve; Fiss., fissure; Inf., inferior; M.C.A., middle cerebral artery; M.P.Ch.A., middle posterior choroidal artery; P.C.A., posterior cerebral artery; P.Co.A., posterior communicating artery; Ped., peduncle; Pet., petrosal, petrous; S.C.A., superior cerebellar artery; Semicirc., semicircular; Temp., temporal; Tent., tentorial; Vert., vertebral.

圖3.18。基底動脈上部動脈瘤的前顳下顯露術。A,問號形狀的頭皮切口(實線)和骨瓣位於顴骨上方。如果顴骨(孵化區)的上邊緣阻礙了沿中窩底部的低曝光通道,則用鑽頭將其移除。B,骨瓣被抬高以暴露硬腦膜開口的位置(斷線)。顳肌向前反射。可能需要在骨瓣下緣做一個小的顱骨切除術,同時切除顴骨上部,以使視野下降到中顱窩底部。C,顳葉被抬高以暴露基底動脈,丘腦操作,腦後,後交流,小腦上動脈,滑車和動眼神經,以及幕。顳肌向前反射。D,放大圖。 The thalamoperforating arteries course along the posterolateral margin of the neck of the aneurysm. A., arteries; B.A., basilar artery; M., muscle; P.C.A., posterior cerebral artery; P.Co.A., posterior communicating artery; S.C.A., superior cerebellar artery; Temp., temporal; Tent., tentorium; Th.Pe., thalamoperforating.
圖3.19。基部的頂端動脈瘤。優越的觀點。動脈瘤從基底動脈的頂端向上,丘腦操作動脈在管壁的後緣周圍伸展。左側交通動脈大小正常,既非發育不良也非胎兒型。右腦後動脈是一種胎兒型主要起源於頸內動脈。右側P1發育不良,左側P1大小正常。暴露的其他結構包括動眼神經和視神經、垂體柄、小腦上動脈和內側後脈絡膜動脈。B-F,丘腦動脈的起源模式。它們是基底尖動脈瘤區域最重要的穿孔分支。 B, most common pattern of origin. The thalamoperforating arteries are paired and arise from P1 segments, which are not hypoplastic. C, the perforating artery on the left is much larger than the one on the right. D, a single or dominant thalamoperforating artery arises from the hypoplastic right P1. The right posterior cerebral artery has a fetal configuration, arising predominately from the carotid artery. E, there are two thalamoperforating arteries on the left and a smaller one arising from the hypoplastic right P1. F, paired thalamoperforating arteries. The right one arises from a common trunk with the medial posterior