

你可以有所作為。
的188bet手机app幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈我們無法繼續製作《地圖集》。
請承諾每年至少向Atlas捐贈250美元。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法使用它,他們的病人的護理依賴於它。
請立即捐款!
最後更新:2021年4月8日
摘要目的:治療位於顱脊交界處(CVJ)前部的病變仍然是一個具有挑戰性的神經外科問題。本研究的目的是檢查CVJ硬膜外前側的顯微外科解剖,以及遠外側和極外側寰枕經關節入路所獲得的暴露的差異。遠外側入路,如最初所述,是一種枕下外側入路,位於胸鎖乳突肌和椎動脈後方,枕骨和寰枕髁和寰枕關節內側。極外側入路,如最初所述,是一種直接外側入路,深入胸鎖乳突肌的前部,在頸內靜脈後麵,沿椎動脈的前部。兩種入路均可鑽寰枕關節處的髁突,但由於入路方向不同,暴露方式不同。
方法: 15例成人屍體標本經彩色矽膠灌注動脈和靜脈後,使用×3至×40的放大鏡進行研究。在逐步解剖中檢查了CVJ硬膜外部分和兩個寰枕經關節入路的顯微外科解剖。
結果:寰枕遠外側經關節入路能很好地暴露位於CVJ硬膜外區域同側前方和前外側的硬膜外病變。寰枕極外側經關節入路提供了良好的暴露,不僅在暴露的一側,而且還跨越中線延伸到對側寰枕關節內側和下斜坡。
結論:寰枕經關節入路的遠外側和極外側變體提供了經口入路到CVJ前硬膜外結構的另一種選擇。與經口入路相比,兩種入路均縮短了手術路徑,避免了汙染鼻咽,減少了腦脊液漏的發生率,且不受寰枕關節外側的限製。
顱脊交界處(CVJ)前部硬膜外病變的直接手術入路仍然是一個挑戰,因為其位置較深,該區域的重要神經結構,以及它們與椎動脈和鼻咽的關係。CVJ是腫瘤、血管性、創傷性、先天性和退行性病變的常見部位,這些病變可從前路、後路或外側入路(6,20)(圖1、a和B)。前路入路主要用於位於CVJ前部的硬膜外病變,有明顯的缺點,包括視野汙染和腦脊液瘺的發生頻率、寰枕關節限製的外側暴露、手術野深度(5,12,17)。對於大多數硬膜內病變,尤其是頸髓交界處外側或後方的病變,首選後路入路(22)。遠外側經髁入路和極外側經髁入路都為前外側CVJ硬膜內病變提供了良好的手術通路(3,4,9,13,19,23,24,27),但它們也可用於到達前硬膜外病變(圖1,C-H)。本研究的目的是檢查CVJ前部的顯微外科解剖,尤其關注硬膜外間隙,並檢查寰枕經關節變異型遠外側和極外側入路所獲得的前硬膜外暴露的程度。

圖1所示。CVJ前部硬膜外病變的手術入路。A和B(放大視圖),前經口入路(白色箭頭)和後、遠外側和極外側入路(藍色箭頭)。寰枕經關節入路至CVJ前硬膜外病變顯示在其餘圖中。C, E, G,圖集上表麵的上方視圖。D, F, H,枕骨和枕骨大孔的下視圖。A和B, CVJ前部的硬膜外區由枕骨、寰椎、軸及其相關關節和韌帶組成。C和D,右側遠外側入路(紅色箭頭)和左側極外側入路(黃色箭頭)寰枕經關節入路方向。E和F,遠側寰枕經關節入路可進入CVJ的前部或前外側,包括齒狀突和同側下斜坡。紅色圓圈區域表示鑽穿寰髁和齒狀突(E)和枕髁(F)的範圍。G和H,極外側寰枕經關節入路進入CVJ前部,包括齒狀突、下斜坡和側側寰枕關節內側表麵。黃色圓圈區域表示寰突和齒狀突(G)和枕骨髁(H)的鑽孔程度。前; Cond., condyle; Cruc., cruciform; Horiz., horizontal; ICA, internal carotid artery; Lat., lateral; Lig., ligament; Occip., occipital; Post., posterior; Proc., process; PLL, posterior longitudinal ligament; Trans., transverse; VA, vertebral artery. (Images courtesy of AL Rhoton, Jr.)
使用15具成人屍體標本,放大×3至×40,逐步解剖遠外側和極外側入路寰枕關節變異體及相關解剖。動脈和靜脈灌注了彩色矽膠。用Midas Rex鑽頭(Fort Worth, TX)進行骨解剖。
在規劃CVJ區域入路時必須考慮的骨結構是枕骨、寰椎和軸。
枕骨.枕骨環繞枕骨大孔。椎間孔開口呈橢圓形,後寬於前。枕骨分為位於枕骨大孔前的基底部、枕骨枕骨大孔外側的成對髁突部和枕骨枕骨大孔上方及後方的鱗狀部。
枕骨的基底部分,也被稱為斜坡,是一塊向前和向上延伸的厚的四邊形骨板。它在蝶枕軟骨聯合處與蝶骨相連就在鞍背下方。斜坡的上表麵是左右凹的,並由岩石斜坡裂縫在每一側與顳骨的岩石部分分開。在枕骨大孔前基底部的下表麵,有一個小突起,即咽結節,與咽的纖維縫相連。
成對的髁突位於枕骨大孔的外側。枕骨髁與寰椎相連,從這些部位的外表麵突出。髁狀突位於枕骨大孔前半段外側。它們呈橢圓形,向下凸,麵朝下和橫向,長軸指向前方和內側。結節附著於齒狀突的鼻翼韌帶,位於每個髁突的內側。傳遞舌下神經的舌下管位於髁上,可被骨隔部分或完全分割。髁突窩是位於髁突後外表麵的一個凹陷,常穿孔形成髁突後管,通過髁突後管有導靜脈連接椎靜脈叢和乙狀竇。
