

你可以有所作為。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
請立即捐款!
最後更新:2021年4月9日
背景頸靜脈神經鞘瘤的手術入路多種多樣,選擇入路困難。本研究的目的是定義這些方法的解剖元素。
方法:對10具成年屍體頭部進行了檢查。
結果頸靜脈孔的不同部位有外側、後、前三個通路。除去枕骨頸突提供了進入頸靜脈球後側的通道,霰雨下乳突切除術提供了進入頸靜脈球外側邊緣和穹窿的通道,耳前入路提供了進入頸靜脈球和頸靜脈孔前緣的通道。這些入路的補充包括頸椎和椎動脈暴露,麵神經移位,枕骨大孔暴露,外管和髁突切除。
結論了解頸靜脈孔的解剖結構對於實現完全切除腫瘤同時最小化風險至關重要。

25%的神經鞘瘤發生在頭部和頸部。1顱內神經鞘瘤可起源於顱神經(CNs),然而,除了前庭神經鞘瘤外,它們並不常見。2 - 4頸靜脈孔神經鞘瘤主要起源於中樞神經IX和x的神經節5提出這些腫瘤在頸靜脈孔的生長方式取決於起源的神經節。然而,不同的位置和神經和血管累及使得一些腫瘤的確切起源位置難以確定。5 - 9影像學的進步有助於區分頸靜脈孔神經鞘瘤與頸靜脈球瘤、腦膜瘤和其他腫瘤,並確定腫瘤的精確位置、範圍和血管關係。9選擇合適的入路應基於術前神經學檢查結果,以及MRI、CT和血管造影顯示的腫瘤大小、位置和擴展。頸靜脈孔神經鞘瘤的幾種分類是基於腫瘤的位置、大小和擴展。3、7、10、11Kaye等人的分類7很受歡迎,而Pellet et al10增加了沙漏型腫瘤。A型腫瘤主要位於顱內,部分延伸至孔內;B型腫瘤主要位於孔內,伴或不伴顱內延伸;C型腫瘤主要為顱外腫瘤,輕度延伸至孔內或後窩內;D型腫瘤呈啞鈴狀,顱內和顱外延伸通過孔相連。將腫瘤歸為其中一類有助於手術計劃和選擇合適的手術入路。
頸靜脈孔通常由後路和外側路進入,較少由前路進入。眾多的入路導致了選擇合適入路的困惑。在本研究中,將入路文獻與確定每種入路主要解剖特征的解剖切片相結合(表1)。3、6、7,12-33

從福爾馬林灌注的成年屍體頭部中,動脈和靜脈被注入紅色或藍色矽橡膠(道康寧,米德蘭,MI),稀釋劑200(道康寧)和RTV催化劑(道康寧),使用33至340倍的外科顯微鏡和一個與氙氣光源和高清相機連接的08,18厘米霍普金斯內內鏡(Karl Storz GmbH, KG, Tottlingen, Germany)進行解剖。外側枕下,遠外側,20日,32歲的34postauricular transtemporal,14日,35耳前顳下顳下窩,28內窺鏡經鼻/上頜經眶後入路16日,36歲,37歲從不同角度打開頸靜脈孔。
顳骨的岩狀部分形成了頸靜脈球孔和穹窿的前上部分。枕骨頸突形成了椎間孔的後緣。頸靜脈孔位於枕乳突縫線外側和枕岩裂內側之間(見圖1)。頸靜脈球頂位於前庭迷路下方。