choroidal artery. A., arteries; B.A., basilar artery; C.A., internal carotid artery; M.P.Ch.A., medial posterior choroidal artery; O.N., optic nerve; P.C.A., posterior cerebral artery; P.Co.A., posterior communicating artery; Pit., pituitary; S.C.A., superior cerebellar artery; Th.Pe., thalamoperforating.
位於小腦上動脈水平的基底動脈瘤通常發生在基底上動脈彎曲傾斜的地方,因此,沿基底動脈流動所產生的血流動力推力剛好位於小腦上動脈起點上方,而不是位於基底動脈頂端(圖3.15和3.16C)(4)。位於小腦前下動脈起點的動脈瘤通常起源於基底動脈曲線的凸側,並指向與動脈瘤緊鄰的基底段長軸方向(圖3.16D)(10)。
椎動脈上最常見的動脈瘤部位位於小腦後下動脈起源地。椎動脈通常被描述為筆直的;然而,如果存在動脈瘤,通常會發現椎動脈有一個向上凸的曲線,其頂端是小腦後下動脈的起點處(圖3.15和3.16F)(6)。動脈瘤起源於小腦後下動脈起點處的曲線頂端,並向上指向。
發生在兩個椎動脈與基底動脈交界處的罕見動脈瘤最初似乎很難符合這些規則。然而,當在多個血管造影投影中檢查時,它們通常被發現符合這些用於預測更常見的囊狀動脈瘤的位置和投射方向的相同解剖學原理。這些動脈瘤通常出現在椎基底關節交界處形成的彎曲曲線的凸側(圖3.15和3.16E)。一個椎動脈通常占主導地位,較小的椎動脈作為分支部位。如果這種彎曲的結構不存在,很可能動脈瘤與基底動脈下部的開窗有關。
以下的基本手術原則有助於指導顱內動脈瘤的治療。
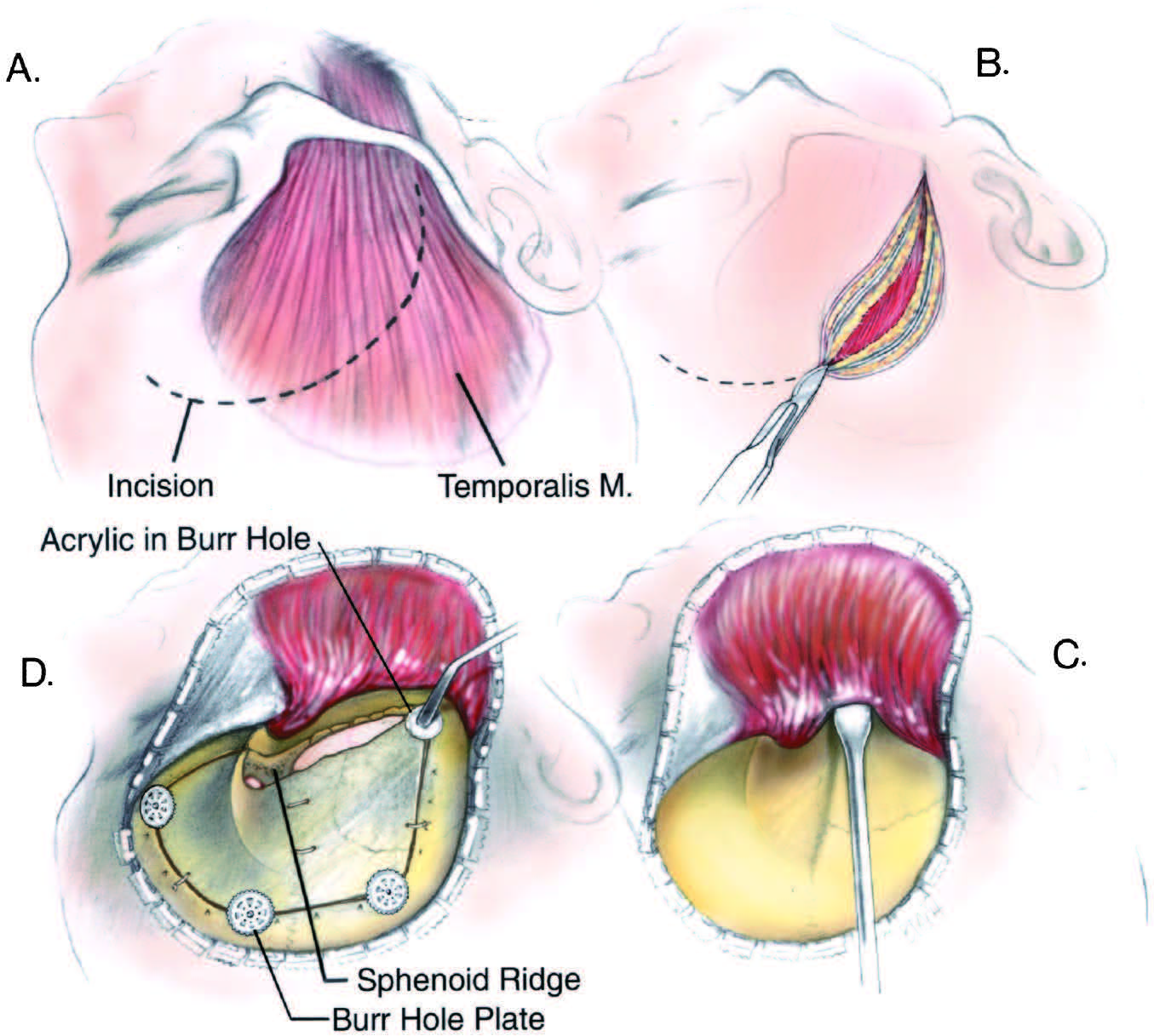
圖3.20。額顳開顱術用於暴露威利斯圓前部或後交通動脈水平以上的動脈瘤。a - c,頭皮和顳肌和筋膜被抬高為單層。D,當開顱手術皮瓣閉合時,可將軟丙烯酸樹脂模壓入毛刺孔,並允許在直視下硬化,以減少整形畸形,如果電鍍係統沒有覆蓋毛刺孔。米,肌肉。
圖3.21。額顳側開顱術的改進,以顯露眼動脈和垂體上動脈起源處的動脈瘤。如圖3.20所示,與將頭皮皮瓣翻轉為單層時相比,這種兩層頭皮開口提供了更低的暴露率和更容易獲得去除前床突和眶頂相鄰部分的方法。頭皮切口位置(實線)和骨瓣位置(斷線)。第一,麵神經的分支穿過顴骨到達前額的肌肉。B,包括盔瓣在內的頭皮,通過打開包骨膜和盔瓣之間的平麵向下反射。在包含麵神經分支的脂肪墊正上方切開顳肌筋膜(但不是顳肌),使脂肪墊和麵神經分支能隨頭皮皮瓣向下反射,從而減少損傷這些麵神經分支的可能性。C,頭皮瓣和顳肌被反射,露出鎖眼和翼點。沿著顳線的前部保留一個包膜和顳肌筋膜的袖套,以促進顳肌和筋膜的閉合。D,額顳骨瓣被抬高了蝶骨脊的外側部分被移除了。 The temporalis muscle and fascia are reflected into the posteroinferior margin of the exposure. E, the anterior clinoid process, roof of the optic canal, and adjacent part of the orbital roof and lesser wing of the sphenoid are commonly removed (hatched area) to access the internal carotid artery proximal to ophthalmic and superior hypophyseal aneurysms. C.A., internal carotid artery; O.N., optic nerve.
