

你可以有所作為。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
現在請捐!
最後更新:2021年7月13日
背景為上、中、下斜坡的相關部位精心定製經行入路,需要對斜坡的病灶關係有精確的理解。
客觀的製定上、中、下斜坡的最佳分類,並定義每個斜坡層麵的顱外和顱內關係。
方法使用手術顯微鏡和內窺鏡對10具屍體頭部和10具幹顱骨進行解剖
結果斜坡被兩個顱內標誌分為上、中、下三分之一:外展神經的硬腦膜孔和舌咽神經的硬腦膜壁。在經鼻入路中暴露的有用的外科標記有助於定位斜坡分區的交界處是內頸動脈的臨骨段的下限,位於維管後開口上方4.9毫米處,以及咽結節。上、中、下斜坡入路可到達前麵描述的後窩上、中、下神經血管複合體的前中線部分。鼻和鼻咽之間的關係在擴大經鼻入路到斜坡邊界的重要回顧。
結論經口入路可以精心定製,以暴露後窩前部的局灶性病變。

後顱窩的前中線區域,包括斜坡和腦幹前表麵,是最難進入的區域之一。多種顯微外科入路,如額下經基底、顳下前經岩(Kawase)、乙狀竇前、乙狀竇後和遠側入路,可限製進入該區域,但有明顯的缺點。1 - 6這些缺點包括廣泛切除顱底結構,需要大腦回縮以達到深中線的神經血管結構,以及通過外側和後外側入路提供的中線結構的有限視野。1 - 6
經鼻經內窺鏡入路進入後窩克服了這些缺點。7 - 14它為中線結構提供了一條直接路徑,並允許在不收縮大腦的情況下觀察它們。該入路通過鑽穿整個或部分斜坡,可獲得腦幹前表麵的全景。然而,大開的斜坡和斜坡硬腦膜增加腦脊液(CSF)泄漏的風險。最近的一個手術係列有很高的發生率(33%)術後腦脊液漏。10
根據病灶位置,精心定製斜坡開口是減少腦脊液泄漏的合理方法。15斜坡通常分為上、中、下三部分,以方便病灶入路。這種斜坡的分類很大程度上是基於經鼻入路暴露的顱外標誌。然而,一個精確的經鼻入路到顱內結構需要徹底了解顱外和顱內結構之間的關係。在這項研究中,我們專注於斜坡和鄰近的腦池和腦幹的顱內外關係的顯微外科和內窺鏡解剖。本研究的目的是細化上、中、下斜坡的分類,並探索每個斜坡分區經鼻經入路的外科解剖。16 - 22

圖1所示。斜坡的顱內表麵與後顱底相鄰部分的骨關係。A,後顱窩上方視圖。顱底被分離成獨立的骨頭,同時保持骨頭之間的關係。顱後窩由枕骨、蝶骨和顳骨組成,顱斜由蝶骨和枕骨組成。B,蝶骨上方。鞍背下方的區域形成了斜坡的上三分之一。舌突是頸動脈岩狀韌帶的附著部位,位於頸動脈岩狀和海綿狀部分的交界處。C,枕骨上方。基底(斜坡)部分形成了斜坡的下三分之二。 The paired condylar parts are situated along the anterolateral margin of the foramen magnum and connect the clival and squamosal parts of the occipital bone. D, posterior superior view. The petroclival fissure, which extends from the foramen lacerum above to the jugular foramen below, is positioned between the clivus and the petrous part of the temporal bone. The petrous apex articulates with the clivus near the junction with the sphenoid and occipital bones. E, enlarged posterior superior view of the left jugular foramen and the adjacent area. The jugular tubercle projects into the posterior fossa just above the hypoglossal canal. The jugular foramen is a sutural foramen located between the temporal and occipital bones. The sigmoid part, the larger lateral part of the jugular foramen, receives the drainage of the sigmoid sinus, and the petrosal part, the smaller medial part, receives the drainage of the inferior petrosal sinus. Cranial nerves IX, X, and XI exit the skull between the sigmoid and petrosal parts of the foramen. F, posterior superior view of a right jugular foramen. The intrajugular processes, the bony prominences that protrude into the jugular foramen from the temporal and occipital bones, are joined by a fibrous or osseus bridge that separates the jugular foramen into petrosal and sigmoid parts. The intrajugular process of the occipital bone is usually smaller than the process on the temporal bone. There is a small bony notch for the glossopharyngeal nerve at the upper border of the jugular foramen. In life, this notch corresponds to the site of the dural glossopharyngeal meatus, where the glossopharyngeal nerve penetrates the dura. The cochlear aqueduct opens into the upper margin of the petrosal part below the glossopharyngeal notch. Ac., acoustic; Coch., cochlear; Cond., condyle; Fiss., fissure; For., foramen; Glossophar., glossopharyngeal; Gr., greater; Hypogl., hypoglossal; Int., internal; Intrajug., intrajugular; Jug., jugular; Less., lesser; N., nerve; Occip., occipital; Pet., petrosal, petrous; Petrocliv., petroclival; Proc., process; Sig., sigmoid; Sphen., sphenoid; Temp., temporal; Tuberc., tubercle; Vestib., vestibular.
本研究使用了10個血管注射彩色矽膠的屍體標本和10個幹頭骨。使用圖像引導(隱身站,Medtronic Sofamor Danek)在垂直於硬齶的冠狀麵對一些標本進行切片,以便於聚焦入路每個階段遇到的結構。使用手術顯微鏡(Carl Zeiss Corp, Oberkochen, Germany)和直徑為4毫米的剛性0°、45°和70°內窺鏡(Karl Storz Co, Tuttlingen, Germany)完成解剖。解剖由上至下,最後至中斜坡區。每個區域先是單側暴露,然後是雙側暴露。
斜坡由蝶骨和枕骨組成,由一個從枕骨大孔前緣向上和向前傾斜的寬而淺的凹槽組成(圖1)。蝶骨形成斜坡的上三分之一,它對應於鞍背後麵和下麵的一個傾斜區域。它繼續不間斷地融入枕骨的基底(斜坡)部分,形成了大部分的斜坡。這兩塊骨頭在蝶枕軟骨聯合處鞍背下方連接,在青春期閉合,成人不可見。23岩斜坡裂隙和頸靜脈孔位於顳骨岩部與相鄰的斜部和枕骨髁部之間,位於斜部的外側邊緣(圖1)。岩下竇沿岩斜坡裂隙的顱內表麵前進。成對的枕骨髁,從枕骨的髁部向下突出,位於枕骨大孔的前外側邊緣。在髁突的顱內表麵,有一個橢圓形隆起,頸靜脈結節,位於舌下管的上方,位於岩斜裂隙下部的內側。
外展神經硬腦膜孔和舌咽口是斜坡顱麵的標誌,將斜坡分為三部分。
外展神經從橋髓溝的內側伸出後,向上和側向穿過位於岩尖上邊緣下方的硬腦膜孔(圖2)。岩尖上邊緣和外展硬腦膜孔之間的平均垂直距離為3.4 mm。刺穿硬腦膜後,外展神經進入Dorello 's管,這是一個狹窄的三角形硬腦膜間隙,由岩蝶骨韌帶(或Gruber 's)上、岩尖下外側和斜下內側為界。24日,25神經位於格魯伯韌帶的下方,格魯伯韌帶從鞍背外側緣的下部延伸到岩尖的上緣。神經周圍的管管內充滿了在海綿竇、基底竇、岩上竇和岩下竇交界處的靜脈彙合。24外展神經在Dorello 's管中向上延伸,到達岩石斜坡裂隙的上端,在那裏進入海綿竇,並繞著頸動脈海綿竇的近端向外側轉彎。
三叉神經通過硬腦膜三叉神經孔出後窩,位於外展硬腦膜神經孔的上外側和幕狀附件的下方,進入Meckel 's洞,位於顳骨岩部上表麵的三叉神經印痕中。
硬腦膜頂頸靜脈孔有兩個穿孔:舌咽神經通過的舌咽口和迷走神經和副神經通過的迷走神經口(圖2)。兩者都位於顳骨和枕骨頸內突的內側,這是從頸靜脈前緣和後緣突出到頸靜脈孔的骨突起,並將頸靜脈孔分為岩狀和乙狀結腸部分(圖1F和2E)。26舌咽口位於迷走神經口的上方。舌咽口位於頸靜脈孔岩部的上緣,在那裏有一個小的骨刻口,舌咽神經沿著它向下延伸,耳蝸導水管進入其中。穿過硬腦膜後,神經與迷走神經和副神經一起進入頸內硬腦膜腔室(在椎間孔的岩狀部和乙狀結腸部之間),但向下穿過頸靜脈孔,與迷走神經和副神經分離。26日,27日最後,舌咽神經沿著頸內靜脈的前壁離開頸靜脈孔,而迷走神經和副神經則沿著靜脈的內側壁離開。
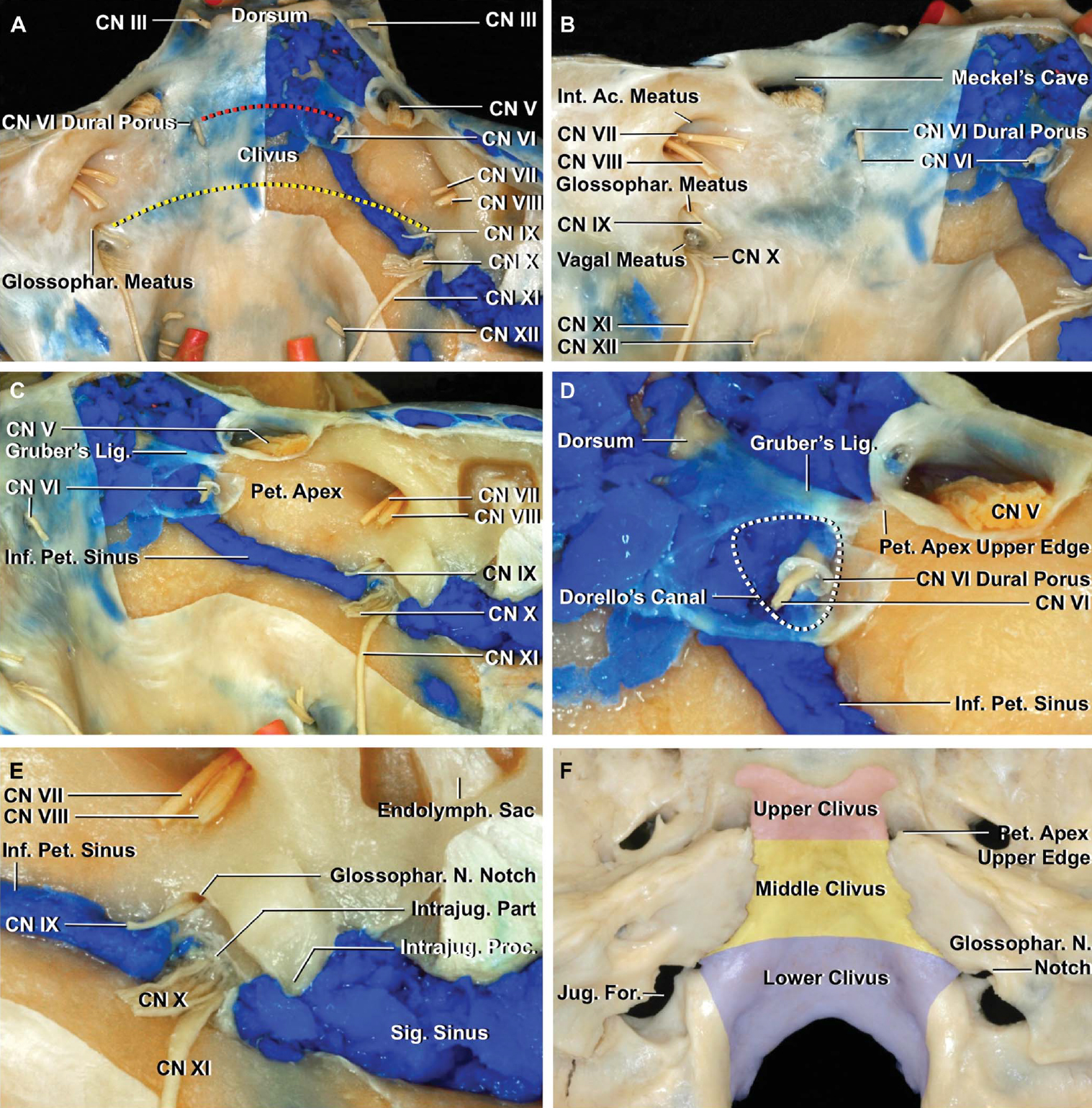
圖2。骨、硬腦膜和顱神經(CN)的關係。A,後上觀。在保留中樞神經的同時切除後窩右半部分的硬腦膜。CNs V至XII穿透硬腦膜後窩。上斜坡和中斜坡在外展神經硬腦膜孔的軸向麵分開,形成外展神經穿過硬腦膜的地方。中斜坡和下斜坡由舌咽部硬膜軸麵分開,舌咽部神經通過它進入頸靜脈孔。紅色虛線表示上、中斜坡的分界,黃色虛線表示中、下斜坡的分界。上斜坡後麵的硬膜內空間包括第三中樞神經和第五中樞神經;中斜坡後麵包括第六、第七和第八中樞; and behind the lower clivus includes CNs IX, X, XI, and XII. B, posterior oblique view, left side. Meckel’s cave, through which the trigeminal nerve passes, is located superolateral to the dural porus of the abducens nerve. The dura over the jugular foramen has 2 perforations: a glossopharyngeal meatus through which the glossopharyngeal nerve passes and a vagal meatus through which the vagus and accessory nerves pass. The glossopharyngeal meatus is located superior to the vagal meatus. C, posterior oblique view after removing the dura on the right side. The inferior petrosal sinus courses along the intracranial surface of the petroclival fissure. D, enlarged view focusing on the dural porus of the abducens nerve and Dorello’s canal. Gruber’s ligament extends from the lower part of the lateral edge of the dorsum sellae to the upper edge of the petrous apex. Dorello’s canal (white dotted line) is a narrow, interdural, triangular space bounded by Gruber’s ligament superiorly, the petrous apex inferolaterally, and the clivus inferomedially. After piercing the dura, the abducens nerve courses beneath Gruber’s ligament and through a large venous confluence at the junction of the cavernous, basilar, and the superior and inferior petrosal sinuses. The dural porus of the abducens nerve is located just below the upper edge of the petrosal apex. E, enlarged view focusing on the jugular foramen. The glossopharyngeal, vagus, and accessory nerves enter the intrajugular part of the jugular foramen, which is located between the petrosal and sigmoid parts. The glossopharyngeal nerve, after reaching the bony notch at the upper border of the jugular foramen, courses downward through the jugular foramen separate from the vagus and accessory nerve. F, the demarcation between the upper and middle clivus corresponds to the level 3.4 mm below the upper edge of the petrous apex. The demarcation between the middle and lower clivus corresponds to the level of the notch for the glossopharyngeal nerve at the upper medial edge of the jugular foramen. Ac., acoustic; Endolymph., endolymphatic; For., foramen; Glossophar., glossopharyngeal; Inf., inferior; Int., internal; Intrajug., intrajugular; Jug., jugular; Lig., ligament; N., nerve; Pet., petrosal, petrous; Proc., process; Sig., sigmoid.
上斜坡位於鞍背和外展神經硬腦膜孔之間,下斜坡位於舌咽部水平和枕骨大孔前緣之間,中斜坡位於上斜坡和下斜坡之間(圖2A和2F)。21後臥突與外展神經硬腦膜孔之間的距離平均為13.2 mm(範圍為12-17 mm);外展神經孔與舌咽口之間,21.4 mm(範圍19-24 mm);在舌咽口和舌下神經硬腦膜孔之間,25.4 mm(範圍,23-30 mm)。相對於骨結構,上斜坡與中斜坡的界線對應於岩尖上緣以下3.4 mm(範圍1.5-6.0 mm),中斜坡與下斜坡的界線對應於頸靜脈孔上緣內側的舌咽神經切跡的水平(圖2F)。
通過鼻腔觀察,斜坡從一側到另一側凸出,向下和向後向枕骨大孔傾斜。它主要是由枕骨斜坡部分的顱外表麵形成的(圖3)。蝶骨體的下表麵位於枕骨斜坡部分的前方,提供了犁骨附著的位置。犁骨的上緣擴展成成對的翼狀,與蝶骨的下表麵相貼合。每個翼翼的外側邊緣延伸到一個薄骨片,陰道突,從翼翼內側板的根部向內側伸出。在犁鼻翼和陰道突之間有一個小管,叫犁陰道管。陰道突的下表麵有一個前後槽它被轉換成一個管,齶陰道管,由齶骨蝶突的上表麵標記。這條齶陰道管通過翼齶窩後壁的內側向前打開並傳遞翼齶神經節的咽支和一個來自上頜動脈的小咽支。犁陰道管位於齶陰道管的內側,並向前延伸至齶陰道管的前端。
岩斜坡裂縫位於斜坡的外側邊緣,將枕骨和顳骨的岩部分開(圖3B)。岩斜裂縫在顱外形成比顱內表麵更深的裂縫,充滿了軟骨,這是原始軟骨的殘餘。這個裂縫從上麵的裂孔延伸到下麵的頸靜脈孔。撕裂孔位於蝶骨、顳骨和枕骨的連接處。撕裂孔的前部與身體、大翼和蝶骨翼突的根部相連,後外側與顳骨岩部的尖部相連,內側與枕骨的斜坡部相連。頸內動脈在出岩尖後,占據了淚孔的上部。維管的後端,傳遞維管動脈和神經,開口進入前外側邊緣的上部至裂孔孔是頸動脈交感神經叢的岩深神經與岩大神經連接形成維神經的地方。
從前麵沿著硬齶軸看,骨顱底的外側部分大部分被上頜骨隱藏(圖3C和3E)。然而,枕骨的斜坡部分可以通過鼻腔的下部和稱為後鼻孔的後鼻孔看到,通過後鼻孔,鼻腔進入鼻咽。斜坡,從下到上,大約向前傾斜45度。蝶竇也可通過鼻腔上部進入。因此,整個斜坡可以通過鼻腔進入,因為蝶竇的後壁形成了斜坡的上部。硬齶位於枕骨大孔的軸位。為了獲得一些斜坡病變所需的擴大鼻腔通道,需要了解沿鼻走廊到斜坡的關係(圖3和圖4)。
Wang等人很好地描述了蝶竇的解剖學和一種新的分類。29蝶竇前壁由兩個區域組成。上部和外側區域與後篩竇細胞共享其壁,從鼻腔無法看到(圖3L)。內側較低的平滑三角形區域稱為蝶骨甲殼,形成了蝶前麵的大部分,可以從上鼻甲後麵的鼻腔看到。蝶竇口位於蝶甲上角外側緣附近和上鼻甲後下端內側略上方(圖4G)。中位麵的前壁有一個脊,蝶脊,它形成了鼻中隔的一小部分。這個脊的前邊界與篩骨的垂直板相連。
蝶竇後壁位於鞍區上方,外側受頸動脈突起的限製,頸動脈的海綿狀部分位於頸動脈的後麵(圖4I、4J和4L)。由於後竇壁對應於位於鞍背和枕骨基底部之間的斜坡部分(圖4L和5),因此頸動脈的這一垂直段也被稱為“膝前段”。當頸動脈向遠端延伸時,頸動脈從頸動脈管中退出,並向上和向內側轉向,在淚孔上方形成“前膝”。前膝也被稱為淚孔段,因為它與淚孔的關係。頸動脈從屈點開始並向上延伸,在屈點處,動脈在淚段遠端垂直轉向(圖4L和5)。28日,30竇常向後延伸,超出垂體窩後壁的垂直冠狀麵,形成斜坡隱窩,Wang等人檢查的竇中有68%存在。29這個隱窩可以向上延伸到鞍背和/或枕骨基底部。
成對的維管位於蝶竇骨底,也可伸入蝶竇,特別是伸入通氣良好的竇前部(圖4K)。根據Osawa等人的研究,2860%的鼻竇可見骨突出物覆蓋在蝶竇底維甸管上。
向前觀察枕骨斜坡部分的顱外表麵,可以在中線處看到一個小凸起,即咽結節(圖3)。咽結節與咽中縫相連,上收縮肌插入咽中縫。本研究中所有20例標本均可見咽部結節。它位於犁骨後緣後17.4 mm和枕骨大孔前緣前10.8 mm處。頭長肌附著在咽結節側麵的斜坡上。頭前直肌是位於頭長肌深處的一塊小肌肉,附著在上麵一個小凹處,即髁上溝,位於枕骨髁上方和寰椎側塊下方。頭直肌前附著的凹槽位於枕骨大孔前緣上方平均9.0毫米處,可被稱為髁前結節的小突起所取代。20日,31日32髁上溝為估計舌下管及其外孔的位置提供了可靠的標誌。舌下管位於牙槽深處。舌下管的顱外孔和頸靜脈孔位於骨溝的外側。枕骨枕骨大孔的前緣與寰枕前膜相連。
枕骨的成對髁狀部分位於枕骨大孔的兩側。枕骨髁與寰椎相連,位於枕骨大孔前半部分外側,呈橢圓形,向下凸,麵朝下和側向,其長軸向前和向內側。位於每個髁內側的齒狀突鼻翼韌帶上的結節。舌下管位於髁突前後軸的中間三分之一以上,並從其顱內開口向前和側向。