圖1。(A)右側頸靜脈孔後上視圖。椎間孔分為岩狀、乙狀結腸和頸內3個部分。乙狀結腸竇通過乙狀結腸部分而岩下竇通過岩部。(B和C)頸靜脈孔和頸靜脈突的下視圖。枕髁位於髁突窩的前方(斷續線)。頸靜脈突(綠色)位於頸靜脈孔的後部,從枕髁的後半部分向外側延伸。頸靜脈窩和頸靜脈孔位於枕髁前半部分的上方和外側。(D)後視圖,右側橋小腦角。 The jugular foramen is located between the internal acoustic meatus and the jugular tubercle. The rectus capitis lateralis attaches to the inferior surface of the jugular process, which is located posterior to the jugular foramen. (E) Endoscopic view of the right jugular foramen. CNs IX, X, and XI pass through the intrajugular part of the foramen. The dural roof of the foramen is the site of the glossopharyngeal and vagal meati. A dural septum separates the 2 meati. (F) Lateral view of the intrajugular part of the left jugular foramen. The jugular bulb has been translocated posteriorly after removing all of the temporal bone except the petrous apex. The inferior petrosal sinus passes between the glossopharyngeal and vagus nerves to empty into the jugular bulb. The accessory nerve passes posterior to the vagus nerve. A., artery; Ac., acoustic; Atlanto-occip., atlantooccipital; Cap., capitis; Car., carotid; Cond., condylar, condyle; Fiss., fissure; Flocc., flocculus; For., foramen; Glossopharyng., glossopharyngeal; Hypogloss., hypoglossal; Inf., inferior; Int., internal; Intrajug., intrajugular; Jug., jugular; Lat., lateralis; Lt., left; M., muscle; Mag., magnum; Mast., mastoid; Meat., meatus; N., nerve; Occip., occipital; Occipitomast., occipitomastoid; Pet., petrosal; Petro-occip., petro-occipital; P.I.C.A., posterior inferior cerebellar artery; Proc., process; Pyramid., pyramidal; Rec., rectus; Rt., right; Sig., sigmoid; Styl., styloid; Stylomast., stylomastoid; Sup., superior; Temp., temporal; Tuberc., tubercle; Vag., vaginal; Vert., vertebral. (Images courtesy of AL Rhoton, Jr.)
頸靜脈孔分為3部分:岩部(岩竇通過),乙狀竇(乙狀竇通過)和頸內(神經通過)。頸內部分位於乙狀結腸和岩狀部分之間,是位於顳骨和枕骨相對表麵的稱為頸內突的骨突起的位置(圖1A)。頸內脊沿著頸靜脈球的內側邊緣從顳骨的頸內突向前延伸與頸內脊在進入頸動脈管的後邊緣彙合稱為頸動脈脊。顳骨頸內脊略向內側,在其內側表麵有一個淺的舌咽溝,舌咽神經沿此溝而行。頸動脈脊將頸靜脈孔和頸動脈管分開,並與莖突在其側緣附近相遇(圖1B和1C)。覆蓋頸靜脈孔的硬腦膜被硬腦膜折分為舌咽肌和迷走肌。
枕髁位於頸靜脈孔下方和內側的枕骨大孔前半部分的外側緣(圖1B和1C)。枕髁位於髁突窩淺凹陷的前方和下方,在這裏,後髁導靜脈進入後髁突管,到達並流入乙狀竇。枕骨頸突從枕骨髁的後半部分向外側延伸形成了孔的後緣。當結合枕下外側入路、冰雨下乳突切除術或頸椎暴露術時,切除頸突提供了進入頸靜脈球後緣和頸內靜脈的途徑。枕乳突縫合穿過頸靜脈突的外側邊緣和二腹肌溝和莖突的內側邊緣,止於頸靜脈孔(圖1B和1C)。莖突孔,麵神經通過它,位於頸靜脈突的前外側。
頸靜脈球和頸內靜脈鄰近部分同時接受顱內靜脈和顱外靜脈的引流,包括乙狀竇和岩下竇、椎靜脈叢、舌下管靜脈叢、後髁密使靜脈和沿岩枕裂下側的靜脈。岩下竇上端與海綿竇和基底靜脈叢相通,下端與頸靜脈球或頸內靜脈相通(圖1F)。38
此前沒有單一的手術入路報道可進入頸靜脈孔的全部邊緣,然而,根據入路選擇,從報道的入路中選擇可進入頸靜脈孔所有邊緣的選擇性段。為了評估這一點,在單個標本上進行了暴露孔前、外側和後表麵的入路。它從耳後經顳孔入路開始,通過高暴露的頸部來控製頸內動脈、頸內靜脈和頸內孔以下的下中樞神經。第一步是分離附著在乳突上的肌肉,包括胸鎖乳突肌、半棘肌、最長肌和二腹肌,暴露枕動脈、頭外側直肌、C1橫突和枕下三角。在第一步之後,C1橫突、乳突尖、覆蓋麵神經的腮腺和頭外側直肌仍然是暴露孔的障礙(圖2A)。接下來,進行雪花雨下乳突切除術,以暴露頸靜脈球的上側麵(圖2B)。移除乳突尖沿枕乳突縫線向下延伸鑽孔暴露乙狀竇到達頸靜脈突下表麵的頭外側直肌附著處。乙狀竇在進入頸靜脈球之前穿過枕乳突肌線。如果麵神經不向前轉位,頸靜脈突不切除,這個手術野會受到限製(圖2C)。分離頭外側直肌並切除枕骨頸靜脈突,打開了頸靜脈孔的後下側,為不移位麵神經的腫瘤切除提供了廣闊的通路(圖2D)。 Extending the drilling medially above the jugular bulb exposes the cochlear aqueduct, which opens into the pyramidal fossa located medial to the glossopharyngeal groove of the temporal bone (Figures 1C and 2E). Next, several steps were added to widen the surgical field. The fallopian bridge technique in which the facial canal is skeletonized without transposition is completed to expose the junction of the inferior petrosal sinus, the jugular bulb, the area anterolateral to the jugular bulb, and the middle ear cavity (Figure 2E).27,39 An intracranial extension of the tumor can be accessed by opening the presigmoid or retrosigmoid dura. In the presigmoid approach, the otic capsule will rarely be an obstacle if the sigmoid sinus and the posterior fossa dura behind the cochlear canaliculus are exposed to provide access to the area between the jugular foramen and the nerves entering the internal acoustic meatus (Figure 2F). For the retrosigmoid approach, the superior oblique muscle is detached from the superior nuchal line and a lateral suboccipital craniectomy is completed to access the lower CNs intradurally (Figure 2G).