鱗狀部分是位於枕骨大孔上方和後麵的一個內部凹板。它包含幾個突起,如枕外隆突和脊,包括頸部眾多肌肉附著的頸線(圖2)。
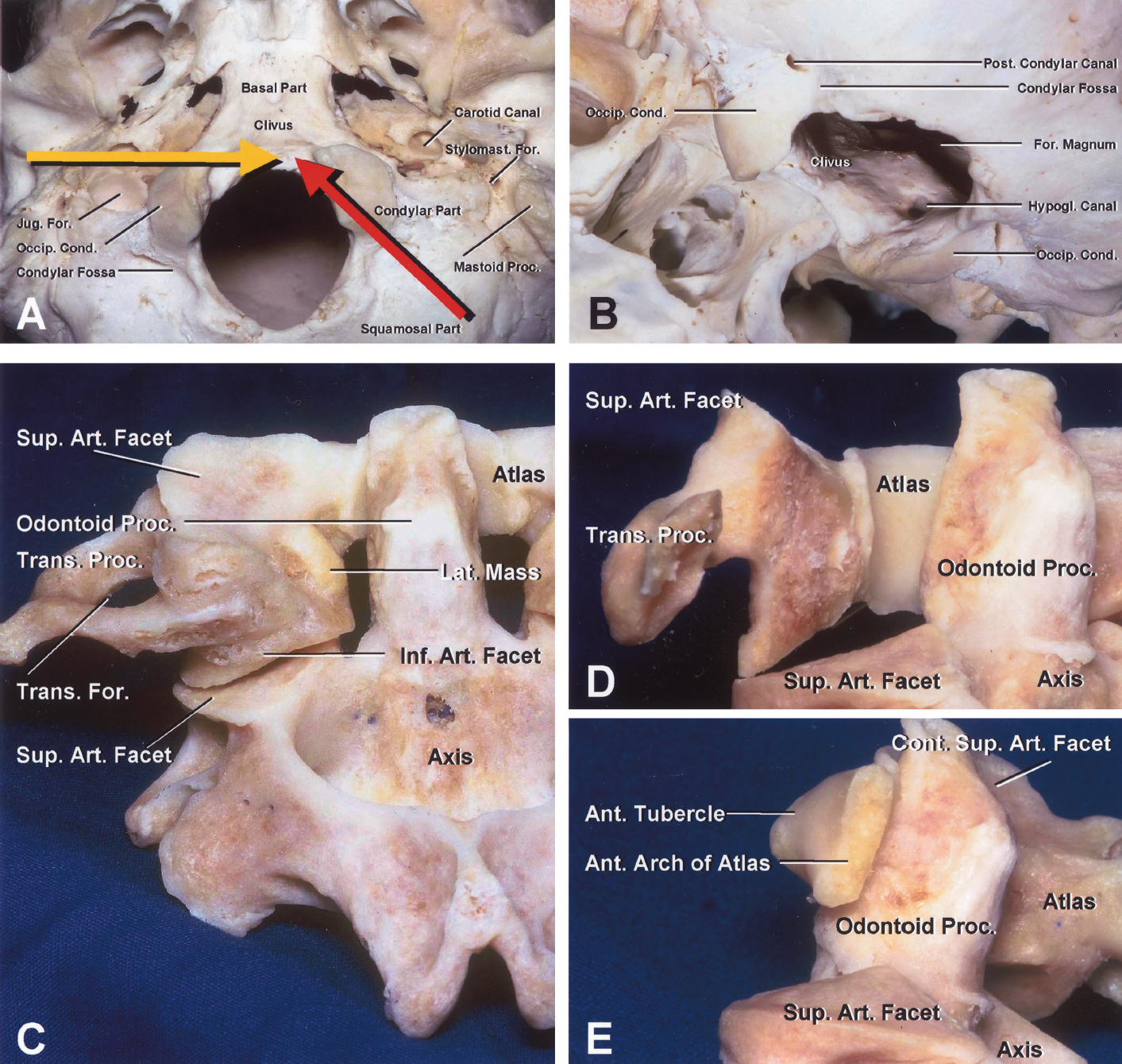
圖2。枕骨(A和B)和寰樞複合體(C-E)。一、自卑觀;B、左側後斜位視圖;C,後視圖;D,遠側入路提供的視圖;E,極側入路提供的視圖。A,枕骨圍繞著橢圓形的枕骨大孔。枕骨分為位於枕骨大孔前的基底部(斜坡部)、枕骨大孔外側的成對髁突部和枕骨大孔上方及後方的鱗狀部。枕骨的基底部,也被稱為斜坡,是一塊厚的四角形骨板,向前向上延伸,在鞍背下方與蝶骨相連。枕骨的髁部,也就是枕骨髁所在的位置,位於外表麵枕骨大孔前半部分的外側。 Arrows show the direction of the far lateral (red) and extreme lateral (yellow) atlanto-occipital transarticular approaches. B, left oblique view directed through the foramen magnum from the left side to show the intracranial aspect of the right hypoglossal canal situated above the condyle. The condylar fossa is located behind the condyle and may open into the condylar canal, through which an emissary vein passes. The condyles block access to the anterior aspect of the foramen magnum. C, a laminectomy of the atlas exposes the relationships among the lateral mass, transverse process of the atlas, and odontoid process. D, far lateral approach to the dens. The posterior parts of the lateral mass of the atlas and the transverse process have been drilled away. This approach provides the shortest route to the dens but does not gain the clearest contralateral view. E, extreme lateral approach to the dens. This approach accesses the entire odontoid process and the medial surface of the contralateral atlanto-occipital joint from a lateral perspective. Ant., anterior; Art., articular; Cond., condyle; Cont., contralateral; For., foramen; Hypogl., hypoglossal; Inf., inferior; Jug., jugular; Lat., lateral; Occip., occipital; Post., posterior; Proc., process; Sup., superior; Stylomast., stylomastoid; Trans., transverse. (Images courtesy of AL Rhoton, Jr.)
地圖集和軸心的綜合體.寰椎是第一頸椎,與其他頸椎不同的是它呈環狀,沒有椎體和棘突。它由兩個位於環前外側的厚側塊組成。側塊前麵由短的前弓連接,後麵由長而彎曲的後弓連接。通常椎體的位置被軸的齒狀突所占據。前弓前凸並有前正中結節。後弓向後凸起,在其上外表麵外側有一個中間的後結節和一個椎動脈通過的槽。每個側塊的上表麵有一個向上和內側的橢圓形凹麵,並與向下和外側的枕骨髁相連。每個側塊的下表麵有一個圓形、平麵或略凹的麵,朝下、向內、略向後,與軸的上關節麵相連。每個側塊的內側都有一個小結節,用於附著在齒狀突後麵的寰椎橫韌帶上。 Each transverse foramen is situated between the lateral mass and the transverse process and transmits a vertebral artery. Note that the cervical spinal cord is located at the level of the posterior margin of the lateral mass.