圖3。a -。斜坡的顱外表麵與鄰近顱底的骨關係。劣質的視圖。枕骨斜部顱外表麵左右凸,表麵不規則。在枕骨大孔處,上麵比下麵寬。B,放大圖。岩斜坡裂隙將斜坡的側緣與顳骨的岩部分開。這個裂縫從上麵的裂孔延伸到下麵的頸靜脈孔。在蝶骨陰道突的下表麵有一個前後槽。 This groove joins with the upper surface of the sphenoidal process of the palatine bone to form the palatovaginal canal, which opens anteriorly into the pterygopalatine fossa. An inconsistent vomerovaginal canal may lie medial to the palatovaginal canal between the ala of the vomer and the vaginal process of the sphenoid. C, anterior view. The middle and inferior conchae have been removed. The clival part of the occipital bone is seen through the lower part of the nasal cavity and the posterior nasal apertures (choanae), the opening between the nasal cavity and nasopharynx bounded below by the horizontal plate of the palatine bone, superiorly by the body of the sphenoid, and laterally by the medial pterygoid plates. The sphenoid sinus occupies the upper part of the view through the nasal cavity. The hard palate is positioned at the level of the foramen magnum posteriorly. The lateral part of the cranial base is hidden behind the maxillae. D, anterior view. The sphenoid, ethmoid, and both palatine bones have been fitted together. The ethmoid bone forms the roof of the nasal cavity in front of the sphenoid bone. The middle nasal conchae are parts of the ethmoid bone, whereas the inferior nasal concha is a separate bone. The posterior end of the middle conchae articulates with the ethmoidal crest of the perpendicular plate of the palatine bone. E, the sphenoid, ethmoid, and maxillary bones and the vomer have been fitted together. The perpendicular plate of the ethmoid forms the upper part of nasal septum and the vomer forms the lower part. The frontal processes of the maxillae form the anterior part of the lateral wall of the nasal cavity. F, anterior view. The sphenoid, occipital, and left palatine bones have been fitted together. The pharyngeal tubercle is exposed in the midline on the clival part of the occipital bone. The sphenopalatine notch of the palatine bone, located between the orbital and sphenoid processes, is closed superiorly by the inferior surface of the sphenoid bone to form the sphenopalatine foramen. The anterior end of the vidian canal is sometimes seen through the sphenopalatine foramen. G, anterior view. The occipital, sphenoid, and left palatine bones and the axis and atlas have been fitted together. The clivus and atlas (C1) can be viewed through the nasal cavity between the body of the sphenoid above, the horizontal plate of the palatine bone below, and the vertical plate of the palatine bone and pterygoid process of the sphenoid bone laterally. H, oblique view of the left lateral wall of the nasal cavity. The sphenoid and left maxillary and palatine bones have been fitted together. The lower half of the lateral nasal wall is composed of, from anterior to posterior, the maxilla, the perpendicular plate of the palatine bone, and the medial pterygoid plate. The sphenopalatine foramen is located just above the ethmoidal crest of the palatine bone. The maxillary hiatus, a large opening in the medial wall of the maxillary sinus, is formed by the maxilla anteriorly and the perpendicular plate of the palatine bone posteriorly. The hiatus is partially closed by the inferior nasal concha and the ethmoid bone.