95%的動脈瘤出現在以下5個部位之一,所有這些部位都靠近Willis圓(圖3.1)。這些部位是1)頸內動脈之間的後交通和前脈絡膜動脈;2)前交通動脈區;3)大腦中動脈的初始分叉或三分叉;4)頸內動脈分叉;5)基底分岔。對於所有這些起源於Willis前圈的動脈瘤,以及一些起源於基底動脈上的動脈瘤,通常選擇額顳側開顱術進行輕微修改(21)。以翼點為中心的額顳皮瓣(翼點開顱術)可用於頸內動脈瘤(圖3.4、3.20和3.21)。對於大腦中動脈和頸內動脈分支的動脈瘤,皮瓣可在後上方擴大;對於前交通區,皮瓣可向前擴大;對於基底尖動脈瘤,皮瓣可在後上方提供翼前-顳前或前顳下入路。
這個皮瓣的頭皮切口從顴骨上方開始,穿過顳區向前延伸到發際線後的額區。打開頭皮進行額顳部暴露的方法不同,取決於動脈瘤的位置(圖3.20和3.21)。如果動脈瘤位於後交通動脈的水平或以上,則皮膚、盔瓣、周包膜、顳肌和筋膜反映為單層。如果動脈瘤位於眼動脈或垂體上動脈的水平,皮膚和盔瓣在一層被抬高,顳肌和筋膜在第二層被抬高。與單層皮瓣相比,雙層頭皮開口為切除前床突和眶頂鄰近部分提供了較低的曝光率和更好的通路。
一個小的,遊離的骨瓣,其基部的中心在翼點以下,被抬高。通過移除蝶骨脊,減少眶頂和側壁的厚度,使顱骨的開口向下方和內側延伸,形成一層薄薄的骨殼。準備這一皮瓣所需的時間,在這一皮瓣中,所有軟組織層都被反射在一起,比單獨分離和反射每一層所需的時間要短。由於麵神經分支到額肌的顳肌筋膜淺表層沒有受到幹擾,因此單層暴露可以減少額肌無力的發生率。減少了顳肌周圍的剝離,減少了限製張嘴的攣縮的發生,減少了由顳肌瘢痕和萎縮引起的美容畸形。任何會因整容畸形而愈合的鑽孔或顱骨切除部位都用顱骨成形材料或非磁性板封閉。顱骨成形術材料成型就位,並允許在直視下硬化,以確保硬化材料符合該區域的自然輪廓。
如果動脈瘤位於垂體上動脈或眼動脈的起源處,或者通過這種入路達到基底動脈尖的動脈瘤,則修改額顳頭皮皮瓣,使頭皮和盔瓣作為一層被抬高,顳肌和筋膜作為第二層被抬高(圖3.21)。這可以使顳肌反射到暴露的後下部分,並提供較低的暴露來去除前臥突、視神經管頂部和眼眶頂部的鄰近部分,這些通常是處理後交通動脈近端的動脈瘤所需要的。
顱底入路,如眶顴骨切開術、前岩切開術、乙狀竇前入路和遠側入路的各種改進,在動脈瘤的治療中被越來越多地使用,因為它們減少了大腦回縮的需要,增加了手術路徑的寬度,並擴大了夾層和夾板應用的角度。眶顴開顱術抬高眶上緣和眶外側緣及顴弓,可使頸動脈頸線上和威willis環上的所有動脈瘤暴露出來,但眼動脈瘤和垂體上動脈瘤的好處最大(圖3.7和3.22)。眶顴開顱術可與以下任何一種手術相結合:前臥位切除術和視神經管頂和眶尖切除治療眼和上垂體動脈瘤;海綿竇頂前臥位切除開口;後斜位切除(經海綿狀入路)或前路岩石切開術切除低窪的基底動脈尖或基底動脈瘤(圖3.7、3.17、3.22和3.23)。遠外側入路暴露椎動脈,使其在寰枕關節後方移動,越來越多地用於椎、椎基底動脈瘤和下基底幹動脈瘤(圖3.24和3.25)。對於位於後窩中央的動脈瘤,可以考慮采用不同程度的顳骨切除的乙狀竇前入路,盡管其中許多動脈瘤可以通過眶顴路、前岩石切開術或遠側入路的各種改進來達到(圖3.26和3.27)。眶顴入路的各種修正在本期第9章中進行了回顧,遠側入路和乙狀竇前入路在千年期中進行了回顧神經外科(16、17)。
翼狀骨瓣或眶顴骨瓣抬高並打開硬腦膜後,打開蛛網膜,通常從額下回三角部以下開始。可將毗鄰側裂前部的額葉抬高,使蝶骨脊暴露於前臥突的深度。進入海綿竇前部的側靜脈通常被保留(圖4.12)。在視神經和頸動脈周圍的池的蛛網膜壁被打開。如果動脈瘤起源於頸內動脈(圖3.3、圖3.4和圖3.7),外科醫生就處於所需的位置。切除前床突,拆除視神經管和眼眶頂的鄰近部分,切開延伸至視神經上方的硬腦膜鐮狀突,使視神經得以活動,可使頸眼動脈瘤和上垂體動脈瘤暴露。動脈瘤暴露的前臥位切除通常是在瘤內而不是在瘤外進行。
在接近後交通動脈瘤時,首先暴露頸動脈脊上肌的前或前外側表麵,然後暴露動脈瘤產生的後內側或後內側壁(圖3.8)。有人認為後交通動脈可以用動脈瘤頸夾住,特別是當動脈發育不良時(9)。然而,Willis環發育不良段與正常或大段產生相同數量和大小的穿孔分支。