軸,即第二頸椎,比寰椎更接近於典型的椎體,但它與從身體向上突出的齒狀突(齒狀突)有區別。齒突的前部是關節突,它與寰椎前弓背部的關節突形成關節。齒狀突的頂端呈尖狀,由根尖韌帶連接;齒狀突的一側為扁平,與鼻翼韌帶相連;齒狀突的後表麵底部為凹槽,與寰椎橫韌帶相連。齒突和身體兩側有一對巨大的橢圓形切麵,從身體橫向延伸到椎弓根的毗鄰部分,並與寰椎的下切麵相連。身體的前部在頸長肌連接區域的中線兩側被挖空。頸椎軸的椎板比其他頸椎的椎板更厚,椎弓根更粗壯,棘突更大(圖3)。

圖3.地圖集和軸。一、視野優越;B,前視圖;C,後視圖;D,左斜後視圖;E,右側視圖。A,寰椎由兩個位於前外側的厚側塊組成,前麵由短的前弓連接,後麵由較長的彎曲後弓連接。每個側塊的內側有一個小結節,用於連接寰椎橫韌帶,它經過齒狀突的後方。前弓前凸並有前正中結節。 The position of the vertebral body is occupied by the odontoid process of the axis. Note that the posterior margin of the lateral mass is located lateral to the anterior part of the spinal cord. B, the axis is distinguished from the typical vertebrae by the odontoid process (dens), which projects upward from the body. On the front of the dens is an articular facet that forms a joint with the facet on the posterior surface of the anterior arch of the atlas. The dens and body are flanked by paired large oval facets that extend laterally from the body onto the adjoining parts of the pedicles and articulate with the inferior facets of the atlas. The anterior aspect of the body is hollowed out on each side of the midline in the area where the longus colli muscles attach. C, D, and E, the posterior arch of the atlas is convexed backward and has a median posterior tubercle and a groove on the lateral part of its upper-outer surface in which the vertebral artery courses. The upper surface of each lateral mass has an oval concave facet that faces upward and medially and articulates with the occipital condyle, which faces downward and laterally. The dens has a pointed apex that is joined by the apical ligament and flattened sides where the alar ligaments are attached. The lamina of the axis is thicker than any other cervical vertebrae, and the spinous process is larger. The C2 nerve emerges between the posterior arch of the atlas and the lamina of the axis. Distal to the ganglion, the nerve divides into larger dorsal and smaller ventral rami. Ant., anterior; Art., articular; Cruc., cruciform; Dors., dorsal; Horiz., horizontal; Inf., inferior; Lat., lateral; Lig., ligament; Post., posterior; Proc., process; Sup., superior; Trans., transverse; VA, vertebral artery; Vent., ventral. (Images courtesy of AL Rhoton, Jr.)
寰樞關節.寰椎和軸的關節包括四個滑膜關節:齒突前後的兩個正中關節和寰椎和軸側塊相對關節麵之間的成對外側關節。中間關節位於齒狀突的前後,有自己的纖維囊和滑膜腔。前突位於齒狀突的前表麵和寰椎前弓的後側麵之間。後側滑膜腔更大,位於軟骨覆蓋的寰椎橫韌帶前表麵和齒狀突後表麵之間。
寰椎和樞椎由十字韌帶、前後縱韌帶和圍繞在側塊上相對關節麵之間的關節囊連接。交叉韌帶有橫向和垂直的部分,在齒突後麵形成交叉。橫向部分稱為橫韌帶,是一條粗而結實的帶,在齒狀突後拱過寰椎環,並將椎管分為包含硬腦膜和脊髓的較大後腔室和包含齒狀突的較小前腔室。
在腹表麵,寰椎和軸由前縱韌帶連接,前縱韌帶是固定在寰椎前弓下緣上方和軸體前方下方的一條寬寬的韌帶。後縱韌帶下方附著於軸體後表麵,上方附著於交叉韌帶的橫向部分和斜坡(圖3和圖4)。

圖4。CVJ前麵的硬膜外區域。A-G,後視圖;H,逐步解剖的側位視圖。A,小腦扁桃體位於枕骨大孔上方。椎動脈在寰枕關節水平穿入硬腦膜,並在齒狀韌帶和副神經前通過枕骨大孔上升。B,髓質的下部和頸脊髓的上部已經被切除以暴露CVJ的前部。硬腦膜位於脊髓的前麵。通過硬腦膜可以看到位於硬腦膜下方的椎靜脈叢。C,硬腦膜被切除以暴露蓋膜,這是後縱韌帶的口側延伸。D,蓋膜被移除以暴露十字韌帶和鼻翼韌帶。 The horizontal portion of the cruciform ligament, called the transverse ligament of the atlas, extends laterally to attach to the medial edges of the lateral masses of the atlas, and the vertical portion ascends to attach to the anterior margin of the foramen magnum deep to the tectorial membrane. The alar ligaments pass upward and laterally and attach to the lateral edges of the occipital condyle. E, the cruciform and alar ligaments have been removed to expose the dens. The apical ligament of the dens extends upward to attach to the margin of the foramen magnum. F, the transatlantal approach. The left lateral mass of the atlas has been removed. G and H, the atlantooccipital transarticular approach. The inferior surface of the occipital condyle has been removed to show the increased access to the odontoid process provided by the far lateral approach (G) and extreme lateral approach (H). A-O, atlanto-occipital; Ant., anterior; Art., articular; Cap., capitis; CN, cranial nerve; Cond., condyle; Cruc., cruciform; Dent., dentate; Dors., dorsal; Horiz., horizontal; Int., internal; Jug., jugular; Lig., ligament; Long., longus; M., muscle; Memb., membrane; Occip., occipital; P.I.C.A., posteroinferior cerebellar artery; Post., posterior; Proc., process; Sup., superior; Trans., transverse; V., vein; VA, vertebral artery; Vent., ventral. Vert., vertical. (Images courtesy of AL Rhoton, Jr.)