圖3。投入。我放大視圖。J,顱底側麵圖。翼齶窩是上頜竇後壁上半部分與蝶骨翼突之間的狹窄空間。蝶齶孔通過窩內側壁進入鼻腔。K,矢狀切麵標本右外側鼻壁。上、中、下鼻甲已經切除。一根細長的彎曲骨,稱為鉤突,連接上頜裂孔的前部,並將上頜裂孔分為前後間隙。後間隙稱為半月裂孔,位於鉤突和篩大泡之間,其特征為弧形。 The anterior space is closed by the mucosa in life. The posterior space is also closed by mucosa except at the ostia draining the maxillary, ethmoidal, and frontal sinus into the nasal cavity. The sphenopalatine foramen is located behind the ethmoid bulla. L, anterior view of the sphenoid bone. The left half of the anterior wall of the sphenoid sinus has been opened. The anterior wall of the sphenoid sinus consists of 2 areas, an upper and lateral depressed area, which shares its wall with the posterior ethmoid cells, and is hidden behind the ethmoid air cells. In this specimen, the most posterior ethmoid cells extend into the sphenoid sinus and are called Onodi cells. A lower and medial smooth triangular area that can be viewed through the nasal cavity behind the superior turbinate corresponds to the sphenoid conchae. The ostia of the sphenoid sinus are located near the superior angles of the sphenoid concha. The sphenoidal crest forms a small part of the nasal septum and articulates with the perpendicular plate of the ethmoid bone. M, inferior view of the sphenoid and palatine bones and the vomer. The upper border of the vomer is expanded into an ala on each side and attaches to the sphenoid bone. The lateral border of each ala articulates with a thin bony lamella, the vaginal process of the sphenoid bone, which projects medially from the root of the medial pterygoid plate to complete the palatovaginal canal. The pterygoid hamulus, around which the tensor veli palatini muscle turns medially to insert into the soft palate, projects laterally from the tip of the medial pterygoid plate. N, inferior view of the occipital bone. The pharyngeal tubercle is located in the midline of the clivus approximately 1 cm anterior to the anterior edge of the foramen magnum. The occipital condyles project downward along the anterolateral margin of the foramen magnum. There is a small bony groove, the supracondylar groove, for the insertion of the rectus capitis anterior muscle in front of each occipital condyle. The extracranial end of the hypoglossal canal opens above the occipital condyle. O, anterior view. The sphenoid and occipital bones are fitted together. The areas corresponding to the upper, middle, and lower clivus are shown on the exocranial aspect. The anterior end of the vidian canals sits at the junction of the upper and middle clivus. The pharyngeal tubercle can be used to estimate the junction of the middle and lower clivus. Car., carotid; Cond., condyle; Eth., ethmoid; Fiss., fissure; For., foramen; Front., frontal; Gr., greater; Horiz., horizontal; Hypogl., hypoglossal; Jug., jugular; Lac., lacrimal; Lat., lateral; Less., lesser; M., muscle; Max., maxillary; Med., medial; Occip., occipital; Orb., orbital; Pal., palatine; Palatovag., palatovaginal; Perp., perpendicular; Petrocliv., petroclival; Pharyng., pharyngeal; Proc., process; Pteryg., pterygoid; Pterygopal., pterygopalatine; Sphen., sphenoid; Sphenopal., sphenopalatine; Sup., superior; Temp., temporal; Tuberc., tubercle; Vag., vaginal, Vomerovag., vomerovaginal.
在經鼻入路時,顱外表麵的某些標誌可能是有用的(圖5)。
在大多數情況下,上斜坡和中斜坡之間的界限,定義為外展神經硬腦膜孔的水平,接近蝶竇底。然而,氣孔和蝶竇底之間的關係根據蝶竇的肺化程度而不同。頸內動脈的下緣,或淚盆和頸下段的交界處,為硬腦膜孔提供了標誌。33
外展神經起於橋髓連接處,在腦膜前池上升到達硬腦膜孔(圖6和7)。然後在硬腦膜兩葉之間上升,從幾乎垂直於動脈的頸動脈旁中點後方通過,並從Gruber韌帶下方進入海綿竇。33硬腦膜孔位於頸動脈腹旁段下限的同一水平(圖5L)。這個點對應於“撕裂骨段的上限”,被Barges-Coll等人認為是外展孔的一個標誌。33維底管的後端在頸內動脈的膝前或淚盆段的下外側打開。28這種解剖關係使維管成為經鼻擴張入路中到達頸動脈淚盆段的重要地標。19日,28日,34在我們的研究中,外展神經硬腦膜孔位於維管後端上方平均4.9毫米(範圍4-6毫米)處。
維甸神經從翼齶窩向後延伸,穿過維甸管,到達頸內動脈淚滴段的外側表麵和海綿竇的前內側(圖5-7)。如圖6E所示,神經在裂孔處略微向上彎曲,並與岩大神經和岩深神經相連。岩大神經起源於膝狀神經節,在頸岩水平段的上方和三叉神經節的下方向維甸管延伸。當它向內側延伸時,它沿著頸動脈管的前部向下延伸並與岩深神經相連,岩深神經是頸動脈交感神經叢的分支,形成維神經。雖然維神經後端和頸管都是頸內動脈前膝的重要標誌,但它們在頸岩動脈上的位置不同。維管神經從起源處向前延伸,沿頸動脈向下轉入維管的後端,維管位於淚孔的下外側邊緣和頸動脈岩末的下外側(圖7I-7L)。誤解這些關係可能會造成頸動脈損傷。
中、下斜坡在舌咽部軸向水平處劃分,與頸靜脈孔的上內側邊界相對應。前向觀察頸靜脈孔顱外孔時,可以看到舌咽神經從乙狀結腸部前緣的頸靜脈孔中出來。然而,在經鼻入路中,頸靜脈孔的顱外孔不被認為是介於中斜坡和下斜坡之間的手術標誌,因為頸靜脈孔位於太過外側。咽結節是中線上一致的骨突出,是判斷中、下斜坡邊界的較好地標。從硬齶前方平行觀察,中斜坡和下斜坡之間的邊界近似於咽結節的前緣水平(圖5);結節頂端上方的邊緣平均為3.9毫米(範圍2-8毫米)。邊緣位於髁上溝上方平均7.0 mm(範圍4-10 mm)處,用於頭前直肌的附著。打開斜坡就在咽部結節前尖的下方露出舌咽神經的池部就在它離開硬腦膜之前。
斜坡的階梯式開口,依次打開上、中、下斜坡的右、左半部分,清晰地顯示了顱外和顱內結構的關係(圖5E-5L)。上斜坡垂直長度平均為17.3 mm;中斜坡,13.7 mm;下斜坡,15.2毫米。上、中斜的腦幹分界對應腦橋的中段,中、下斜的腦幹分界對應腦橋髓溝。打開上、中、下斜坡,分別暴露腦橋上半部分、腦橋下半部分和髓質的前表麵。
通過打開前壁和部分蝶竇底,通常可暴露整個上斜坡。在暴露上斜坡時,直式內窺鏡沿上鼻道向蝶骨口推進進入鼻腔(圖7)。右側中鼻甲被外側碾碎(側化)或切除,下鼻甲被側化。將鼻中隔後部與蝶骨脊分離,切除鼻中隔後緣約1cm處,為雙鼻孔內固定提供視野。蝶竇前壁在蝶甲和蝶脊水平處的開口為蝶竇提供了一個三角形的通道,在側麵受到上鼻甲和後篩竇細胞的限製。切除上鼻甲和後篩竇細胞(後篩竇切除術)可拓寬通向蝶竇的手術路徑。
通過從竇底內側向外側鑽孔來確定維管。管常被認為是竇底的突出部位(圖4K)。在蝶竇底有3個前後方向的通道:從內側到外側,分別是犁陰道、齶陰道和維底管(圖6和7F)。最內側的管,犁陰道管,更多的是一個淺骨溝而不是一個管。當從蝶竇的內側到外側鑽孔時,通常首先會碰到齶陰道管,也稱為齶蝶竇管,它可能會被誤認為維迪管,因為這兩個管都有神經和動脈,並通往翼齶窩齶陰道管從翼齶神經節傳咽神經,從上頜動脈第三段傳咽動脈,比咽管中的維神經和動脈小得多。齶陰道管和維氏管的另一個區別是,從前端到後端,齶陰道管的走向與矢狀麵呈內側角度,而維氏管的走向則呈輕微的外側角度。維管的前開口位於齶陰道管外側約2mm,35但它們可能共享同一個前開口。側向45內窺鏡可使通過蝶竇的維管可視(圖4K)。
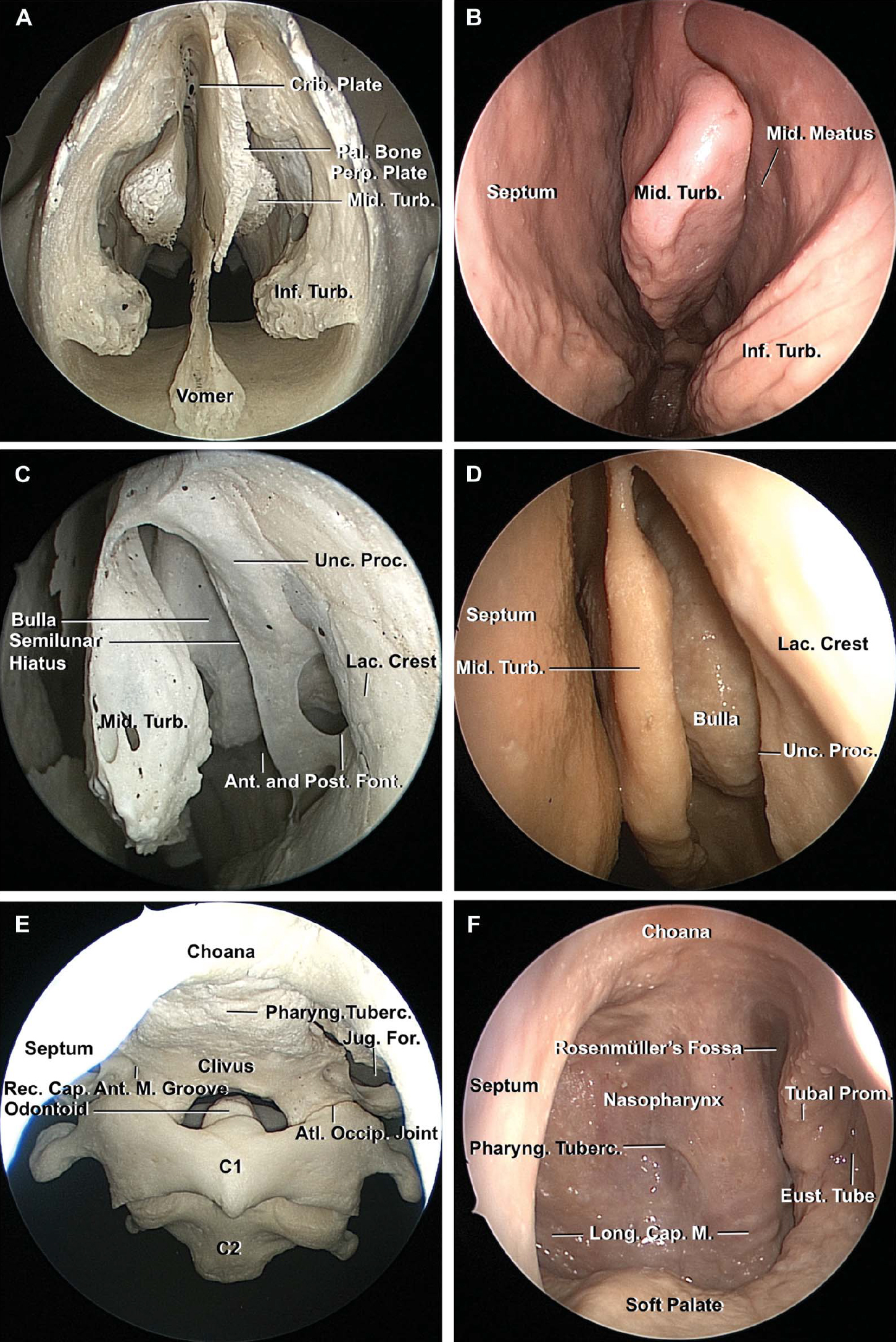
圖4。f。A,通過骨鼻腔前鼻孔的內窺鏡視圖。篩骨、犁骨和蝶骨脊的垂直板形成骨性鼻中隔。中、下鼻甲伸入鼻腔。B、鼻腔粘膜完好。內窺鏡已插入左鼻孔。篩竇大泡和鉤突隱藏在中鼻道的中鼻甲下,隨著內窺鏡的推進而暴露出來。C, a的放大視圖。左側篩竇大泡是一個圓形的骨突出物,覆蓋在篩竇氣細胞上,位於中孔上外側的鉤突後。鉤突起於篩骨最前麵的空氣細胞——鼻角細胞,向下向後延伸,附著於下甲。 The uncinate process divides the maxillary hiatus into a smaller anterior part and a larger posterior part called the anterior and posterior fontanelles, respectively. In life, the anterior part is closed by the mucosa, whereas the posterior part forms the infundibulum, leading to themaxillary, frontal as ethmoid ostia. The uncinate process obscures the direct view of the maxillary ostium and semilunar hiatus inthe view through the 0° endoscope. D, view with intact mucosa. The ethmoid bullae and uncinate process are positioned lateral tothe middle turbinate in the middle meatus. E, anterior view of the clivus. The pharyngeal tubercle, a good landmark for the demarcation between the middle and lower clivus, is seen in midline, whereas the anteromedial edge of the jugular foramen, which sits at the junction of the middle and lower clivus, may be difficult to see through the nasal cavity. The small groove for the insertion of the rectus capitis anterior muscle is seen at the upper anterior edge of the occipital condyle. F, anterior view of the opening from the nasal cavity into the nasopharynx. The tubal prominence is seen behind the ostium of the eustachian tube. The fossa of Rosenmüller projects laterally behind the tubal elevation. The pharyngeal tubercle and longus capitus underlie the mucosa.
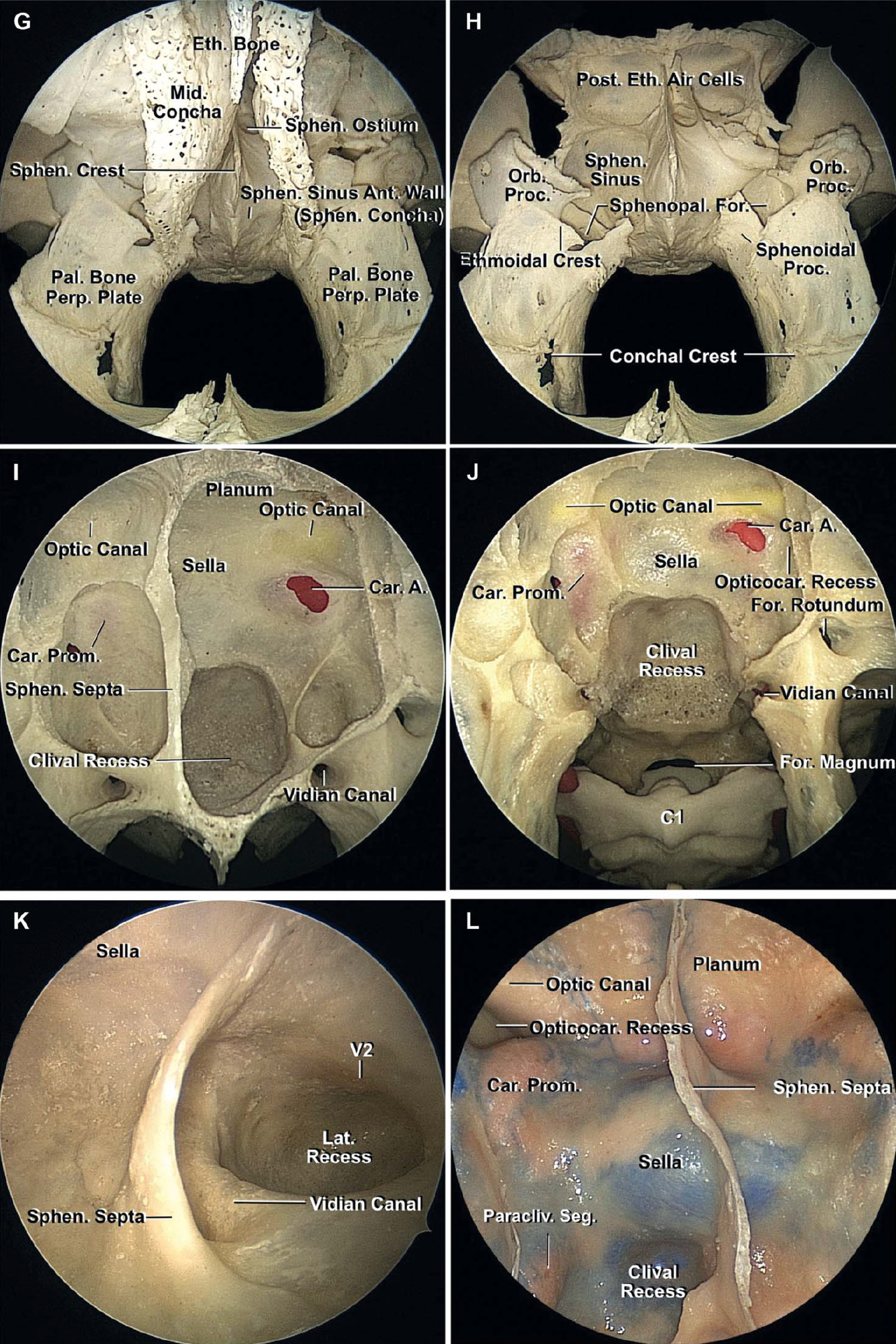
圖4。G-L。G,重建蝶骨、篩骨和雙齶骨的前內窺鏡視圖。通過鼻腔隻能看到蝶竇前壁的下內側部分,也就是蝶竇的鼻甲。蝶竇前壁的其餘部分隱藏在篩骨後麵,篩骨與蝶竇前壁共用後壁。蝶竇口暴露於蝶甲上角附近。篩竇後空氣細胞與蝶竇前壁的上外側有一個共同的壁。H,篩骨被切除了。的right half of the anterior wall of the sphenoid sinus has been opened. The sphenopalatine foramen is located just above theethmoid crest in the lateral wall of the nasal cavity between the sphenoid and orbital processes of the palatine bone. I, posterior wallof the sphenoid sinus. There is a spontaneous dehiscence of bone over the left carotid artery. The posterior sinus wall is limitedsuperiorly by the sellae and laterally by the prominences overlying the cavernous carotid. The posterior sinus wall corresponds tothe part of the clivus formed by the sphenoid bone. The sinus wall often extends posteriorly beyond the vertical coronal plane ofposterior wall of pituitary fossa to form a clival recess. The vidian canal is located at the lower lateral corner of the sphenoid sinus.J, view extending to the clivus, foramen magnum, and C1. In this specimen, the opticocarotid recesses, the recess located betweenthe optic canal and the carotid prominence that extends into the optic strut, is shallow. K, left lateral wall of the sphenoid sinusviewed with a 45° endoscope. In this specimen, the pneumatization extends laterally beyond the vidian canal into the greater wingto form a lateral recess. The left vidian canal underlies a bony ridge in the lateral part of the floor of the sphenoid sinus. L, posteriorwall of the sphenoid sinus in another specimen. The vertical paraclival segment of the carotid artery ascends along the lateral limitof the posterior wall of the sphenoid sinus. A., artery; Ant., anterior; Atl., atlanto; Cap., capitis; Car., carotid; Crib., cribriform;Eth., ethmoid; Eust., eustachian; Font., fontanelles; For., foramen; Inf., inferior; Jug., jugular; Lac., lacrimal; Long., longus; M.,muscle; Mid., middle; Occip., occipital; Opticocar., opticocarotid; Orb., orbital; Pal., palatine; Paracliv., paraclival; Perp., perpendicular; Pharyng., Pharyngeal; Post., posterior; Proc., process; Prom., prominence; Rec., rectus; Seg., segment; Sphen., sphenoid; Sphenopal., sphenopalatine; Tuberc., tubercle; Turb., turbinate; Unc., uncinate.
移除蝶隔,沿內側至外側方向鑽入斜坡隱窩,暴露斜坡硬腦膜,平行於頸內動脈,以防止動脈損傷。上斜坡與岩尖在中線外側約10毫米處並在頸內動脈後方相連。纖維軟骨填充沿岩尖和斜坡之間連接的垂直凹槽(圖7I)。在鑽上斜坡最外側部分時,應注意避免損傷外展神經,因為神經穿過岩斜坡連接處的上邊緣。
上斜坡硬腦膜很容易分為兩層:麵向骨的骨膜層和麵向腦幹的腦膜層(圖8)。顱底、岩上竇和岩下竇在兩層硬腦膜之間。基底靜脈叢位於上斜坡的後表麵,連接成對的海綿竇的後端,打開基底靜脈叢可能會導致嚴重出血。靜脈叢在向枕骨大孔下降時變得不那麼突出。每個海綿竇的後端與上、下岩竇和基底竇形成獨特的靜脈彙合處或溝。外展神經穿過腦膜硬腦膜,穿過靜脈彙合處,然後穿過蝶顱韌帶(Gruber’s)下方。然後神經繞過頸內動脈的外側到達眼神經的內側在海綿竇的外側壁。用斜坡鑽孔保留Gruber韌帶有助於保持外展神經的位置(圖7K)。
打開上斜坡硬腦膜有損傷外展神經的潛在風險,特別是硬腦膜間段,因為硬腦膜間段可能難以定位,靜脈出血可能進一步模糊其識別。成對外展硬腦膜孔之間的距離平均為20.9 mm(範圍18-25 mm)。Barges-Coll等33報告外展神經在橋髓溝處的水平距離為10 mm,在靜脈彙合處的水平距離為18.5 mm。外展神經的硬膜間段常伴有腦膜背動脈,它通常起源於頸內動脈的腦膜下垂體支的鞍背水平。6%的腦膜背動脈直接來自腦膜垂體幹起源下方的海綿內頸動脈。36起點遠端動脈與外展神經一起向後穿過海綿竇,到達背側和斜坡上的硬腦膜,並在那裏沿外展神經向內側延伸至Gruber韌帶下方(圖7K)。45內窺鏡向外側可幫助顯示外展神經硬膜間段、腦膜背側動脈和格魯伯韌帶。