由於脈絡膜前動脈的起源和流向較外側,因此在沿脊柱裂接近頸內動脈瘤時,它的起源和近端往往先於後交通動脈暴露出來。脈絡膜前動脈瘤通常在脈絡膜前動脈的後外側上方和內側突出,因此為夾子的安全應用提供了一個分離角度。頸部位於下、內側或下、內側。動脈瘤也可能起源於脈絡膜前動脈的多支血管,並使其分支在外側和內側移位。在頸動脈分叉處工作露出一部分頸部可能會有幫助。
前交流區最常由翼點入路進入,較少由額下、雙額或前半球間入路進入。對於前交通動脈瘤,翼點入路的夾層指向頸內動脈分叉上方,沿大腦前動脈越過視神經和交叉至動脈瘤頸部(圖3.4和3.12)。大部分動脈瘤指向前麵、下方和相對於主動脈瘤A1的一側。沿著翼點的入路有利於暴露眼底前的基底。有些外科醫生從右側入路所有前交通動脈瘤。作者選擇左側,如果左額血腫存在,如果動脈瘤底向右突出,或如果左大腦前動脈占優勢,而右側發育不良。控製占主導地位的大腦前動脈是很重要的,因為這些動脈瘤大多發生在一個A1占主導地位和另一個A1發育不良的情況下。如果動脈瘤暴露於交叉上方的蛛網膜下池,則不需要切除直回。如果需要切除A1s和A2s近端以及循環和前交通動脈,則應盡量減少。
在確定腦前動脈瘤頸部時,由於Heubner返動脈通常在A1段之前暴露(圖3.9和3.13)。額葉上方的第一個動脈可能是複發動脈。如果A1是發育不良的,那一側的再循環動脈可能和A1段一樣大甚至可能會和A1段混淆因為它可能和A1段有相同的路徑。返動脈可能位於A1段的任何方向,但如果沿著它走,通常在前交通動脈的遠端與A2段相連。複發動脈可能粘附在動脈瘤壁上。它可能向前循環或穿過直回,在切除直回後部時可能被阻塞,就像在直回入路中所做的那樣。A1的外膜可能掩蓋Heubner動脈,即使在顯微鏡下,夾子也很容易造成無意的閉塞。發育不良的A1s應該保留,因為即使它們很小,也可能產生穿孔分支。臨時夾應放置在A1段避開射孔分支的位置,因為大部分射孔分支都來自A1段的外側。在動脈瘤暴露不充分的部位放置夾會導致動脈瘤周圍穿孔小動脈閉塞,因此應避免。
大腦前動脈遠端動脈瘤位於中線或附近。應從非顯性右側通過冠狀縫線前方的單側額側開顱術,並根據需要延伸至中線,以獲得沿鐮的暴露而不過度回縮(圖3.14)。開顱術最好放置在足夠遠的前方,以便暴露胼胝體周動脈的近端,並在暴露過程中發生出血時暫時閉塞。顱切開術可以進行改進,以便在同一手術中也能切除第二個動脈瘤,這個動脈瘤比其他部位的動脈瘤更常發生。大腦前動脈的遠端部分由於位於半腦間裂很深而難以暴露。在其他位置,兩條大腦大動脈的主幹不像遠端大腦前動脈那樣並排運行,由於分支從一側到另一側的交叉,一條大腦前動脈的損傷可能導致對側大腦半球的梗死。一種不太令人滿意、難度較大的入路,僅適用於A2近端病變,是通過額葉抬高的翼點或額下開顱術,從頸動脈起源處向遠端延伸大腦前動脈。在縮回額葉內側表麵之前,可能需要犧牲一條從腦半球上緣到矢狀竇的橋靜脈。大多數情況下,隻需要犧牲一條靜脈。從這一點開始,手術通常是冗長的,因為半腦間裂提供的暴露有限,動脈瘤經常附著在鐮上,因為這個部位的動脈瘤在暴露過程中比其他幕上動脈瘤更容易破裂。
大腦前動脈遠端動脈瘤在破裂後發生腦出血的頻率略高於其他部位的動脈瘤,因為沒有蛛網膜下池供出血進入,且大腦表麵緊貼。出血可能進入大腦前動脈對麵的腦半球。明顯的血腫可能指示入路在血腫的一側。在解剖動脈瘤之前,應先確定胼胝體周圍動脈和胼胝體周圍動脈以及正常解剖結構的變異(圖2.22)。兩個大腦前動脈之間的連接可能發生在動脈瘤區域的近端或遠端,或者動脈瘤可能發生在單個胼胝體周動脈的頂端,這是由兩邊的胼胝體周動脈融合形成的單個動脈。遠端大腦前動脈動脈瘤頸通常較寬且呈動脈粥樣硬化狀。
大腦中動脈動脈瘤通過裂側裂顯露出來(圖3.4,3.9,3.10)。通常情況下,打開側裂並在額葉以下暴露的上部工作,將使近端M1段及其分叉後主幹在遇到動脈瘤頸部和動脈瘤底之前暴露出來。這些動脈瘤通常發生在靠近膝的M1分叉或三分叉處的紋狀動脈遠端,但它們也可能發生在M1段到額葉或顳葉早期分支的起源處。發生在早期分支部位的動脈瘤起源於與莢狀紋狀動脈相同的M1段。大莢狀紋狀動脈的起源處也可能出現動脈瘤。這些動脈瘤發源於膝(最常見的部位),向下、向前和側向,可能附著在蝶骨脊上,在這種情況下,手術入路可能需要修改,以避免在蝶骨脊處撕裂動脈瘤底。