寰枕關節.寰枕骨和枕骨由寰枕關節周圍的關節囊和寰枕前膜和枕後膜連接。寰枕前膜附著於枕骨大孔前緣上方,寰枕前弓上緣下方,寰枕關節囊外側。寰枕後膜是一層薄膜,上麵與枕骨大孔的後緣相連,下麵與寰枕後弓的上緣相連。膜的外側邊界是自由的,拱在椎動脈和頸第一神經根後麵。該膜的外側邊緣可能在其拱起椎動脈後側的區域發生骨化,從而在寰枕關節內側的動脈周圍形成部分或完整的骨環(圖4A)。
軸和枕骨.四條纖維帶——蓋膜、成對的鼻翼韌帶和根尖韌帶——連接軸和枕骨。蓋膜是後縱韌帶的頭側延伸,覆蓋齒狀突和交叉韌帶。它連著軸體的後表麵,連著枕骨上表麵枕骨大孔前,連著寰枕關節內側外側。鼻翼韌帶是兩條強壯的韌帶,出現在齒狀突上部的兩側,並斜向上外側延伸,附著於枕髁的內側表麵。齒狀突尖韌帶從齒狀突尖端延伸至枕骨大孔前緣,位於寰枕前膜和交叉韌帶上延之間(圖4,C-E)。
脊髓。脊髓被硬脊膜包圍,位於橫韌帶後麵椎管的後部。脊髓與髓質融合在一個任意設定的水平上位於形成第一頸神經的背側和腹側細根的上限。在腹側比背側更容易鑒別,因為第一頸神經的腹側小根總是存在,而在許多情況下背側小根不存在。脊髓和髓質的交界處位於第一頸根的吻側邊緣,這意味著髓質而不是脊髓占據了枕骨大孔(圖3A和4A)。
每個背側根和腹側根由一係列6到8個小根組成,分別扇形進入脊髓的後外側和前外側表麵。背根和腹根分別穿過蛛網膜下腔和硬腦膜的橫切麵,然後在椎間孔附近彙合形成脊神經。枕骨大孔區域的細根幾乎直接橫向穿過到達硬腦膜孔。背根的神經元聚集在一起形成神經節,位於背根和腹根交界處的近端;然而,第一頸背根和相關的神經節可能缺失。C1, C2和C3神經,遠端神經節,分為背支和腹支。背支分為內側支和外側支,支配頸部後部的皮膚和肌肉。C1神經,稱為枕下神經,位於枕骨和寰椎之間的椎管,有一個比腹側支大的背側支。背支位於寰椎後弓和椎動脈之間。C1腹側支在寰椎後弓和椎動脈之間向前延伸,在寰椎側塊外側和椎動脈內側,支配頭側直肌。 The C2 nerve emerges between the posterior arch of the atlas and lamina of the axis where the spinal ganglion is located extradurally and medial to the inferior facet of C1 and the vertebral artery. Distal to the ganglion, the nerve divides into a larger dorsal and a smaller ventral ramus. After passing below and supplying the inferior oblique muscle, the dorsal ramus divides into a large medial branch, called the greater occipital nerve, and a small lateral branch. The C2 ventral ramus courses between the vertebral arches and transverse processes of the atlas and axis and behind the vertebral artery to leave this operative field (Figs. 3 and 4).
椎動脈(硬膜外部分)。成對的椎動脈起於鎖骨下動脈,經上六個頸椎橫突上行,經寰椎側塊後方,進入枕髁後方硬腦膜,經枕骨大孔上行至髓質前部,在橋髓交界處彙合形成基底動脈。
椎動脈硬膜外部分分為三段。第一節段的起點從鎖骨下動脈延伸至最低橫孔,通常在C6水平。第二節通過頸神經根前的上六個頸椎的橫孔上升。該節段在軸上方橫向偏離,到達寰椎橫孔的橫向位置。第三節是與枕骨大孔最密切相關的部分,從寰椎橫突的枕骨大孔延伸至硬腦膜的通路部位。第三節穿過寰椎側塊和寰枕關節後的內側,並壓入寰椎後弓外側部上表麵的凹槽,在那裏沿枕下三角的底部行進。它通過寰枕膜外側邊界前進入椎管。椎動脈周圍是頸深靜脈和硬膜外靜脈吻合形成的靜脈叢。C1神經根穿過椎動脈下表麵的硬腦膜並在動脈和寰椎後弓的溝之間。這種骨溝有時轉變為完全包圍一小段動脈的骨管。 The terminal extradural segment of the vertebral artery gives rise to the posterior meningeal and posterior spinal arteries, deep cervical musculature branches, and sometimes the posteroinferior cerebellar artery (Figs. 3 and 4).
硬膜外的群體。該區域的靜脈流分為兩個係統,一個由頸內靜脈引流,另一個由椎靜脈叢引流。頸內靜脈起源於頸靜脈孔,由乙狀竇和岩下竇彙合。環繞枕下三角椎動脈的靜脈叢是由許多小通道形成的,這些小通道進入椎叢內部(硬腦膜和椎骨之間),從椎弓骨後弓上方的椎管發出。後髁使者靜脈穿過後髁管,在椎靜脈叢和乙狀結腸竇之間形成溝通。舌下管靜脈叢沿舌下管延伸,將基底靜脈叢與環繞枕骨大孔的邊緣竇連接起來(圖4A)。
對CVJ前部遠外側和極外側入路(圖1,C-H,圖2,A和C-E)的描述分為兩個解剖階段。第一階段,肌肉剝離,包括皮膚切口,肌肉反射(包括形成枕下三角的肌肉),檢查肌肉與椎動脈、椎靜脈叢、寰椎橫突和上頸神經的關係。第二階段,硬膜外剝離,檢查椎動脈的轉位,寰枕關節切除的範圍,以及CVJ前部硬膜外間隙的暴露和識別。
肌肉發達的階段。手術時患者采用坐位或改良的“公園-長凳”體位(3)。采用馬蹄形頭皮皮瓣進行顯露,因為與線性切口相比,馬蹄形頭皮皮瓣能更好地顯示肌肉層及其與神經和血管結構的關係(圖5A)。切口在中線開始,大約5厘米上項線以下,並直接向上略高於上項線,橫向項線上方,到達乳突,向下,在胸鎖乳突肌後緣的頸部的肌肉在橫向方麵大約5厘米以下乳突尖和下麵的橫突阿特拉斯可以通過皮膚觸診。肌肉一般與頭皮反射成單層,露出肌肉形成枕下三角;然而,在屍體上進行了逐步的肌肉解剖,以觀察三角表麵肌肉的關係。

圖5 (a-d)。遠側寰枕經關節入路:肌肉期(A-D)和硬膜外期(E-J)。A,為了從側麵進入CVJ的前部,使用馬蹄形頭皮皮瓣進行肌肉暴露,因為它可以更容易地反射下方或下方外側的肌肉層,因此可以更廣泛地暴露外側,並為上頸椎椎板切除術提供空間。肌肉與頭皮呈單層反射,因為單獨反射肌肉會使閉合更加困難,並與傷口問題(如假性脊膜膨出)的高發相關。切口開始於枕外隆突下約5厘米的中線,向上至枕外隆突正上方,在頸上線上向外側轉彎,到達乳突,在胸鎖乳突肌後緣前向下轉彎。B,皮瓣向下和向內側反射,露出最淺表的肌肉層,由胸鎖乳突肌和頭脾肌組成,由斜方肌和頭半棘肌組成。C,向下反映頭半棘肌,露出上、下斜肌和寰椎橫突,在乳突和下頜角之間的皮膚有一個突出的頂端。枕下三角受三塊肌肉的限製(上方和內側為頭後大直肌,上方和外側為上斜肌,下方和外側為下斜肌)。D,枕下三角通過反射頭直肌後大肌在下方和內側,上斜肌在外側,下斜肌在內側打開。打開三角暴露了椎靜脈叢圍繞椎動脈的部分,它經過寰枕關節後方,穿過寰枕後弓的上邊緣。C2神經位於寰椎後弓和椎軸板之間。 Distal to the ganglion, the nerve divides into larger dorsal and smaller ventral rami. A-O, atlanto-occipital; Ant., anterior; Art., articular; Cap., capitis; CN, cranial nerve; Cond., condyle; Dent., dentate; Dors., dorsal; For., foramen; Inf., inferior; Int., internal; Jug., jugular; Lig., ligament; Long., longitudinal, longus; M., muscle; Maj., major; Min., minor; OA, occipital artery; Obl., oblique; Occip., occipital; P.I.C.A., posteroinferior cerebellar artery; Post., posterior; Proc., process; Rec., rectus; Semispin., semispinalis; Splen., splenius; Suboccip., suboccipital; Sup., superior; Trans., transverse; V., vein; VA, vertebral artery; Vent., ventral. (Images courtesy of AL Rhoton, Jr.)