圖5。A-D,鼻咽和斜坡逐步剝離。A,翼狀突前麵的冠狀麵。蝶竇、鼻腔和鼻咽為斜坡提供通道。顳下窩位於鼻腔和鼻咽部外側,包含翼狀肌外側和內側、上頜動脈、下頜神經和翼狀靜脈叢的分支。B,翼肌,顳肌下部,犁肌都被切除了。維管位於蝶竇底的下側角,在這裏,沿著蝶竇底的水平線與沿著蝶竇外側壁和內側翼板的垂直線相遇。C為右側翼突、張肌、齶提肌和鼻咽結構,除右側咽鼓管外,保留維管。咽鼓管從中耳延伸,沿著翼狀內側板的後緣,進入鼻咽部。頸內動脈和頸內靜脈位於卵圓孔和下頜神經分支的後麵。 D, the pterygoid processes have been removed on both sides, and the eustachian tubes have been retracted laterally to provide an anterior view of the clivus and the adjacent area. The anterior edge of the exocranial orifice of the jugular foramina is located at almost the same level as the anterior edge of the pharyngeal tubercle. The soft palate sits at the level of the foramen magnum.

圖5 E-J。E-L,逐步剝離,顯示顱外標誌與顱內結構之間的關係。E,下坡的右半部分已經打開了。中斜坡和下斜坡之間的邊界接近咽結節的前緣。舌咽神經和迷走神經暴露在舌下管上方。F,下斜坡的左半部分也已經打開,髓質已經暴露。顱內中下斜坡的分界在舌咽神經正上方的橋髓溝處。G,上斜坡右半部分的骨頭和硬腦膜已經打開。頸內動脈的垂直段,沿著蝶竇後壁的外側邊界上升,稱為臨骨段。上斜坡和中斜坡之間的邊界位於頸內動脈臨骨段下限的同一水平線上。 H, removing the left half of the upper clivus and opening the dura exposes the upper part of the pons. The lacerum segment of the petrous carotid is positioned at the anterior genu below the paraclival segment. I, the right half of the middle clivus has been opened. A thin dural bridge has been preserved at the junction of the upper and middle clivus, and a thin bony bridge has been preserved at the junction of the middle and lower clivus. J, the left half of the middle clivus has been opened to expose the intradural structures in the upper, middle, and lower clival regions. The middle clival opening exposes the lower pons.

圖5。K和L,在(K)和(L)打開斜坡之前顱底中線的放大前視圖。薄硬腦膜橋將上、中斜坡分開,薄骨橋將中、下斜坡分開。上斜坡和中斜坡之間的邊界位於頸動脈岩的臨骨段和裂骨段的交界處(黃色虛線),大約在維管後端上方5mm。中斜坡和下斜坡之間的邊界位於咽結節頂部上方約4mm處。打開上、中、下斜坡,分別暴露腦橋上半部分、腦橋下半部分和髓質的前表麵。當維甸管從前端延伸至後端時,其延伸方向與矢狀麵呈輕微的側向角度,幾乎與硬齶平麵平行,或與硬齶平麵呈輕微的向下角度。維底管的後端位於頸內動脈的前膝下外側,或淚盆段。一個,動脈;A.I.C.A.; anterior inferior cerebellar artery; Ant., anterior; Asc., ascending; Bas., basilar; Car., carotid; CN, cranial nerve; Cond., condyle; Eust., eustachian; Fiss., fissure; For., foramen; Hypogl., hypoglossal; Inf., inferior; Int., internal; Jug., jugular; Lat., lateral; M., muscle; Mass., masseter; Max., maxillary; Med., medial; N., nerve; Occip., occipital; Pal., palatini; Paracliv., paraclival; Pet., petrous, petrosal; Petrocliv., petroclival; Pharyng., pharyngeal; Pit., pituitary; Post., posterior; Proc., process; Prom., prominence; Pteryg., pterygoid; S.C.A., superior cerebellar artery; Seg., segment; Sphen., sphenoid; Stylopharyng., stylopharyngeus; Temp., temporal; Tens., tensor; Tuberc., tubercle; V., vein; Vag., vaginal; Vert., vertebral.
打開垂體下的上斜坡硬腦膜,暴露腦橋前表麵的上半部分和腦橋前池(圖7L和8)。這種暴露的上限是腦橋-後腦交界處和Liliequist膜的中腦葉,如果不向上延伸到垂體後。位於橋腦前膜外側的橋小腦池的暴露受到頸內動脈和岩尖的限製。除非動脈明顯拉長,否則可見基底上動脈及其通向腦橋的穿支(圖7L)。小腦上動脈(SCA)的橋腦前段,在橋腦交界處附近環繞腦幹,在上45內窺鏡的曝光上限處可見。
在隻限於上斜坡的暴露中沒有暴露顱神經。三叉神經起於上斜坡水平,在橋小腦池中走行,通過暴露部位的外側。通過鑽蝶骨舌突和岩尖擴展暴露,包括或不包括頸內動脈轉位,提供三叉神經和Meckel 's洞穴的前視圖,但在局限於斜坡的暴露中看不到。37,38動眼神經起於中腦前部,經過SCA上方,除非暴露向上延伸,否則看不到。
上斜坡上徑路的上延伸伴垂體腺的升高和鞍背的切除將暴露出椎弓根間池。但是,由於鞍底硬腦膜的骨膜層在頸內動脈和鞍膈周圍與硬腦膜融合,形成垂體窩頂,與硬腦膜上環融合,硬腦膜上環包圍並緊緊附著於頸內動脈,因此,通過簡單的上斜坡路徑很難將完好的鞍硬腦膜的垂體腺抬高。將垂體囊從海綿竇的內側壁分離,這個過程被Kassam等人描述得很好,18有助於提升腺體和暴露鞍背。
骨膜和腦膜硬腦膜層排列在鞍底和垂體腺下表麵(圖8)。骨膜層粘附在蝶骨上,腦膜層從膈肌沿垂體腺向下延伸。硬腦膜的雙層結構在蝶鞍底部很明顯,特別是在位於兩層之間的海綿間竇處。海綿竇內側壁由一層薄薄的腦膜硬腦膜形成(圖8B),它將腦垂體的外表麵與頸內動脈分隔開來。39垂體包膜是一種非常薄的半透明膜,它緊緊地附著在緊鄰海綿竇內側壁的垂體腺上,通過仔細的解剖可以與海綿竇內側壁分離。海綿竇內側壁鞍部覆蓋前葉外側表麵,後葉位於鞍背前凹前表麵的前葉和海綿竇內側壁的後麵,在海綿竇內側壁鞍部沿背內表麵外側邊緣與硬腦膜融合的後麵。
腦垂體通過腦垂體囊和海綿竇內側壁之間的開口與硬腦膜結構分離。這允許腺體向上轉位以切除鞍背。需要注意避免垂體下動脈過度移位和撕脫,該動脈起源於鞍背外側的腦膜垂體幹,並向內側為後葉供血。
該方法暴露了位於蛛網膜下腔幕上和幕下交界處的踝間池和Liliequist膜葉(圖8D)。動眼神經在花序梗間池的側壁內走行,形成利列奎斯特膜葉附著的支柱。通過該方法,所有標本均可暴露SCA和大腦後動脈的起源。打開Liliequist膜的間腦葉,它延伸到足間池上方,暴露出交叉池和頸動脈池中的後交通動脈和頸內動脈段。這種暴露,在擴展上斜坡暴露的上限,可能需要70內窺鏡(圖8F)。
與位於蝶鞍後麵的上斜坡相反,下斜坡位於鼻咽後壁的後麵,鼻咽後壁通過後鼻孔(鼻後孔;圖9和10)。後鼻孔是由蝶骨體上方形成的成對孔,外側由齶骨垂直板和內側翼狀板形成,下方由齶骨水平板形成,內側由中線處的耙骨形成。咽鼓管沿內側翼板後緣在鼻咽側壁上打開。幾塊肌肉,包括張肌、齶帆提肌和輸卵管咽肌,附著在咽鼓管上並通過打開咽鼓管起作用,而咽鼓管大部分時間保持閉合狀態(圖9)。在咽鼓管口後麵,由咽鼓管軟骨部分的底部形成的粘膜下有一個堅硬的凸起,即咽鼓管凸起(或咽鼓環)。咽鼓管和輸卵管抬高位於下斜坡入路的側限。如前所述,咽鼓管口之間的橫向距離平均為24.1 mm,咽鼓管高度之間的橫向距離平均為14.7 mm。21咽隱窩(或Rosenmüller窩)從鼻咽後外側角向外突出,位於咽管隆起後。咽旁頸內動脈延伸到Rosenmüller窩的外側邊緣。
對於下斜坡的入路,在鼻咽後壁上做一個u形或線形粘膜切口,切口上緣位於咽結節略上方。頭長肌與斜坡的附著通常表現為v型粘膜隆起。咽結節位於V下端中線處(圖10A和10C)。在頭長肌插入處上方有一個淺的倒三角形粘膜凹陷,這與兒童時期咽扁桃體或腺樣體的位置相對應。
鼻咽後壁的肌肉結構分為3層(圖9I和9J)。咽基底筋膜是打開鼻咽粘膜後最淺的一層,覆蓋頭長肌。它與枕骨和顳骨的下表麵緊密相連。隨著筋膜的下降,它的厚度逐漸減少,並在軟齶水平逐漸融入咽上收縮肌。咽上縮肌插入咽中縫,中縫與咽結節相連。上縮肌的上緣位於C1水平,通常不打開以暴露下斜坡。咽基底筋膜在其上緣處與蝶骨和枕骨之間的纖維軟骨和淚孔處融合。第二層是頭長肌。頸內動脈咽旁段向上延伸到頭長肌。纖維軟骨沿著頭長肌附著的外側邊緣填充岩斜裂隙。 The third and deepest layer of the posterior nasopharyngeal wall consists of the rectus capitis anterior and the longus colli muscles. The rectus capitus anterior is a short, flat muscle that extends across the front of the atlanto-occipital joint. The muscle usually attaches in a groove just above the occipital condyle, but its attachments may be associated with a tubercle that can be mistaken for the medial edge of the occipital condyle. The hypoglossal nerve and neuromeningeal branches of the ascending pharyngeal artery course along the lateral edge of the rectus capitus anterior (Figure 9). The longus colli muscle is not encountered in the lower clival approach because it inserts below the exposure into the atlas. The petrosal venous confluence is situated lateral and deep to the rectus capitis anterior muscle, around the extracranial orifice of the jugular foramen and hypoglossal canal, where the lower end of the inferior petrosal sinus connects to the venous plexus of the hypoglossal canal and prevertebral venous plexus (Figures 9E and 10I).26它通過舌咽部和迷走神經之間靜脈壁上的1到2個開口流入頸靜脈球的內側或者流入頸靜脈孔下麵的頸內靜脈。岩斜坡下靜脈沿岩斜坡裂隙顱外表麵走行,與顱內側的岩下竇形成鏡像,並流入岩彙合處。岩斜下靜脈上端經裂孔與頸動脈周圍的靜脈叢或直接與海綿竇相連。咽升動脈的腦膜神經支在頸靜脈孔下方形成分支,穿過岩彙合處、舌下管和頸靜脈孔為周圍的硬腦膜供血。