顱底尖動脈瘤有幾種入路。它們可能通過翼點、顳前、顳前或顳下入路暴露。通過額顳(翼點)開顱可到達基底尖尖的四種路徑是:1)通過頸光三角,位於頸內動脈、視神經和大腦前動脈之間;2)下頸內動脈分叉與上視道之間;3)通過頸動脈與動眼神經之間的間隔,後交通動脈上方;4)頸內動脈與動眼神經之間及後交通動脈下方(圖3.4和3.28)。
如果視神經、頸動脈和A1之間的間隔足夠寬,動脈瘤向上方或前方突出(圖3.4和3.28),一些顱底尖動脈瘤可能通過頸動脈三角暴露出來。如果頸動脈和A1被拉長,三角變寬,如果這些動脈較短,三角變小。如果采用這種方法,應注意保護頸內動脈上的重要穿支,這些穿支穿過這個空間供應視神經、束和間腦。發生在高顱底分岔處的動脈瘤也可能通過下麵的頸內動脈分岔與上麵的視道之間的間隔暴露,通常是通過壓下分岔,但同樣,穿過這個間隔處的穿通動脈必須得到保護(圖3.4和3.28)。如果頸動脈脊上段較短,因此頸動脈分叉、視道下表麵和前穿孔物質之間有較寬的空間,則可采用這種方法。在翼點路徑中,動脈瘤通常通過頸內動脈和動眼神經之間的間隙進入(圖3.4和3.28)。這種暴露通過抬高頸動脈和近端M1段來促進。在暴露頸動脈和動眼神經之間的區域後,必須決定是否通過在後交通動脈上方或下方操作來暴露動脈瘤。如果基底動脈瘤起源於基底上動脈的後側,最好抬高顳葉,沿中窩底部接近該區域(圖3.4、3.17和3.18)。
大多數基底動脈動脈瘤通過前顳下入路進入(圖3.17和3.18)。如果將頭皮翼點切口和骨瓣向後延伸至耳前上方的問號切口,向下延伸至耳屏附近的顴弓,以便沿著中窩底部暴露,則顳下和顳下入路將變得容易。將顳肌和筋膜與頭皮分開,向前向下折疊顳肌,便於沿著中窩底暴露。抬高顳葉前部可使顳下前部顯露出來,同時可見動眼神經,因為它起源於腦梗內側表麵,穿過腦後動脈和小腦上動脈之間,進入海綿竇頂。抬高後交通動脈和顳葉暴露基底動脈尖,兩種動眼神經,以及右側後交通動脈與右側大腦後動脈的連接處。顳下入路結合小腦幕在滑車神經與小腦幕邊緣交界處後的切開,可觸及基底低分叉處或小腦上動脈起點處的動脈瘤。發生在小腦前下動脈起源地的動脈瘤,如果起源地位於基底動脈上部,也可以通過這條路進入(圖3.17)。
在顳下入路中,當腦後動脈內側彎曲時,沿著腦基底分叉處的動脈瘤頸最好能找到。P1下表麵是穿孔分支最不常見的起始部位,因此是通向大腦後動脈近端和基底分支最安全的入路(圖3.17和3.18)。位於Labbé靜脈前顳葉下的入路比沿著蝶骨脊的翼點入路能更好地暴露出通常來自基底動脈後部的穿通動脈。這些穿孔分支特別重要,因為它們供應控製意識的間腦區域。假設基底分叉動脈瘤和某些腫瘤的分支較少,大腦對它們的依賴程度也較低,則可考慮橫斷發育不良的後交通動脈或P1。然而,射孔分支的數量和直徑是相對恒定的,與主幹的大小無關。如果發育不良的部分被分割,應注意不要犧牲任何小的穿孔分支(20)。在結紮或放置夾在大腦後動脈時,必須避免從外側顳下路徑看不到其內側表麵的環狀小動脈。這些小的周動脈通常與大腦後動脈主幹合並在同一個蛛網膜束中,隻有將它們從主幹中分離出來才能保存下來。
顱底入路在顱底尖動脈瘤的治療中應用越來越頻繁。眶顴骨開顱術,去除眶頂、外側壁和顴弓,增加了暴露角度,無論入路是經眼、顳前、顳下前或顳下中(圖3.7和3.22)。另外兩種用於達到基底下分叉的改進方法是眶顴骨開顱聯合經海綿入路,其中前、後床突和海綿竇頂被切除(圖3.7和3.22)。經海綿入路的另一種選擇是前岩切入路,在打開硬腦膜之前,通過額顳或眶顴開顱術將頸岩動脈後和三叉神經下的岩尖部分在硬腦膜外切除(圖3.17和3.23)。鑽孔完成後,打開硬腦膜,拉開幕。暴露可使三叉神經受到抑製,因此與未進行岩石切開術的幕部切開術相比,暴露的基底動脈長度顯著增加。