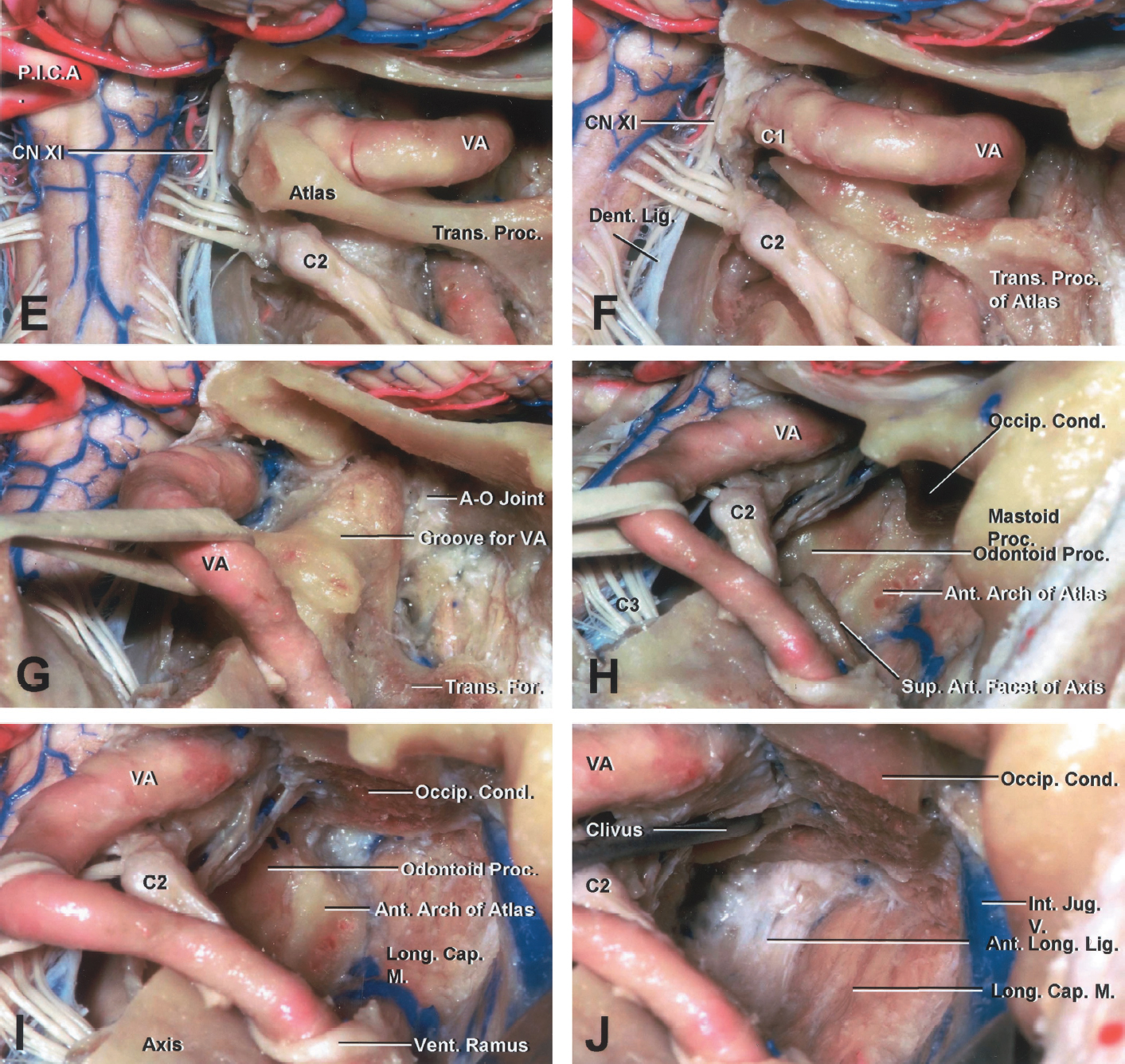
圖5 (e-j).E,暴露和控製椎動脈是手術中最重要的方麵。動脈經寰椎橫突上升後,向內側轉至寰椎側塊和寰枕關節後方,並壓入凹槽,在寰椎後弓外側部上表麵標出其路徑。F, C1神經在動脈的下表麵在動脈和寰椎後弓之間。繼續骨膜下剝離,直到在寰椎上側的椎動脈槽內發現椎動脈。使用骨膜下剝離術將椎動脈骨膜鞘的下側麵從這個凹槽中解脫出來。寰椎後弓從同側橫孔對麵的中線外取下。G,將椎動脈轉置出大西洋橫孔可以使其更側向暴露。這需要在寰椎橫孔內延長骨膜下剝離。然後通過移除後根來打開橫孔。 The vertebral artery is dissected free of the axis and displaced medially and caudally. H, the lateral mass of the atlas between the occipital condyle and the superior articular facet of the axis is totally removed. Resection of the ipsilateral transverse and alar ligaments exposes the odontoid process. I, the inferior surface of the occipital condyle can be removed if it is difficult to see the superior aspect of the dens. Care should be taken to avoid damaging the hypoglossal nerve as it passes above the occipital condyle. J, the contralateral occipital condyle is not exposed, but the contralateral edge of the dens can be seen and removed, with or without mild retraction of the ventral aspect of the dural sac. The dural sac can be retracted posteriorly to see the dens and ipsilateral half of the lower clivus. The area can be drilled using the far lateral approach, as shown in Figure 1, E and F. A-O, atlanto-occipital; Ant., anterior; Art., articular; Cap., capitis; CN, cranial nerve; Cond., condyle; Dent., dentate; Dors., dorsal; For., foramen; Inf., inferior; Int., internal; Jug., jugular; Lig., ligament; Long., longitudinal, longus; M., muscle; Maj., major; Min., minor; OA, occipital artery; Obl., oblique; Occip., occipital; P.I.C.A., posteroinferior cerebellar artery; Post., posterior; Proc., process; Rec., rectus; Semispin., semispinalis; Splen., splenius; Suboccip., suboccipital; Sup., superior; Trans., transverse; V., vein; VA, vertebral artery; Vent., ventral. (Images courtesy of AL Rhoton, Jr.)