圖6。上斜坡的階梯式顯露。A,維竇管沿竇底側緣延伸。齶陰道管位於齶骨蝶突和蝶骨陰道突之間,位於維管內側。B,放大圖。蝶中隔和翼突被切除。犁體的翼(翼)沿蝶竇底附著。犁陰道管位於犁骨翼和蝶骨陰道突之間,是一個較淺的骨槽而不是管。在a.c中,犁陰道管位於齶陰道管的內側。海綿竇的內側壁已經打開,頸動脈的海綿段已經暴露出來。竇後壁,上受鞍區限製,外側受頸動脈臨骨段限製,對應於由蝶骨形成的斜坡部分。 D, the right half of the upper clivus has been drilled. The periosteal layer of the clival dura has also been opened to expose the basilar venous plexus. A bundle of the carotid sympathetic plexus ascends on the cavernous carotid and joins the abducens nerve. E, anterior, oblique view of the right anteromedial cavernous sinus. The venous confluence surrounding the dural porus of the abducens nerve has been removed. The vidian nerve runs below anathe cavernous segment of the abducens nerve runs above the lingual process of the sphenoid bone. The vidian nerve, when followed posteriorly, reaches the lateral surface of the lacerum segment of the petrous carotid artery. Here, the nerve turns slightly upward in the foramen lacerum and is continuous with the greater petrosal and the deep petrosal nerves. The abducens nerve, when followed anteriorly, exits its dural porus and ascends lateral to the internal carotid artery. F, the upper clivus has been opened and the dura, above the level of the dural porus of the abducens nerve (yellow arrow), has been removed. The basilar artery and the upper half of the pons are exposed. A., artery; Bas., basilar; Car., carotid; Cav., cavernous; CN, cranial nerve; Dist., distal; For., foramen; Hyp., hypophyseal; Inf., inferior; N., nerve; Ophth., ophthalmic; Palatovag., palatovaginal; Paracliv., paraclival; Pet., petrosal; Pit., pituitary; Plex., plexus; Proc., process; Prom., prominence; Seg., segment; Sphen., sphenoid; Sup., superior; Vomerovag., vomerovaginal.
前頭直肌的收縮或切除暴露了枕骨髁和舌下管。枕髁和舌下管位於0°內窺鏡下斜坡暴露的外側極限(圖10K和10L)。在鑽開翼突根後,將45°內窺鏡插入咽鼓管軟骨部分上方,可看到頸靜脈孔的顱外孔(圖10I和10J)。鑽這個部位並從內側路徑暴露頸靜脈孔在技術上是困難的,需要非常注意,因為咽鼓管的軟骨與填充淚孔下部的軟骨混合在一起。在咽部結節前緣以下的斜坡部分,向下延伸到枕骨髁的外側。斜坡開口在舌下管的外側受限,舌下管從顱外開口後內側穿過。在舌下管上方區域可以獲得更寬的斜坡開口,這裏的斜坡開口在側麵受到岩斜坡裂隙和頸靜脈孔的限製。在本研究中,舌下管上方平均走廊寬度為38.6 mm,舌下管水平平均走廊寬度為26.6 mm。頸靜脈結節位於顱內表麵岩斜裂、頸靜脈孔和舌下管之間的三角形區域。該區域由下斜坡最厚部分的堅硬致密骨組成。 Drilling here requires great care to avoid damaging the hypoglossal canal and cisternal portion of cranial nerves IX, X, and XI, which rest on the dura covering the jugular tubercle.
齒狀突頂端韌帶從齒狀突頂端延伸到枕骨大孔的前緣,位於寰枕前膜和十字韌帶的上延伸處之間。十字形韌帶的上垂帶和被膜附著於斜坡的上表麵。翼韌帶是兩條強壯的筋帶,分別出現在齒狀突上部的兩側,並向斜上外側延伸,附著於枕髁的內側表麵。雖然根尖韌帶在維持頭部和頸部之間的穩定方麵作用很小,40翼韌帶的橫斷可能導致寰枕關節和寰樞關節的不穩定。第四十一條、第四十二條在保留關節突及其內側表麵皮質骨的情況下鑽孔枕骨髁的鬆質骨可以避免術後不穩定。
發育良好的硬腦膜靜脈竇在舌下管周圍延伸,並與枕邊的大孔竇和舌下管內的舌下靜脈叢相通。當切開下斜坡硬腦膜時,硬腦膜竇可能是一個特殊的挑戰。
打開下斜坡硬腦膜幾乎暴露了髓質的所有前表麵(圖9H和10M)。橋髓溝位於中斜坡和下斜坡的交界處,枕骨大孔的前緣與舌下管的最下根從髓質發出的位置重合。第一頸神經位於枕骨大孔下方。在枕骨大孔和寰椎間打開硬腦膜暴露頸髓的上端和C1神經,盡管這需要橫斷十字韌帶的頂端和上垂直支。下斜坡開口主要通向髓前池,其上部受內側橋髓性蛛網膜的限製,外側受小腦髓池的限製,小腦髓池起始於舌咽神經、迷走神經和副神經前麵的橄欖後緣。下斜坡入路隻延伸到小腦髓池的一小部分前部。
打開下斜坡暴露的顱神經是舌咽神經、迷走神經、副神經和舌下神經,它們都起源於髓質,與小腦後下動脈(PICA;圖10 m-10o)。中斜坡和下斜坡之間的邊界位於舌咽神經池部的上方。通過鑽頸靜脈結節可暴露舌咽部和迷走神經的池部,頸靜脈結節對應於經鼻入路舌下管上方的骨區。前視時,起源於髓質的附屬小根通常隱藏在舌下小根、管和椎動脈後麵。舌下管鑽孔擴大了通道,促進了副小根的暴露,但可能導致舌下靜脈叢和咽升動脈腦膜分支出血,並有損傷舌下神經的危險。
打開下斜坡幾乎暴露了整個椎動脈硬膜內段(圖9H和10M)。在大多數情況下,椎動脈在舌下小根的前麵走行,因為它上升到連接另一個椎動脈在橋髓溝處或附近。下斜坡的開口也暴露了異食尼卡的前髓段和外側髓段。本研究中20例PICA中有19例發生於下斜坡開口;1異食癖發生於中斜坡與下斜坡交界處的椎動脈。如果動脈起源於椎動脈的硬膜外部分,則異食癖的起源可能無法從經鼻鏡觀察到。脊柱前腹側動脈及其起源在所有標本的下斜坡開口均可見。
中斜坡的標誌是位於其上邊界的頸動脈旁的下限和位於其下邊界的咽結節。中斜坡的前表麵對應於犁骨與蝶竇底和枕骨上部的附著區域。鼻咽暴露與下斜坡相同。手術走廊到中斜坡的外側界限是上麵的翼狀突上部和下麵的輸卵管隆起。翼突內側邊緣之間的距離平均為24.9 mm。如果不切除翼狀突的根,很難暴露中斜坡外側邊緣的裂孔和岩斜坡裂隙。移除翼突的步驟在以前的文章中已經描述過,重點是經翼突入路進入顳下窩。17日,43-45移除中鼻道外側壁的鉤突以暴露上頜口(鉤突切除術),將其向後擴大至齶骨垂直板前緣水平(後竇口造口術)。蝶齶動脈穿過的蝶齶孔和篩骨脊(位於齶骨垂直板上的水平脊,在那裏有中甲關節)是暴露翼齶窩的重要標誌(圖3和圖4)。蝶齶孔位於蝶齶脊上方。切除上頜竇後內壁和齶骨眶突,暴露翼齶窩、維管和圓孔。翼突前表麵的暴露需要翼齶內內容物的側向回縮,包括維管;眶下,較大和較小的齶神經;蝶齶骨的神經節;還有上頜動脈的末端分支。在翼突的後方鑽孔,露出頸內動脈。19日,28日維甸管通向頸動脈的膝前段,或頸動脈的切淚段。19日,28日腓神經的後部分隱藏在淚孔上部前外側緣的纖維軟骨中,岩深神經和岩大淺神經在此彙合形成腓神經(圖11)。
取出犁體,從內側到外側鑽取中間斜坡(最厚的部分)以暴露硬腦膜。中斜坡的梯形外側與上部的裂孔和頸內動脈和下部的岩斜坡裂縫接壤(圖11)。中斜坡入路的硬腦膜開口在外側受到岩下竇的限製,岩下竇沿岩斜坡裂隙的顱內側延伸。下岩竇上下段的橫向距離平均分別為21.9 mm和38.6 mm。犧牲岩下竇可使暴露擴大到岩尖內側邊緣。鑽鑽岩尖下部將暴露向外側延伸至頸岩。

圖7。f。接近上斜坡。通往上斜坡的路徑通過蝶竇。A到C,蝶竇和斜坡的關係。A,蝶竇的前視圖。後篩竇氣細胞與蝶竇上外側麵有一個共同的壁,並沿蝶竇口外側邊緣延伸。在篩竇氣細胞下麵和中間的蝶麵部分稱為蝶甲。蝶口位於蝶甲狹窄的上部。鼻甲形成了蝶竇前壁的大部分。 B, the posterior ethmoid air cells and the sphenoid concha have been opened to expose the sphenoid sinus. The approach to the upper clivus is directed through the back wall of the sinus below the sella. The approach can be extended upward by elevating the gland and opening through the dorsum sellae. C, the pituitary gland and petrous and cavernous carotid have been exposed. The vidian canals are located along the lateral margin of the sinus floor. The maxillary and vidian nerves enter the posterior wall of the pterygopalatine fossa. The sphenopalatine arteries pass from the pterygopalatine fossa and through the sphenopalatine foramen to enter the nasal cavity. D, the straight endoscope has been advanced into the right nasal cavity toward the sphenoid ostium. For this exposure, the posterior part of the nasal septum has been detached from the sphenoid crest and displaced to the left, the anterior wall of the sphenoid sinus has been removed, and approximately 1 cm of the posterior edge of the nasal septum has been resected. Opening of the anterior wall of the sphenoid sinus, formed by the sphenoid conchae and the sphenoid crest, provides a triangular corridor to the sphenoid sinus. This corridor is limited laterally by the superior turbinate and the posterior ethmoid cells hidden behind the superior turbinate. The sellar dura and medial wall of the cavernous sinus have been exposed. The vomerovaginal canal is located medial to the palatovaginal canal. E, the dura covering the medial wall of the cavernous sinus has been opened. The pituitary gland and sellar dura has been retracted upward to expose the dorsum sellae. It is difficult to elevate the pituitary gland with the sellar dura intact because the dura is fixed to surrounding structures. F, the right half of the upper clivus has been drilled, and the periosteal layer of the clival dura has been opened to expose the venous confluence around the dural porus of the abducens nerve. The basilar venous plexus becomes less prominent as it descends toward the foramen magnum.