如果動脈瘤和連接處在後窩位置較高,則通過顳下幕前暴露術接近椎基底交界處的動脈瘤;如果連接處在後窩中部較深,則通過幕上和幕下乙狀竇前聯合暴露術接近動脈瘤;如果椎基底交界處較低,則通過外側枕下或遠外側入路接近動脈瘤(圖3.16E和3.24-3.27)。起源於小腦後下動脈起點的椎體動脈瘤,如果位於後顱窩較低,則采用外側枕下開顱術或遠外側入路,如果位於後顱窩中部較深,則采用幕上和幕下乙狀竇前聯合顯露術(圖3.16F和3.24 - 3.27)。如果選擇遠外側枕下入路,可以切除C1後弓同側的一半,以充分暴露動脈瘤近端的椎動脈段。隻有在仔細檢查血管造影後,才應選擇枕下入路的一側,因為由於椎動脈的極度彎曲,一個椎動脈的動脈瘤可能位於腦幹的另一側,與椎動脈充盈的一側相對。
圖3.22。眶顴經海綿入路治療基底尖動脈瘤。A,顱眶顴骨截骨術的頭部位置和部位。第一塊是翼點骨瓣(紅色),第二塊是眶顴截骨片(綠色)。兩片式方法比兩種截骨術中包括的骨作為整體抬高時,可以保留更多的眶頂。B,骨切除(紅色凸起區域)可包括蝶骨脊(1)、前臥突(2)和後臥突以及相鄰鞍背(3)。C,手術暴露下基底尖動脈瘤。暴露在頸動脈和動眼神經之間。後交通動脈被抬高了。動脈瘤頸位於鞍背和後床突的後麵。D,側突前被切除露出頸內動脈的側突段和海綿竇的頂部。 The dura of the roof has been opened back to the level of the posterior clinoid process, and the posterior clinoid and adjacent part of the dorsum have been removed to expose the basilar artery below the neck of the aneurysm. A., artery; A.C.A., anterior cerebral artery; Ant., anterior; Bas., basilar; Car., carotid; Cav., cavernous; Clin., clinoid; M.C.A., middle cerebral artery; N., nerve; P.C.A., posterior cerebral artery; P.Co.A., posterior communicating artery; Post., posterior; S.C.A., superior cerebellar artery; Seg., segment.
圖3.23。前路岩石切開術治療下基底分叉動脈瘤。A,抬高問號形頭皮皮瓣(實線)。一個向下延伸到中窩底的骨瓣被抬高(虛線內的陰影區域)。切除皮瓣下緣和顴弓上緣的部分骨,以增加沿中窩底的通路。B,基底下分叉動脈瘤的圖示和前路岩石切開術切除骨的位置。岩尖的前部在頸內動脈岩段後麵在內聽道前麵和耳蝸內側被切除。在骨瓣的下緣切除骨,包括顴弓的上部(孵化區),以增加對中窩底的接觸。C,顳葉被抬高了。幕部切口從滑車神經入口後的內側邊緣延伸至幕部邊緣(折線)。 The dural incision extends forward into the area of the anterior petrosectomy. The P1s and posterior communicating artery and the oculomotor and trochlear nerves are exposed at the medial margin of the tentorial edge. D, the dura has been opened and the trigeminal nerve has been depressed to expose an aneurysm on the low basilar bifurcation. A., artery; Bas., basilar; Car., carotid; CN, cranial nerve; P.C.A., posterior cerebral artery; P.Co.A., posterior communicating artery; Pet., petrous; S.C.A., superior cerebellar artery; Temp., temporal; Tent., tentorial.