皮瓣向下和向內側反射,露出外側胸鎖乳突肌和頭脾肌以及內側斜方肌和頭半棘肌形成的淺層肌肉的上部(圖5B)。將胸鎖乳突肌向下切開,保留枕骨的筋膜以閉合,露出頭脾的上部延伸。剝離斜方肌和頭脾肌,露出頭半棘肌,向下反射,露出上、下斜肌和寰椎橫突,寰椎橫突有一個突出的頂點,可通過乳突和下頜角之間的皮膚觸摸到。枕下三角被三塊肌肉所限製(上方和內側為頭後大直肌,上方和外側為上斜肌,下方和外側為下斜肌),通過反射下方較淺的肌肉而暴露出來(圖5C)。枕下三角通過反射頭直肌後大肌的下方和內側、上斜肌的外側和下斜肌的內側而打開。打開三角暴露了椎靜脈叢的一部分,它圍繞著椎動脈,穿過寰枕關節後方和寰椎後弓的上邊緣。C2神經位於寰椎後弓和椎軸板之間。在神經節遠端,神經分為較大的背側支和較小的腹側支(圖5D)。
硬膜外的階段。暴露和控製椎動脈是手術的一個非常重要的方麵。椎動脈位於椎軸橫孔上方,在上升至寰椎橫孔時略向外側延伸,寰椎橫孔位於椎軸橫孔的外側。動脈經寰椎橫突上升後,在寰椎側塊和寰枕關節後方向內側轉彎,壓入凹槽,在寰椎後弓外側上表麵標記其路徑(圖5E)。C1神經在動脈的下表麵在動脈和寰椎後弓之間。寰椎後弓的下緣首先暴露於骨膜下,從中線開始,一直到橫突。然後暴露向後弓的上緣發展。繼續骨膜下剝離,直到在寰椎上側的椎動脈槽內發現椎動脈。使用骨膜下剝離術將椎動脈骨膜鞘的下側麵從該凹槽中解脫出來,以減少椎靜脈叢出血。寰椎後弓從同側橫孔對麵的中線外移出(圖5F)。將椎動脈從寰橫孔轉位可以使其更側向暴露。 The subperiosteal dissection is extended along the posterior root of the transverse foramen, then the transverse foramen is unroofed by removing the posterior root. The vertebral artery is dissected free of the axis and displaced medially and caudally (Fig. 5G). The lateral mass of the atlas between the occipital condyle and the superior articular facet of the axis is totally removed. Resection of the ipsilateral transverse and alar ligaments exposes the odontoid process (Fig. 5H). The inferior surface of the occipital condyle can be removed if it is difficult to see the superior aspect of the dens (Fig. 5I). Care should be taken to avoid damaging the hypoglossal nerve as it passes above the occipital condyle. The contralateral occipital condyle is not exposed, but the contralateral edge of the dens can be seen and removed, with or without mild retraction of the ventral aspect of the dural sac. The anterior part of the cervical spinal cord is located medial to the posterior part of the lateral mass. Gentle retraction of the dural sac permits visualization of the dens and the ipsilateral half of the lower clivus (Fig. 5J).
肌肉發達的階段。患者平臥位。皮膚切口從乳突尖以下約6cm開始,沿著胸鎖乳突肌的前邊界向上延伸至外耳道,在肌肉附著上方後方彎曲(圖6A)。胸鎖乳突肌插入處被分開,留下肌筋膜袖帶附著在乳突上以閉合。乳突尖端到副神經進入胸鎖乳突肌的平均距離為3.5厘米。因此,上幾厘米的肌肉可以快速解剖,但下部分必須仔細解剖。從下外側反射胸鎖乳突肌,可暴露頸內靜脈與胸鎖乳突肌之間的平麵(圖6,B和C)。從下內側反射頭脾肌、頭半棘肌和頭最長肌,可暴露枕下三角以及依附於寰椎橫突的上、下斜肌、頭側直肌和肩胛提肌(圖6,D和E)。在曝光中可觸診寰椎橫突。分割枕下三角的插入點並反映形成枕下三角的肌肉,暴露出軸橫孔和它穿透硬腦膜的點之間的椎動脈。C2神經根暴露在寰椎和椎軸之間。 The ventral ramus of the C2 nerve root curves around the vertebral artery. The posterior belly of the digastric muscle is preserved to protect the facial nerve that exits the skull at the anterior margin of the muscle (Fig. 6F).