圖7。G-L。G,右側前內側海綿竇麵,45°內窺鏡向外側。維丁管向後打開,進入前外側邊緣,直到撕裂孔。眼神經和動眼神經在海綿竇外側壁內走行,外展神經在海綿竇內向前走行。上頜神經在海綿竇下方向前延伸。眼動脈和視神經通過視神經管視神經支柱的上方。顯露外展神經和基底靜脈叢的硬腦膜孔。維神經在蝶突舌突的下方展神經在蝶突舌突上方。H,圖像聚焦於右側頸動脈旁。 The lingual process of the sphenoid bone has been removed. The petrolingual ligament bridges the interval between the lingual process and petrous apex just below the cavernous sinus. The vidian nerve courses below the petrolingual ligament. The inferolateral trunk arises from the lateral aspect of the horizontal segment of the cavernous carotid, descends lateral to the abducens nerve, and supplies the dura of the inferolateral wall of the cavernous sinus surrounding the foramina rotundum and ovale. I, the petrolingual ligament has been removed, and the petrous apex and the gasserian ganglion have been exposed by retracting the ganglion laterally and the carotid artery medially. J, view of the left anteromedial cavernous sinus with a 45° endoscope directed laterally. The upper clivus has been drilled, and the periosteal layer of the clival dura has been opened to expose the venous confluens. K, the venous confluens around the dural porus of the abducens nerve has been removed. The abducens nerve penetrates the dura and ascends lateral to the carotid artery and below the petrosphenoid (Gruber’s) ligament, which extends from the lower part of the lateral edge of the dorsum sellae to the petrous apex. The dorsal meningeal branch of the meningohypophyseal trunk courses below Gruber’s ligament and near the abducens nerve. L, opening the upper clival dura below the pituitary gland exposes the upper half of the anterior surface of the pons. The outer arachnoid membrane has been opened and retracted laterally. The anterior pontine membranes, located just medial to the dural pori of the abducens nerves, separate the prepontine cistern from the cerebellopontine cisterns. The upper basilar artery and its perforating branches to the pons are well visualized. The rostral limit of the upper clival approach is usually at the pontomesencephalic junction. A duplicate left superior cerebellar artery encircles the brainstem near the pontomesencephalic junction. A., artery; A.C.A., anterior cerebral artery; Ant., anterior; Bas., basilar; Car., carotid; Cav., cavernous; Cist., cistern; CN, cranial nerve; Conf., confluence; Dor., dorsal; Eth., ethmoid; Fiss., fissure; For., foramen; Gang., ganglion; Hyp., hypophyseal; Inf., inferior; Inferolat., inferolateral; Lat., lateral; Lig., ligament; Max., maxillary; Med., medial; Men., meningeal; Memb., membrane; N., nerve; Ophth., ophthalmic; Palatovag., palatovaginal; Pet., petro, petrosal, petrous; Petrocliv., petroclival; Petroling., petrolingual; Pit., pituitary; Plex., plexus; Pon., pontine; Post., posterior; Prepon., prepontine; Proc., process; Pterygopal., pterygopalatine; S.C.A., superior cerebellar artery; Seg., segment; Sphen., sphenoid; Sphenopal., sphenopalatine; Sup., superior; Tr., trunk; Trans., transverse; V., vein; Ven., venous; Vomerovag., vomerovaginal.
打開中斜硬腦膜可暴露腦橋前表麵的下半部分、腦橋前池的下半部分和腦橋小腦池的內側部分(圖5、10和11)。橋前膜分隔了橋前池和橋小腦池,當它們向下延伸時變得不那麼突出。
中斜坡入路暴露外展神經池部的全部長度。麵神經和前庭耳蝸神經與腦幹的連接處可見,但大部分神經池段隱藏在岩尖後麵。即使使用橫向角度內窺鏡,也很難看到他們的池段的整個長度(圖11D)。麵神經根出區位於外側中斜坡區,靠近中、下斜坡交界處。由於根出口區位於橄欖上凹,即橋腦髓溝外側邊緣的一個淺凹陷,因此使用45內窺鏡從下斜坡水平方向可以更清楚地觀察到它(圖11H)。鑽孔岩尖下表麵(岩下切開術),打開內聽道前壁,可以暴露整個池長度和部分麵神經和前庭耳蝸神經的口段(圖11F)。
基底下動脈和小腦前下動脈(aica)通常在斜坡中入路暴露。在本研究中,所有20個AICA起源均從基底動脈中斜坡水平處分支。如果起頭是彎曲的基底動脈,它向外側循環進入橋小腦角,則可能需要下岩切開術來顯露起頭和AICA的橋前段。岩石切開術也可能暴露出AICA的出生前和出生前段(圖11F)。盡管異食癖的起源通常位於下斜坡水平,但彎曲異食癖的顱環可能延伸至中斜坡區域。
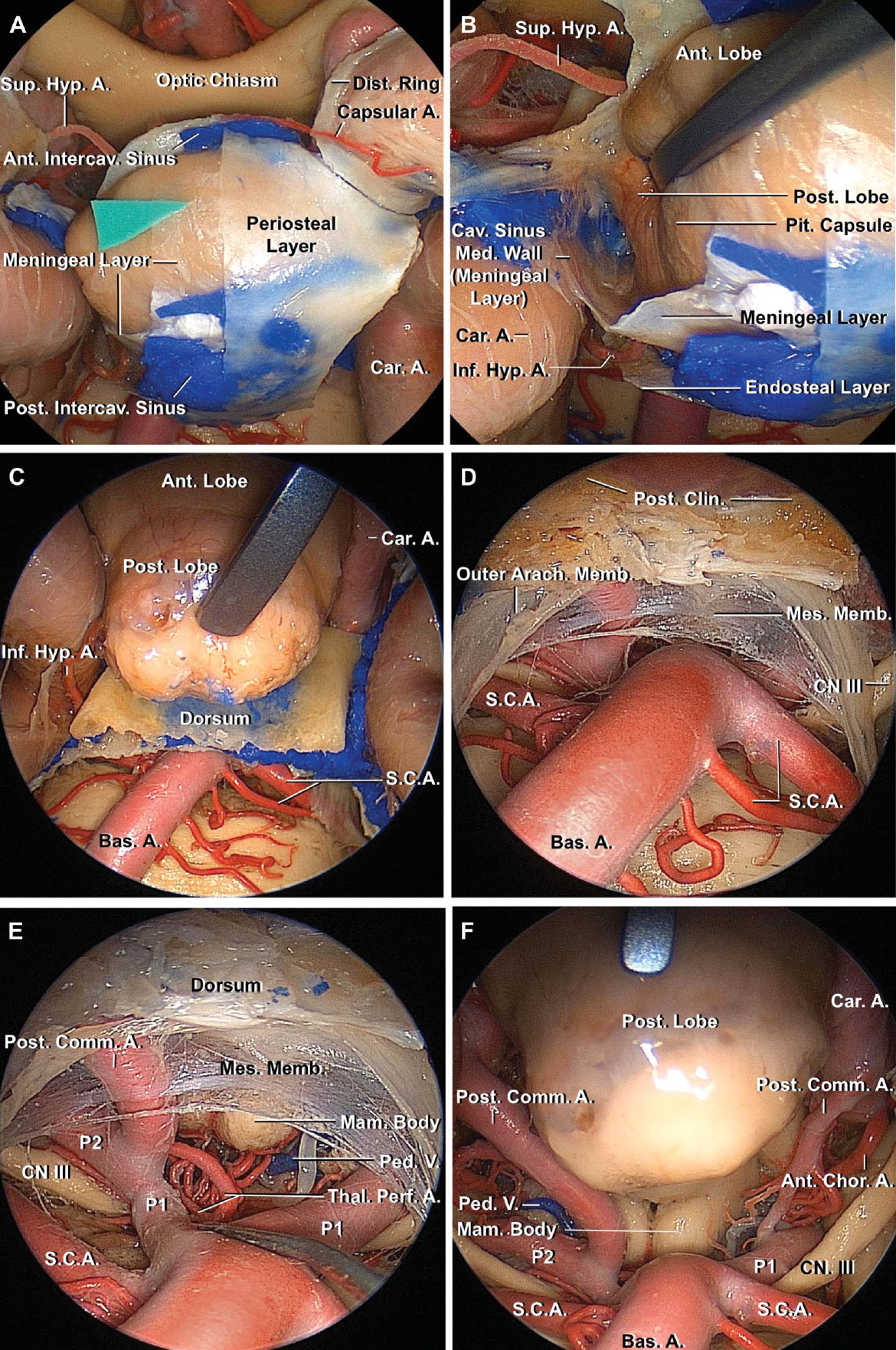
圖8。上斜坡入路延伸至鞍下入路。A,兩層硬腦膜,骨膜和腦膜,排列蝶鞍下垂體。在腦膜層和腦垂體囊之間插入一個三角形的綠色片。硬腦膜的雙層結構在兩層之間的海綿間竇周圍尤為明顯。左頸動脈遠端硬腦膜環已被切開。B,海綿竇內側壁的鞍部與垂體囊分離,前葉向內側縮回露出後葉。海綿竇的內側壁由一層薄薄的腦膜硬腦膜構成。垂體囊緊密地附著在腺體的外表麵。海綿竇內側壁的鞍部覆蓋前葉外側表麵,後葉位於海綿竇內側壁後鞍背凹陷處。 C, 45° endoscope directed superior. The posterior lobe of the pituitary grand has been retracted upward, and the dorsum sellae has been exposed. The posterior lobe sits in the concave anterior surface of the dorsum sellae. The inferior hypophyseal artery arises from the meningohypophyseal trunk and courses medial to supply the posterior lobe. Care is required to avoid avulsion of the inferior hypophyseal artery during transposition of the gland. D, 45° endoscope directed superior. The dorsum sellae has been drilled while preserving the posterior clinoid processes and adjacent part of the dorsum. The mesencephalic leaf of Liliequist’s membrane, which spans the interval between the posterior clinoid process and the pontomesencephalic junction, has been exposed. The mesencephalic membrane is open around the upper the basilar artery. The oculomotor nerves course in the lateral wall of the interpeduncular cisterns and form the pillars to which the leaves of Liliequist’s membrane attach. This specimen has a duplicate left superior cerebellar artery. E, closer view. The contents of the interpeduncular cistern and the origins of the both posterior cerebral arteries can be seen through the large opening in the mesencephalic membrane. The thalamoperforating arteries arise from the P1 and enter the brainstem by passing through the posterior perforated substance in the area behind the mamillary bodies. F, 70° endoscope directed upward showing the anatomic upper limit of the extended upper clival approach. The diencephalic leaf of Liliequist’s membrane has been opened, and the posterior lobe of the pituitary gland has been elevated. The interpeduncular and part of the chiasmatic and carotid cisterns are accessible. The right peduncular vein is exposed lateral to the mamillary bodies. A., artery; Ant., anterior; Arach., arachnoid; Bas., basilar; Car., carotid; Cav., cavernous; Chor., choroidal; Clin., clinoid; Comm., communicating; CN, cranial nerve; Dist., distal; Hyp., hypophyseal; Inf., inferior; Intercav., intercavernous; Mam., mamillary; Med., medial; Memb., membrane; Mes., mesencephalic; Ped., peduncular; Perf., perforating; Pit., pituitary; Post., posterior; S.C.A., superior cerebellar artery; Sup., superior; Thal., thalamo; V., vein.
本文所描述的上、中、下斜坡的定義與我們之前所描述的後窩3個神經血管複合體的概念相吻合,其中斜坡在外展和舌咽部的硬腦膜孔水平被橫線分為3個部分。46、47上、中、下經顱入路可到達3個神經血管複合體的前內側部分。上斜坡入路及其延伸暴露了中腦、橋腦上半部分、SCA以及上神經血管複合體中的動眼神經和三叉神經。中斜坡入路暴露了中神經血管複合體中的橋腦、AICA、外展神經、麵神經和前庭耳蝸神經的下半部分。下斜坡入路暴露下神經血管複合體中的髓質、異食癖、舌咽神經、迷走神經、副神經和舌下神經(圖12)。
即使在神經導航或術中成像係統的輔助下,了解斜外緣和內緣結構之間的關係對斜坡的合適病灶開口也是必不可少的。然而,關於這一課題的研究並沒有解決關於斜坡劃分的爭議。斜坡的水平是根據顱外解剖結構(如蝶竇底)任意分類的。弗雷澤等12、15報道了其病灶入路至斜坡的良好臨床效果,包括術後腦脊液漏發生率較低。他們將斜坡的上三分之一定義為可以通過打開蝶竇接近的部分,而下三分之二包括不打開任何竇即可到達蝶竇底以下的部分。點畫等14還將斜坡分為3部分。我們對這三種經顱入路的定義與他們的一致,包括一個上斜坡區,通過這個區域,腦橋和中腦的上半部分可以通過蝶竇暴露出來。然而,由於蝶竇的肺化程度不同,蝶竇底並不總是劃分上斜坡和中斜坡的合適地標。48本研究為這些解剖學上合理的局灶經骨入路的優秀研究提供了重要信息。
根據病變的位置精心定製的局灶經路可最大限度地減少手術的侵襲性。許多小的或“鎖眼”開顱術的方法已經發展為追求最小的侵入性。49歲的50根據病變是否位於橋小腦角的上、中、下神經血管複合體,乙狀結腸後入路有幾種變體。46Hitotsumatsu等51同時介紹了三叉神經痛、麵肌痙攣和舌咽神經痛的3種不同入路。與這些外科創新一樣,局灶內窺鏡經腔入路能夠有效地接近病灶,同時最大限度地保護顱底。內窺鏡還有助於手術操作,如移除頭長肌的堅韌附件,鑽厚斜坡,控製毗鄰斜坡的各種靜脈叢出血。
以前的一些關於跨界方法的報告顯示了廣闊的全景,但是7、21如此大的暴露可能會增加術後腦脊液漏的風險。各種技術,包括墊圈密封關閉,52球囊支架的使用,53硬膜外(覆蓋)技術,54還有鼻中隔皮瓣,55-58用於重建顱底和硬腦膜缺損,避免腦脊液漏。使用這些新技術,術後腦脊液漏率已降低到0%至9.5%。52歲的54-56使用精心定製的局部穿透照射也可以進一步降低腦脊液泄漏率。
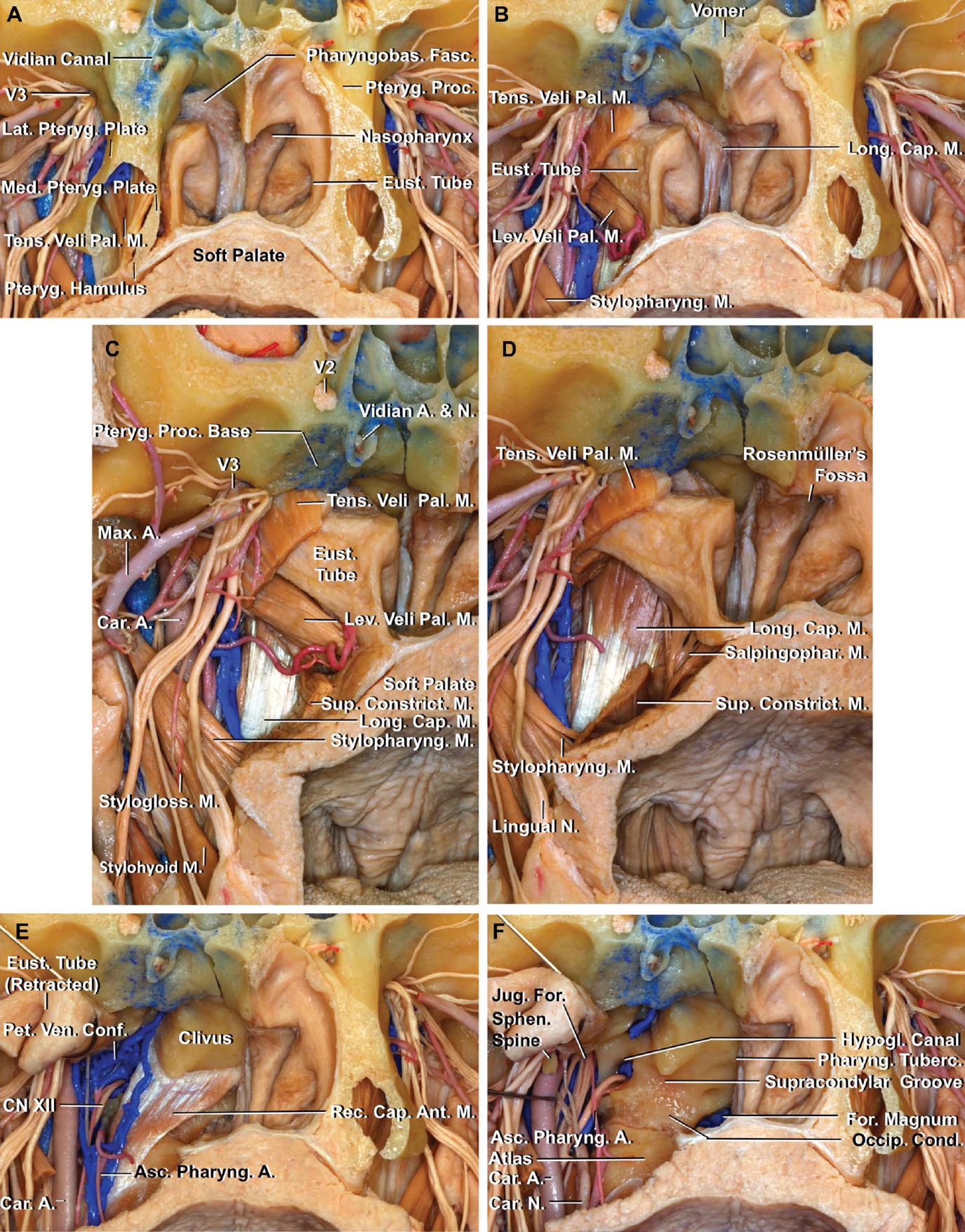
圖9。f。以下斜坡為重點的階梯式解剖。A,鼻咽後壁右半部分的粘膜已經被切除。咽基底筋膜覆蓋頭長肌,與枕骨和顳骨下表麵牢固相連,是打開粘膜後最前麵的一層。齶板張肌沿著咽鼓管軟骨部分的前外側向下並向內側繞過翼內側板的翼鉤,插入軟齶。B,翼突和咽基底筋膜被切除,齶板張肌的中間部分被分割。頭長肌是鼻咽後壁的第二層,附著在咽結節外側的斜坡上。齶提肌在與軟齶相連之前,沿著咽鼓管的下側下降。C、視角聚焦右側。 The superior pharyngeal constrictor muscle, the upper edge of which is located at the C1 level, slightly inferior to the level of the soft palate, inserts into the pharyngeal raphe, which attaches above to the pharyngeal tubercle. The internal carotid artery ascends just lateral to the longus capitis muscle. D, the levator veli palatini has been removed to expose the salpingopharyngeus muscle, which attaches to the inferior part of the cartilaginous eustachian tube, and passes downward to blend with the posterior fasciculus of the palatopharyngeus muscle. E, the right tensor and levator veli palatini and longus capitis muscles have been removed, and the eustachian tube has been detached from the soft palate and retracted laterally. The rectus capitis anterior, located behind the longus capitis muscle, arises on the lateral mass and adjacent part of the transverse process of the atlas and attaches to the anterior surface of the occipital bone above the occipital condyle. The hypoglossal nerve and neuromeningeal branches of the ascending pharyngeal artery course along the lateral edge of the rectus capitus anterior. The petrosal venous confluence is situated lateral and deep to the rectus capitis anterior muscle around the extracranial orifice of the hypoglossal canal and petrosal part of the jugular foramen. F, the rectus capitis anterior muscle and the petrosal venous confluence have been removed. The internal carotid artery has been retracted laterally to expose the anterior edge of the extracranial orifice of the jugular foramen. The supracondylar groove, located just above the occipital condyle, is the site of attachment of the rectus capitis anterior muscle. The pharyngeal tubercle and the anterior edge of the extracranial orifice of the jugular foramen are located at approximately the same level.