圖3.24。遠側的方法。A、程序如圖所示為直立位置;然而,手術通常是在四分之三俯臥位進行。插圖顯示頭皮切口(實線)和骨開口(陰影區)的位置。所有的枕下肌肉,除了那些與枕下三角相鄰的肌肉,都是向下折疊成一層,帶有頭皮皮瓣。椎動脈位於枕寰關節後枕下三角深處,位於上、下斜肌和頭直肌後大肌之間。第二,枕骨髁的後部被切除了。如圖所示,硬腦膜打開。C,椎動脈和小腦後下動脈從椎動脈的低起點。 The aneurysm projects between the posteroinferior cerebellar artery and the vertebral artery and in front of the brainstem. The glossopharyngeal, vagus, accessory, and hypophyseal nerves are in the exposure. D, posteroinferior cerebellar artery vertebral aneurysm for which a far lateral approach would be considered. A., artery; A.I.C.A., anteroinferior cerebellar artery; B.A., basilar artery; Lig., ligament; Inf., inferior; M., muscle; Occip., occipital; P.C.A., posterior cerebral artery; P.I.C.A., posteroinferior cerebellar artery; Post., posterior; S.C.A., superior cerebellar artery; Sp., spinal; Suboccip., suboccipital; Sup., superior; Trans., transverse; Vert., vertebral.

點擊這裏查看此圖像的交互模塊和相關內容。
圖3.25。遠外側和經髁入路。A,枕骨髁和枕骨大孔的下視圖。枕髁是位於枕骨大孔前半部分外側邊緣的卵形結構。舌下管,探頭通過,位於枕髁中部三分之一以上,從後到前,從內側到外側。舌下管的顱內端位於枕髁後三分之一與中三分之一交界處上方約5mm處,距後髁邊緣約8mm處。髓管顱外端位於髁狀突前三分之一和中三分之一交界處上方約5mm處。遠外側入路通過髁突後麵的區域,經髁入路需要切除部分髁突。大箭頭顯示的是經髁入路的方向,而凸起的區域顯示的是枕骨髁的一部分,可以在不暴露舌下管內舌下神經的情況下切除。B,右側。 A suboccipital craniectomy has been completed and the right half of the posterior arch and the posterior root of the transverse foramen of the atlas have been removed. The vertebral artery passes medially behind the atlanto-occipital joint. A posterior condylar vein passes through the occipital condyle. C, the drilling in the supracondylar area exposes the hypoglossal nerve in the hypoglossal canal and can be extended extradurally to the level of the jugular tubercle to increase access to the front of the brainstem. The dura has been opened. The dural incision completely encircles the vertebral artery, leaving a narrow dural cuff on the artery so that the artery can be mobilized. D, comparison of the exposure with the far lateral and transcondylar approaches. On the right side, the far lateral exposure has been extended to the posterior margins of the atlantal and occipital condyles and the atlanto-occipital joint. The prominence of the condyles limits the exposure along the anterolateral margin of the foramen magnum. On the left side, a transcondylar exposure has been completed by removing the posterior part of the condyles. The dura can be reflected further laterally with the transcondylar approach than with the far lateral approach. The condylar drilling provides an increased angle of view and room for exposure and dissection. The dentate ligament and accessory nerve ascend from the region of the foramen magnum. A., artery; Atl.Occip., atlanto-occipital; Car., carotid; CN, cranial nerve; Cond., condylar, condyle; Dent., dentate; For., foramen; Hypogl., hypoglossal; Jug., jugular; Lig., ligament; N., nerve; Occip., occipital; P.I.C.A., posteroinferior cerebellar artery; Post., posterior; Proc., process; Stylomast., stylomastoid; Trans., transverse; V., vein; Vert., vertebral.
圖3.26。幕上和幕下乙狀竇前聯合入路至基底動脈。A,頭皮切口位置(實線)和去骨位置(斷線)。B,動脈瘤的類型,可以考慮這種方法。C,顳上和顳下區域已經暴露。乳突切除術已經完成,小心保存耳膜和半規管上的骨頭。硬腦膜在乙狀竇前打開。硬腦膜切口穿過岩上竇和幕邊緣,注意保護滑車神經。這提供了進入椎動脈上部和基底動脈全長的通道。這種入路可用於小腦前下動脈起源處的基底動脈或椎動脈與基底動脈交界處的動脈瘤。 This approach may also be selected for vertebral aneurysms arising at the origin of the posteroinferior cerebellar artery if the aneurysm is located high and deep in the posterior fossa. The jugular bulb may block access to the lower part of the intracranial part of the vertebral artery. Care is taken to preserve the vein of Labbé as the temporal lobe is elevated. Other structures in the exposure include the oculomotor, trigeminal, abducens, facial, vestibulocochlear, glossopharyngeal, and vagus nerves and the superior cerebellar artery. A.I.C.A., anteroinferior cerebellar artery; B.A., basilar artery; Jug., jugular; P.C.A., posterior cerebral artery; P.I.C.A., posteroinferior cerebellar artery; S.C.A., superior cerebellar artery; Sig., sigmoid; Sup., superior; Temp., temporal; Tent., tentorium; V., vein; V.A., vertebral artery.