圖6 (a-f).極外側寰枕經關節入路:肌肉期(A-F)和硬膜外期(G-N)。A,皮膚切口開始於乳突尖以下約6厘米,沿著胸鎖乳突肌的前邊界一直到外耳道的水平,在肌肉附著上方的後方彎曲。B和C,胸鎖乳突肌的插入點被分開,留下一個肌筋膜袖帶連接到乳突以閉合。乳突尖端到副神經進入胸鎖乳突肌的平均距離為3.5厘米。因此,上幾厘米的肌肉可以快速解剖,但下部分必須仔細解剖。下外側反映胸鎖乳突肌暴露了頸內靜脈和胸鎖乳突肌之間的平麵。D和E,反映了頭脾肌、頭半棘肌和頭最長肌向內側下方暴露了枕下三角和上、下斜肌、頭側直肌和肩胛提肌與寰椎橫突的連接。在曝光中可以觸診到寰椎橫突。 F, reflecting the muscles forming the suboccipital triangle exposes the vertebral artery between the transverse foramen of the axis and the point where it penetrates the dura mater. The C2 nerve root is exposed between the atlas and the axis. The posterior belly of the digastric muscle is preserved to protect the facial nerve. A-O, atlanto-occipital; Ant., anterior; Art., articular; Aur., auricular; Br., branch; Cap., capitis; CN, cranial nerve; Cond., condyle; Cont., contralateral; Digast., digastric; Dors., dorsal; For., foramen; Gr., great; Inf., inferior; Int., internal; Jug., jugular; Lat., lateralis; Lev., levator; Long., longissimus or longus; M., muscle; Maj., major; N., nerve; OA, occipital artery; Obl., oblique; Occip., occipital; Post., posterior; Proc., process; Rec., rectus; Scap., scapula; Semispin., semispinalis; Splen., splenius; Sternocleidomas., sternocleidomastoid; Suboccip., suboccipital; Sup., superior; Trans., transverse; V., vein; VA, vertebral artery; Vent., ventral. (Images courtesy of AL Rhoton, Jr.)

圖6 (g-n).G,寰枕極外側經關節入路在乳突尖以下,頸內靜脈和硬膜囊之間。H,當胸鎖乳突肌向外側反射時,應注意保護脊副神經。最深處的肌肉是由肩胛提肌最上麵的滑塊、上、下斜肌和頭側直肌形成的,它們都附著在寰椎橫突上。I和J,這種方法的一個重要方麵是暴露和控製椎動脈。顯露寰椎後弓的橫突和外側部分後,在C1弓上表麵的凹槽中發現動脈。這個凹槽標誌著寰椎側塊的後緣。在骨膜下暴露椎動脈可減少椎靜脈叢的出血,該叢位於動脈周圍的骨膜鞘內。K,切除橫孔後根可以使動脈向下和側向遠離寰枕關節和寰椎側塊的後方。L和M,動員椎動脈後,完全鑽開寰椎側塊,必要時取出枕骨髁下表麵。 N, the odontoid process has been drilled away. The extreme lateral approach has a greater advantage than the far lateral approach in visualizing the entire odontoid process, inferior surface of the lower clivus, and medial surface of the contralateral atlantooccipital joint. The area that can be drilled using the extreme lateral approach is shown in Figure 1, G and H. A-O, atlanto-occipital; Ant., anterior; Art., articular; Aur., auricular; Br., branch; Cap., capitis; CN, cranial nerve; Cond., condyle; Cont., contralateral; Digast., digastric; Dors., dorsal; For., foramen; Gr., great; Inf., inferior; Int., internal; Jug., jugular; Lat., lateralis; Lev., levator; Long., longissimus or longus; M., muscle; Maj., major; N., nerve; OA, occipital artery; Obl., oblique; Occip., occipital; Post., posterior; Proc., process; Rec., rectus; Scap., scapula; Semispin., semispinalis; Splen., splenius; Sternocleidomas., sternocleidomastoid; Suboccip., suboccipital; Sup., superior; Trans., transverse; V., vein; VA, vertebral artery; Vent., ventral. (Images courtesy of AL Rhoton, Jr.)
硬膜外的階段.該方法的一個重要方麵是暴露和控製椎動脈。顯露寰椎橫突和後弓外側後,在C1弓上表麵的凹槽內發現動脈。這個凹槽標誌著寰椎側塊的後邊緣(圖6,G-J)。使用骨膜下剝離術將內襯凹槽的骨膜鞘抬高,使用鑽頭或小咬骨鉗去除橫突。在骨膜下暴露椎動脈可減少位於動脈周圍的骨膜鞘內的椎靜脈叢的出血。切除橫孔後根可使動脈向下和側向移位,遠離寰枕關節和寰椎側塊(圖6K)。寰椎側塊向上至枕骨髁,向下至軸的上關節麵,從而暴露軸的齒狀突。枕骨髁沿枕骨大孔前半部分的側邊向下突出。軸的上關節麵位於齒狀突基部的外側(圖6L)。 Drilling can be extended to the lower surface of the occipital condyle to expose the superior aspect of the dens (Fig. 6M). Removing the odontoid process exposes the medial aspect of the contralateral atlanto-occipital joint and the inferior surface of the lower clivus (Fig. 6N). Care is taken to avoid damage to the internal jugular vein, which is located immediately anterior to the transverse process of the atlas.