圖9。G-L。G,右側下斜坡已經鑽孔同時保留維管,枕骨髁的關節麵,和枕骨大孔的前緣。被岩斜裂、頸靜脈孔和舌下管包圍的三角形區域與頸靜脈結節在顱內表麵的位置相對應。H,放大視圖。下斜坡已在兩側鑽孔。打開下斜坡硬腦膜暴露了髓質和椎體的前表麵,小腦後下和脊髓前動脈。舌咽神經和迷走神經起於橄欖後溝口側舌下小根起端處及後方。這些神經的整個池段可以通過鑽頸靜脈結節暴露出來。 The accessory rootlets are hidden by the hypoglossal canals and the vertebral arteries. I, midsagittal section of another specimen showing the relationship between the posterior nasopharynx and lower clivus. The anterior surface of the clivus leans approximately 45° anterior in the view through the nasal cavity. The posterior nasopharyngeal wall has 3 layers: mucosal, fascial, and muscular. The pharyngobasilar fascia and longus capitis muscles are attached to the clivus; the longus colli muscles are attached to the atlas. The rectus capitis anterior muscle is not shown because the muscle is situated lateral to the midline. J, enlarged view. The pharyngobasilar fascia diminishes in thickness as it descends and gradually blends into the superior pharyngeal constrictor at the level of soft palate. The anterior edge of the pharyngeal tubercle is located at almost the same level as the pontomedullary sulcus. A., artery; Ant., anterior; Asc., ascending; Atl., atlanto; Bas., basilar; Cap., capitis; Car., carotid; CN, cranial nerve; Cond., condyle; Conf., confluence; Constrict., constrictor; Eust., eustachian; Fasc., fascia; Fiss., fissure; For., foramen; Hypogl., hypoglossal; Inf., inferior; Jug., jugular; Lat., lateral; Lev., levator; Long., longus; M., muscle; Max., maxillary; Med., medial; Memb., membrane; Mid., middle; N., nerve; Occip., occipital; Pal., palatini; Pet., petro, petrosal; Petrocliv., petroclival; Pharyng., pharyngeal; Pharyngobas., pharyngobasilar; P.I.C.A., posterior inferior cerebellar artery; Pontomed., pontomedullary; Proc., process; Pteryg., pterygoid; Rec., rectus; Salpingophar., salpingopharyngeus; Sphen., sphenoid; Stylopharyng., stylopharyngeal; Stylogloss., styloglossus; Sulc., sulcus; Sup., superior; Tens., tensor; Tuberc., tubercle; Turb., turbinate; V., vein; Ven., venous; Vert., vertebral.
在防止腦脊液漏方麵,斜坡局灶開口同樣重要,但這不應以血管控製和腫瘤切除為代價。許多斜坡病變如脊索瘤需要切除所有受累組織,包括骨和硬腦膜。一般來說,腫瘤周圍的切緣越寬,複發的幾率越低。這一原則不應為了便於重建而妥協。然而,對於相對較大的病變,可以通過打開斜坡的“上三分之二”或“下三分之二”來優化這一概念,這可能使充分的暴露和最小的侵入。了解斜坡和臨骨區解剖的真正價值在於提供安全的大範圍暴露和通路。即使需要開大斜坡,本研究中顯示的解剖結果也有助於安全有效的暴露。
脊索瘤和軟骨肉瘤累及斜坡,通常經鼻入路。10、12、14應用局灶經皮入路治療這些病變似乎是合理的,因為它們可能發生在不同的斜坡水平,除非病變涉及整個斜坡。洪江等59報道了根據斜坡累及程度改變內鏡入路治療斜坡脊索瘤的方法。此外,脊索瘤也可延伸累及後窩的硬膜內神經血管複合體。Al-Mefty等60手術中發現53%的脊索瘤有硬膜內伸展。在這種情況下,準確了解斜坡受累程度和硬膜內神經血管複合體之間的關係是必不可少的。
前中線區域的其他硬膜內病變,如表皮樣囊腫,11neuroenteric囊腫,8、13腦膜瘤15日,61年像海綿狀畸形這樣的軸內病變可能適合局灶經骨入路。如果動脈瘤是血管內治療的禁忌症,並且在斜坡暴露或附加的血管內技術會影響血流控製,那麼局灶經腔入路可以應用於後窩中線動脈瘤。62年,63年在SCA、AICA和PICA起源處精心挑選的動脈瘤也可以分別通過上、中、下斜坡入路入路。
顱底入路按入路方向分為4組:前入路、前外側入路、外側入路和後入路。2前外側入路包括經海綿狀入路,在這種入路中,前、後斜位切除和鞍背切除聯合眶顴開顱術可切除低處顱底尖或顱底- sca動脈瘤。這種入路也可能暴露在足梗間池和前脊池上緣的病變,主要在同側,64年,65年與上斜坡的部分區域相對應。
外側入路包括顳下前經岩路、迷路路、耳蝸路以及幕上和幕下乙狀竇前聯合入路。經岩前入路或Kawase入路到達上斜坡區同側半部分,同側三叉神經水平以下暴露有限,包括中斜坡區的部分但不是全部同側半部分。3, 66經迷路和經耳蝸入路是乙狀竇前入路的改進,將手術視野進一步向中線延伸。經耳蝸入路可以看到內聽道內側的外展神經、三叉神經下緣、進入頸靜脈孔的神經、基底動脈的一段,以及AICA的起源和起始段,3.接近整個同側中斜坡區域。幕上和幕下乙狀竇前聯合入路使岩石斜坡區從中窩和幕下切肌到頸靜脈球顯露出來。3.因此,暴露不僅覆蓋同側上、中斜坡區,還包括下斜坡區的上半部分,但如果不增加經耳蝸暴露,接近中線是困難的。經耳蝸暴露改善了通往腦幹、斜坡和基底動脈前部的通道,但這樣做的代價是暫時或永久的麵癱和聽力喪失。
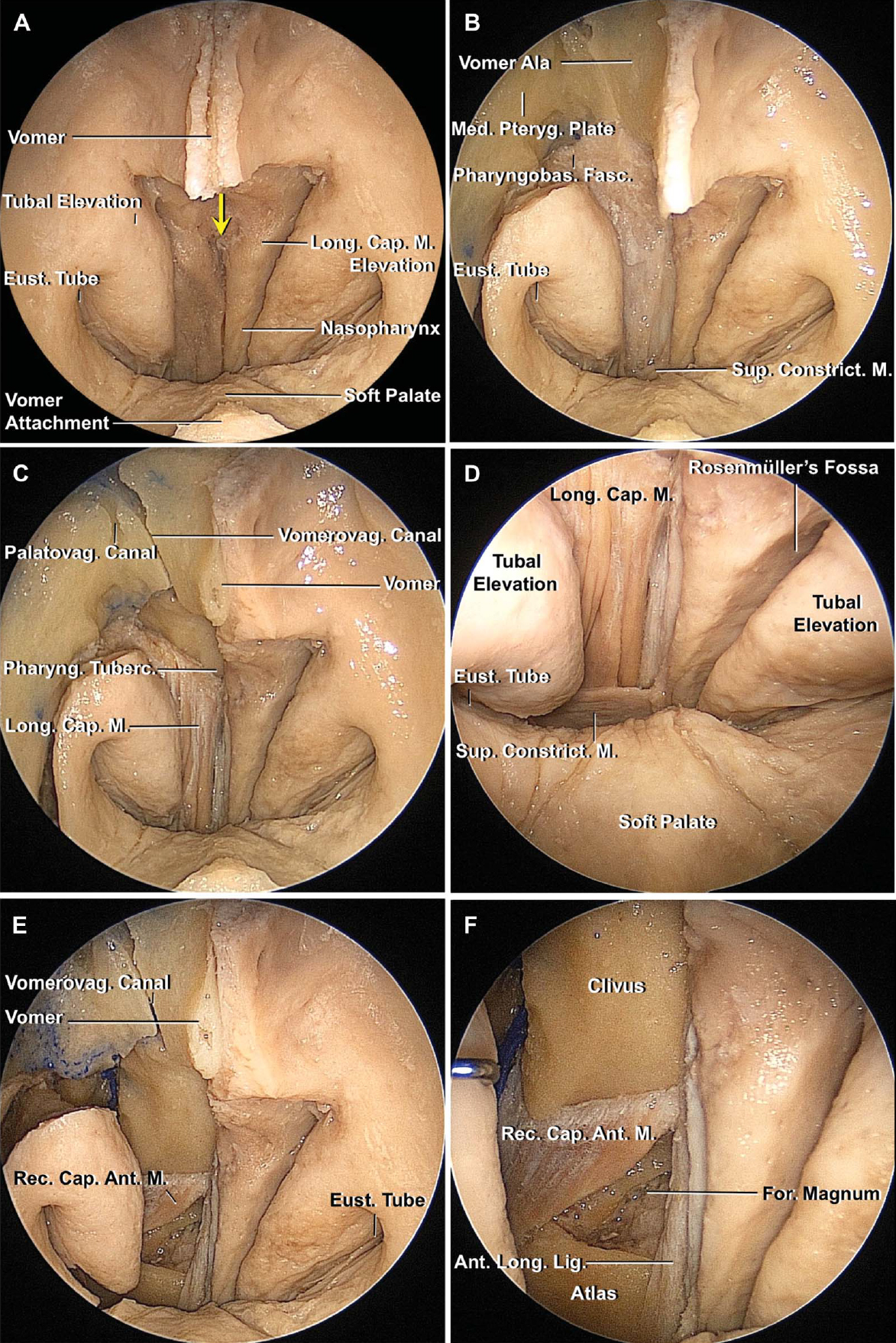
圖10。f。內窺鏡入路至下斜坡。A,通過下鼻道引入內窺鏡觀察鼻咽後壁。鼻中隔的後部已從蝶脊上分離並切除。鼻咽後壁右半部分的粘膜已被切除。咽鼓管在鼻咽部的側壁上打開,就在突出而穩固的咽鼓管凸起的前方。頭長肌插入斜坡處,通常在粘膜表麵可見v型隆起。咽結節位於V(黃色箭頭)的下緣。在頭長肌插入處上方的粘膜上有一個淺的倒三角形凹陷,與兒童咽扁桃體或腺樣體的位置相對應。 B, the nasopharyngeal mucosa on the right side has been removed. The pharyngobasilar fascia covers the longus capitis muscle and attaches firmly to the inferior surface of the occipital and temporal bones. As the fascia descends, it diminishes in thickness and gradually blends into the superior pharyngeal constrictor at the level of soft palate. At its upper edge, the pharyngobasilar fascia blends with the fibrocartilage around the border between the sphenoid and occipital bones and foramen lacerum. C, the pharyngobasilar fascia on the right side has been removed to expose the longus capitis attachment to the clivus lateral to the pharyngeal tubercle. This specimen has a vomerovaginal canal that shares its anterior end with the palatovaginal canal. The vomerovaginal canal is positioned between the vaginal process of the sphenoid and the ala of the vomer. D, 45° endoscope directed inferior. The upper edge of the superior constrictor is located at the C1 level at the border between the oropharynx and nasopharynx and is not usually opened for exposure of the lower clivus. The fossa of Rosenmüller projects laterally from the posterolateral corner of the nasopharynx behind the tubal elevation. The parapharyngeal segment of the internal carotid artery courses just deep to the lateral limit of the fossa of Rosenmüller. E, the longus capitis muscle and pterygoid process on the right side have been removed to expose the rectus capitis anterior muscle. F, closer view. The rectus capitis anterior is a short, flat muscle that extends across the atlanto-occipital joint and connects to the lateral mass of the atlas and the basal part of the occipital bone.