點擊這裏查看此圖像的交互模塊和相關內容。
圖3.27。幕上和幕下乙狀竇前聯合入路。A,插圖顯示了右側顳枕顱開顱術和乳突暴露。乳突切除術已經完成,由迷宮周圍密集的皮質骨組成的耳膜已經暴露出來。麵神經的鼓膜段和外側管位於亨利脊柱的深處。特勞特曼三角,乙狀竇前的硬腦膜塊,麵對著橋小腦角。B,打開乙狀竇前硬腦膜,分離岩上竇和幕狀肌,注意保留連接橫竇的Labbé靜脈和進入幕狀肌前緣的滑車神經。外展神經和麵神經向前庭耳蝸神經內側暴露。小腦後下動脈與舌咽神經和迷走神經在暴露的下緣。小腦上動脈在動眼神經和滑車神經下麵,在三叉神經上麵。 C, the labyrinthectomy has been completed to expose the internal acoustic meatus. A marginal branch of the superior cerebellar artery loops downward on the cerebellum. D, the dura lining the meatus has been opened and the facial nerve has been transposed posteriorly. The cochlear nerve has been divided and bone removed to expose and remove the cochlea. The transcochlear exposure, completed by removing the cochlea and surrounding petrous apex, provides access to the front of the brainstem and vertebrobasilar junction, but at the cost of loss of hearing caused by the labyrinthectomy and almost certain temporary or permanent facial weakness associated with the transposition of the facial nerve. A., artery; Ac., acoustic; A.I.C.A., anteroinferior cerebellar artery; Bas., basilar; Br., branch; Chor., chorda; CN, cranial nerve; Inf., inferior; Int., internal; Jug., jugular; Marg., marginal; N., nerve; P.I.C.A., posteroinferior cerebellar artery; Pet., petrosal; S.C.A., superior cerebellar artery; Sig., sigmoid; Sp., spine; Sup., superior; Tymp., tympani; V., vein; Vert., vertebral; Vert.-Bas., vertebrobasilar.
圖3.28。四種手術路徑通過額顳開顱術直達基底尖動脈瘤。A,額顳開顱部位(左上)。側裂露出頸動脈、大腦前動脈和中動脈、視神經和動眼神經以及前臥突(右下)。B,基底尖通過頸光三角暴露出來,位於頸動脈,視神經和大腦前動脈之間。如果頸內動脈和大腦前動脈的起始段較長,可以使用這種方法,從而通過這個三角形空間提供一個寬闊的開口。其他暴露的結構包括顱底,後腦,後通信,丘腦操作,小腦上,循環動脈,嗅覺和視道。P1從基底動脈延伸到與後交通動脈的交界處。頸動脈和後交通動脈的穿支可能會形成障礙,因此在四種入路中都應保留。C,通過頸動脈分叉和視神經束之間的間隔進入。 This approach may be used if the carotid artery is short, thus providing an opening between the bifurcation and the optic tract. The perforating branches arising in the region of the bifurcation of the carotid artery may limit access through this area. D, approach directed behind the carotid artery and above the posterior communicating artery, through the interval between the carotid artery and oculomotor nerve. The perforating branches of the posterior communicating artery may need to be separated to reach the basilar apex. E, approach directed below the posterior communicating artery, through the interval between the carotid artery and oculomotor nerve. The posterior communicating artery has been elevated with a small dissector. A., arteries, artery; A.C.A., anterior cerebral artery; Ant., anterior; Bas., basilar; Car., carotid; Chor., choroidal; Comm., communicating; M.C.A., middle cerebral artery; N., nerve; Olf., olfactory; P.C.A., posterior cerebral artery; Post., posterior; Rec., recurrent; S.C.A., superior cerebellar artery; Th.Perf., thalamoperforating; Tr., tract.
貢獻者:Albert L. Rhoton, Jr, MD
內容來自Rhoton AL, Jr.幕上顱空間:顯微外科解剖和外科入路。神經外科2002年,51:S1-iii-S1-vi。doi.org/10.1097/00006123 - 200210001 - 00001.經牛津大學出版社代表神經外科醫師協會批準。©神經外科醫生協會。
神經外科188bet手机app圖譜很榮幸能夠繼承Albert L. Rhoton, Jr . MD的遺產。
請登錄發表評論。
一定要在社交媒體上關注我們,獲取精彩內容並保持更新生活科恩醫生的會議,關於手術技術的問題,以及更多!



您必須登錄才能查看此材料。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
現在請捐!
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。請承諾每年至少捐贈250美元給Atlas。
如果沒有這個承諾,Atlas將很快需要付費訂閱世界上許多病人的護理都依賴於它的外科醫生將無法使用它。現在請捐!