涉及CVJ前部硬膜外間隙的腫瘤、血管性、創傷性、先天性和退行性病變並不罕見。關於該區域病變的適當治療方法存在一些爭議。前路,包括經口入路及其變異,主要用於位於CVJ前部的硬膜外病變(5,12,14,15,17)。後路、後外側和外側入路常用於進入位於CVJ前方或前外側的硬膜內病變(4,11,13,22 - 24)。然而,關於CVJ前部硬膜外間隙的詳細顯微外科解剖研究很少(1,2,25)。
各種各樣的後外側手術入路用於前外側或前外側CVJ已經被描述(3,4,9,11,13,16,18,21 - 24,27)。這些入路分為兩大類:遠外側入路和經髁入路。不鑽枕髁,基本的遠外側入路,也被描述為後外側入路,可能是到達枕骨大孔前外側邊緣的一些病變所需要的全部。然而,它也提供了一條經髁、髁上和髁旁入路以及遠外側入路的幾種修改可以完成的路徑(19,27)。寰枕經關節入路可分為兩種類型:遠外側(後外側)和極外側,這取決於前硬膜外暴露在CVJ的程度。這兩種經關節路徑相似,但從幾個角度來看完全不同,包括入路方向、肌肉、神經和血管解剖以及暴露的解剖結構。
遠外側入路定義為從胸鎖乳突肌後外側入路,由Heros首次報道(13)。肌肉剝離是手術中最重要的部分之一。以前曾報道過遠外側入路肌肉剝離的詳細描述(19,27)。為了從側麵進入CVJ的前部,使用馬蹄形頭皮皮瓣進行肌肉暴露,因為它更容易反射下方或下方外側的肌肉層,從而允許更廣泛的外側暴露和上頸部入路的空間。肌肉與頭皮反射在一個單層上,因為單獨反射肌肉會使閉合更加困難,並且與傷口問題的高發有關,如假性脊膜膨出。可見形成枕下三角的肌肉,可見椎動脈周圍有豐富的靜脈叢。寰枕遠外側經關節入路需要打開橫突,並將椎動脈第三段轉位至下內側。George和Laurian(7)和George等人(9)首次描述了椎動脈從軸到硬腦膜入口的內側移位。這種技術降低了寰枕關節內側鑽孔時椎動脈損傷的風險。椎動脈骨膜下暴露是避免椎靜脈叢出血的關鍵。 Drilling away or removing the entire lateral mass of the atlas increases access to the anterior aspect of the CVJ in front of the spinal cord, because the posterior margin of the lateral mass is usually located at the level of the anterior part of the spinal cord. Removing the entire lateral mass, including the anterior portion, provides greater access and is safer for retraction of the dural sac than removal of only the posterior portion of the lateral mass. Removing the inferior surface of the occipital condyle exposes the superior part of the odontoid process. It is not necessary to open the hypoglossal canal unless the lesion is situated above the lower clivus. This approach has several advantages over the anterior transoral approach, including shorter distance to the lesion, control of the vertebral artery, easy access to laterally located lesions, and the wide and sterile operative view; in addition, posterior stabilization is possible if needed. The far lateral atlanto-occipital transarticular approach, compared with the extreme lateral approach, provides an easy orientation familiar to neurosurgeons and eliminates manipulation near great vessels and the spinal accessory nerve. However, the far lateral atlanto-occipital transarticular approach has a disadvantage in not allowing visualization of the contralateral anterior extradural operative field. Some retraction of the dural sac is necessary in identifying the contralateral structures. Extradural lesions located in the ipsilateral anterolateral aspect of the CVJ can be managed with the far lateral atlanto-occipital transarticular approach.
Sen和Sekhar(23,24)首先描述了極外側寰枕經關節入路,從外側穿過關節柱和乳突尖。該入路也稱為前外側入路(11)或經髁入路(1)。鑽孔的範圍與遠外側寰枕經關節入路相同。極外側寰枕經關節入路與遠外側寰枕經關節入路的區別在於皮膚切口、肌肉反射和入路方向不同。在極外側入路中,胸鎖乳突肌沿其前緣切開,並在與枕骨和顳骨的附著點完全分開。在頸內靜脈和硬膜囊之間,肌肉和脊副神經的下外側反射為頸內靜脈和硬膜囊之間的CVJ前部提供了直接的外側通路。這種暴露的基本原理與Verbiest(26)描述的相似,Verbiest使用該技術去除壓迫下頸椎椎動脈和神經根的骨贅;但是,這種方法沒有訪問中線。正如George等人所描述的,該技術也類似於斜向椎體切除術(10)。寰枕極外側經關節入路主要應用於硬膜外病變(1,2,8,25),但也用於硬膜內病變(23,24)。對於CVJ硬膜外非腫瘤性病變,AlMefty等人(1)報道使用經髁入路鑽孔乳突尖、枕骨髁至舌下管下表麵和寰椎髁表麵。 Care is required to preserve the spinal accessory nerve when the sternocleidomastoid muscle is reflected inferolaterally. In the extreme lateral atlanto-occipital transarticular approach, the muscles attached to the transverse process of the atlas are detached from their insertion on the transverse process. Care is taken not to damage the vertebral artery, the internal jugular vein, and the ventral rami of the spinal nerves, all of which exist beneath these muscles. This approach also requires transposition of the vertebral artery, as does the far lateral atlanto-occipital transarticular approach, using subperiosteal dissection along the upper margin of the axis. After mobilizing of the vertebral artery, the complete lateral mass of the atlas is drilled away, followed by the removal of the inferior surface of the occipital condyle if necessary. The extreme lateral atlanto-occipital transarticular approach, in addition to having the advantages of the far lateral approach, provides exposure of the entire odontoid process, the inferior aspect of the lower clivus, and the medial surface of the contralateral atlanto-occipital joint. Moreover, this approach eliminates the need to retract the dural sac to expose the odontoid and clivus anterior to the cervicomedullary junction. Complete drilling of the lateral atlantal mass by either the far lateral or extreme lateral approaches must be followed by occipitalcervical stabilization and fusion. This stabilization, however, can be performed in the same operative field in both approaches, whereas the anterior transoral approach requires another procedure if posterior occipital-cervical fusion is needed.
總之,對於位於CVJ硬膜外區域同側前方或前外側的病變,應選擇寰枕遠外側經關節入路。當病變延伸至對側寰枕關節和下斜坡時,應選擇極外側寰枕關節經關節入路。這些入路對於累及毗鄰枕突和寰突髁並延伸至前硬膜外間隙的結構的病變是理想的,但對於嚴格局限於齒狀突和寰椎前弓正中的病變不一定是理想的,這可能最好通過經口入路。
遠外側和極外側寰枕經關節入路為暴露CVJ硬膜外病變提供了經口入路的另一種選擇。兩種方法都避免了汙染鼻咽,並提供了一個更短的手術路線。
參與者:Masatou Kawashima, MD, Necmettin Tanriover, MD, Albert L. Rhoton, Jr, MD, Arthur J. Ulm, MD, Toshio Matsushima, MD
來自Kawashima M, Tanriover N, Rhoton AL, Jr, Ulm AJ, Matsushima M.寰枕經關節入路治療顱頸交界前硬膜外病變的遠側側型和極外側型的比較。神經外科2003; 53:662 - 675。doi.org/10.1227/01.NEU.0000080070.16099.BB.經牛津大學出版社許可,代表神經外科醫生協會。©神經外科醫生協會。
神經外科188bet手机app圖集很榮幸能夠保持Albert L. Rhoton, Jr, MD的遺產。
請登錄發表評論。
請務必在社交媒體上關注我們,獲取令人興奮的內容,並保持更新生活科恩醫生的會議,關於手術技術的問題,以及更多!



您必須登錄才能查看此資料。
的188bet手机app幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈我們無法繼續製作《地圖集》。
請承諾每年至少向Atlas捐贈250美元。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法使用它,他們的病人的護理依賴於它。
請立即捐款!
如果沒有你們的大量捐贈我們無法繼續製作《地圖集》。請承諾每年至少向Atlas捐贈250美元。
如果沒有這個承諾,Atlas將很快需要付費訂閱世界各地的許多外科醫生都無法使用它,他們的病人的護理都依賴於它。請立即捐款!