圖10。G-L。G,右頭前直肌已被切除。鼻咽後黏膜與咽結節的關係。H,剩下的鼻咽後壁和翼突已經被切除。下岩斜坡靜脈沿岩斜坡裂隙顱外表麵走行。I,在咽鼓管軟骨部上方插入45°內窺鏡,並向外側觀察頸靜脈孔及其鄰近區域。岩下竇下端的岩靜脈彙合處連接舌下管的靜脈叢和椎前靜脈叢。在這個標本中,靜脈彙流在頸靜脈孔顱外孔下方通過舌咽神經和迷走神經之間靜脈壁的開口流入頸內靜脈的內側。岩斜坡下靜脈也流入岩靜脈彙合處。 J, some of the petrosal venous confluence has been removed to expose the jugular foramen. The glossopharyngeal nerve exits the jugular foramen along the anterior wall of the internal jugular vein, whereas the vagus and accessory nerve exit along the medial venous wall. The neuromeningeal branch of the ascending pharyngeal artery gives rise to the hypoglossal and jugular branches just below the jugular foramen. Both branches penetrate the petrosal confluence and enter the hypoglossal canal and the jugular foramen to supply the surrounding dura. K, anterior view of the clivus.

圖10。mp。L,右下斜坡已經鑽孔露出髓質。下斜坡上緣位於咽結節頂部上方約4mm處。M,下坡的其餘部分已經鑽好了同時保留舌下管。暴露的部分包括髓質的前部;舌咽神經、迷走神經、副神經、舌下神經和C1神經;還有脊椎,小腦後下動脈,脊椎前動脈。N,右側近景。舌下小根沿橄欖前溝生長,通常經過椎動脈後方。 The posterior inferior cerebellar artery arises near the junction of the hypoglossal rootlets with the medulla. The glossopharyngeal, vagus, and accessory nerves arise behind the hypoglossal rootlets, as a line of rootlets originating from the retro-olivary sulcus, a shallow groove between the olive and the posterolateral surface of the medulla. The rostral part of the accessory nerve is hidden by the hypoglossal canal and vertebral artery. O and P, another lower clival region. O, the lower clivus and hypoglossal canals have been drilled. P, closer view of the right side. A., artery; A.I.C.A., anterior inferior cerebellar artery; Ant., anterior; Asc., ascending; Atl., atlanto; Bas., basilar; Cap., capitis; Car., carotid; Constrict., constrictor; Cer., cerebellar, cerebello; CN., cranial nerve; Cond., condyle; Conf., confluence; Eust., eustachian; For., foramen; Hypogl., hypoglossal; Inf., inferior; Jug., jugular; Lat., lateral; Lig., ligament; Long., longus; M., muscle; Med., medial, medullary; Mid., middle; N., nerve; Occip., occipital; Palatovag., palatovaginal; Ped., peduncle; Pet., petro, petrosal, or petrous; Petrocliv., petroclival; Phayrng., pharyngeal; Pharyngobas., pharyngobasilar; P.I.C.A., posterior inferior cerebellar artery; Pontomed., pontomedullary; Pteryg., pterygoid; Rec., rectus; Sulc., sulcus; Sup., superior; Trans., transverse; Tuber., tubercle; V., vein, Ven., venous; Vert., vertebral; Vomerovag., vomerovaginal.
後入路包括乙狀竇後入路和遠外側入路。乙狀竇後肌提供了從滑車神經和三叉神經到副神經和舌下神經的通道。然而,乙狀結腸後暴露的中心是橋小腦角,內聲入口內側結構的暴露與乙狀結腸前入路的迷路後或迷路外一樣有限。3.基本的遠外側入路的特點是沿顱頸連接處後外側切開肌肉,早期識別顱外椎動脈,並進行延伸至枕骨大孔至同側枕骨髁後緣的枕下開顱術或開顱術。這種入路可以通過髁上、髁上和髁旁的延伸來擴展,從而擴展到下斜坡和髓前區。4、6
前路顯微外科入路包括經顱-經基底、額部延伸和經口入路。經顱-經基底入路包括保留眶上緣的雙額開顱術,通過篩竇、蝶竇、蝶鞍和斜坡進入腦幹。67額部延伸入路與經顱-經基底入路相似,不同之處在於它包括眶額篩骨切開術。枕骨大孔可通過經顱-基底和額部延伸入路進入。雖然這兩種入路幾乎都能到達整個斜坡,但在經顱-經基底入路中,鞍下硬腦膜的鼓脹隱藏了鞍下區域。2鏡下或內鏡經口入路可提供從下斜坡到C3下椎體的通路。21
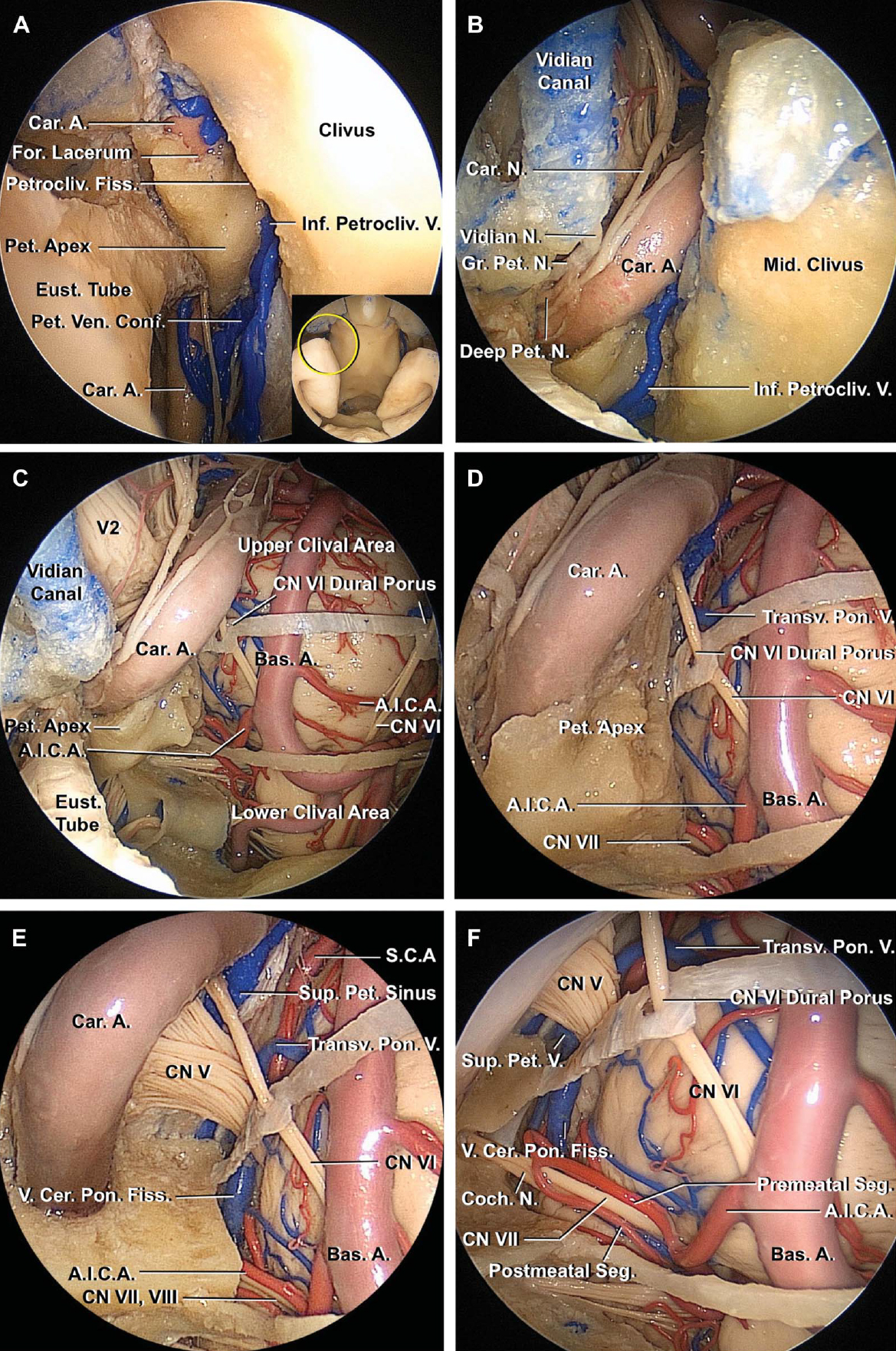
圖11。f。內窺鏡入路至中斜坡。A,視野聚焦於中斜坡和淚孔,45°內窺鏡向外側定向。插圖中的黃色圓圈表示內窺鏡視野。翼狀突已被切除。一些填充撕裂孔下部的纖維軟骨被切除以露出頸岩的前膝。維神經隱藏在撕裂孔前外側邊緣的纖維軟骨中。第二,維甸運河已經被削成了骷髏。維底管是維底動脈和神經的通道,向後打開,進入前外側邊緣的上半部分,直達淚孔。 The deep petrosal branch of the carotid sympathetic plexus joins the greater petrosal nerve at the foramen lacerum near the posterior opening of the vidian canal to form the vidian nerve. The upper end of the inferior petroclival vein connects through the foramen lacerum with the venous plexus around the carotid artery or with the cavernous sinus. The trapezoid-shaped middle clivus is bordered laterally by the foramen lacerum and internal carotid artery in the upper part and by the petroclival fissure in the lower part. C, right lateral part of the middle clival area. The right inferior petrosal sinus and adjacent dura have been removed. A thin dural bridge sits at the junction of the upper and middle clivus, and a thin bony bridge separates the middle and lower clivus. The lower part of the pons, basilar and anterior inferior cerebellar arteries, and cisternal part of the abducens nerves are exposed. D, closer view with the 45° endoscope directed laterally. All the cisternal segment of the facial nerve, except the origin, is hidden by the petrous part of the temporal bone. It is difficult to see the whole cisternal segment even with the angled endoscope directed laterally. E, the petrous apex and bone below the distal carotid canal have been removed to expose more of the cisternal segment of the facial and vestibulocochlear nerves. The posterior root of the trigeminal nerve passes forward below the superior petrosal sinus. F, more of the temporal bone below the carotid canal and trigeminal nerve has been drilled. The anterior wall of the internal acoustic meatus has been opened to expose the cisternal and meatal segments of the facial and vestibulocochlear nerves, as well as the premeatal and postmeatal segment of the anterior inferior cerebellar artery.

圖11。G-H。G, 45°內窺鏡向外側觀察麵神經近端橋小腦角。圖中黃圈為內鏡視野。麵神經在中斜坡區域的下外側。H, 45°內窺鏡近景。內窺鏡已被引入的水平下斜坡和定向上。麵神經根出口區(箭頭)比G圖中更清晰,因為根出口區位於橄欖上窩,是橋髓溝外側邊緣的一個淺凹陷。一個,動脈;A.I.C.A,小腦前下動脈; Bas., basilar; Car., carotid; Cer., cerebello; Chor., choroid; CN, cranial nerve; Coch., cochlear; Conf., confluence; Eust., eustachian; Fiss., fissure; For., foramen; Gr., greater; Inf., inferior; Mid., middle., N., nerve; Ped., peduncle; Pet., petro, petrous, petrosal; Petrocliv., petroclival; Plex., plexus; Pon., pontine; S.C.A., superior cerebellar artery; Seg., segment; Sup., superior; Transv., transverse; V., vein; Ven., venous.

圖12。斜坡每一段與rhoton定義的後窩神經血管複叢之間的關係。46上斜坡入路暴露了上神經血管複叢的前部,包括中腦和橋腦的鄰近部分、小腦上動脈、動眼神經和三叉神經。中斜坡入路暴露了中神經血管複叢的前部,包括腦橋的下半部分、小腦前下動脈、外展神經、麵神經和前庭耳蝸神經。下斜坡入路暴露了下神經血管複叢的前部,包括髓質、小腦後下動脈、舌咽神經、迷走神經、副神經和舌下神經。AICA,小腦前下動脈;CN,顱神經;異食癖,小腦後下動脈;SCA,小腦上動脈。
與經鼻入路相比,腦池內側V、VII、VIII和IX的外側和後側入路受限。也有額外的風險從外側和後方接近中線結構通過在腦幹產生的腦神經束之間和中間工作。如本研究所示,transtransapproach的優點是提供更好的曝光和中線結構的直接正麵視圖。相比之下,經鼻入路如果通過神經束從內側到外側的工作到達顱神經外側的病變,則可能麵臨類似的風險。局灶內窺鏡經鼻經道入路應被視為其他顱底手術的補充路徑,入路的選擇應基於病灶的位置(特別是參考顱神經)、延伸和病灶的性質。
斜坡由兩個顱內標誌分為上、中、下三個部分:外展神經的硬腦膜孔和舌咽肌。咽結節和頸動脈下緣位於維管後開口上方4.9 mm處,是經鼻內窺鏡入路進入斜坡各分支的重要顱外外科標誌。經鼻經鼻入路可以精心定製,以處理涉及斜坡和後窩鄰近部分的局灶性病理。
財政支持由佛羅裏達大學基金會提供。作者在本文中描述的任何藥物、材料或設備中沒有個人財務或機構利益。
貢獻者:Takeshi Funaki, MD, Toshio Matsushima, MD, Maria Peris-Celda, MD, PhD, Rowan J. Valentine, MD, Wonil Joo, MD,和Albert L. Rhoton, Jr, MD
內容來自Funaki T, Matsushima T, Peris-Celda M, Valentine RJ, Joo W, Rhoton AL, Jr.局部經鼻入路至上、中、下斜坡。③Neurosurg(黑格)2013; 73: ons155-ons191。doi.org/10.1227/01.neu.0000431469.82215.93.經牛津大學出版社代表神經外科醫師協會批準。©神經外科醫生協會。
神經外科188bet手机app圖譜很榮幸能夠繼承Albert L. Rhoton, Jr . MD的遺產。
請登錄發表評論。
一定要在社交媒體上關注我們,獲取精彩內容並保持更新生活科恩醫生的會議,關於手術技術的問題,以及更多!



您必須登錄才能查看此材料。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
現在請捐!
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。請承諾每年至少捐贈250美元給Atlas。
如果沒有這個承諾,Atlas將很快需要付費訂閱世界上許多病人的護理都依賴於它的外科醫生將無法使用它。現在請捐!