圖2。(A)宮頸暴露程度高。插入片(左上)顯示左耳後c形切口。高頸夾層暴露了乳突尖、頭側直肌和上、下斜肌和頭直肌後大肌之間的枕下三角(虛線)。(B)雪花雨下乳突切除術。每個半規管都已暴露;上(S)、外側(L)和後(P)。雪花雨下和麵後空氣細胞已被切除,以暴露頸靜脈球。行後鼓室切開術,以方便暴露顏麵管。(C)切除乳突尖暴露頭外側直肌與頸靜脈突下表麵的附著。為了避免損傷麵神經,保留了包裹神經的纖維組織袖套和莖突孔處的莖突動脈。 (D) Removing the jugular process and rectus capitis lateralis exposes the posterior surface of the jugular bulb. The posterior condylar emissary vein connects the jugular bulb and the vertebral venous plexus. (E) Fallopian bridge technique, which leaves a thin shell of bone around the facial nerve. The drilling has been extended below the facial recess, and the bone between the facial canal (fallopian canal) and the posterior wall of the external auditory canal have been removed to provide a view into the middle ear and the anterolateral aspect of the jugular foramen. (F) Presigmoid exposure. The cochlear aqueduct has been exposed before opening the presigmoid dura. The dura in front of the sigmoid sinus has been opened to expose cranial nerves (CNs) VII to XI. (G) Retrosigmoid exposure. The dura behind the sigmoid sinus has been opened to expose CNs VII to XI. A., artery; A.I.C.A, anterior inferior cerebellar artery; Acc., accessory; Ant., anterior; Aque., aqueduct; Aud., auditory; Auric., auricular; Br., branch; Cap., capitis; Car., carotid; Chor., chorda, choroid; Cochl., cochlear; Cond., condylar; Dig., digastric; Emiss., emissary; Endolymph., endolymphatic; Ext., external; Flocc., flocculus; For., foramen; Gl., gland; Gr., greater; Inf., inferior; Int., internal; Jug., jugular; Lat., lateral, lateralis; Lev., lavator; M., muscle; Mast., mastoid; Meat., meatus; N., nerve; Obl., oblique; Occip., occipital; Occipitomast., occipitomastoid; Pet., petrosal; Plex., plexus; Post., posterior; Rec., rectus; Scap., scapulae; Sig., sigmoid; Stylomast., stylomastoid; Suboccip., suboccipital; Sup., superior; Surf., surface; Temp., temporal; Tymp., tympani, tympanic; V., vein. (Images courtesy of AL Rhoton, Jr.)
32分離附著於上、下頸線上的肌肉,暴露出髁窩、椎動脈和周圍的靜脈叢,後者與後髁導靜脈相連,穿過位於枕髁上方的髁管(圖3A和3B)。從後視圖看,頭外側直肌的插入處位於枕動脈和二腹肌內側。在靜脈外打開頸靜脈孔後緣需要切除頸靜脈突,頸靜脈突在頸靜脈孔後橫向延伸(圖3C和3E)。如Wen等人所述,將頭側直肌從頸靜脈下表麵剝離後,取出頸靜脈突,露出頸靜脈孔的後下表麵32(圖3 e)。鑽枕骨髁和枕骨髁上方區域以暴露舌下管及其與頸內靜脈內側表麵的連接處,很少需要,可能會導致頸顱不穩定,需要進行枕頸融合(圖3E)。副神經偶爾穿過C1橫突和頸內靜脈之間。40
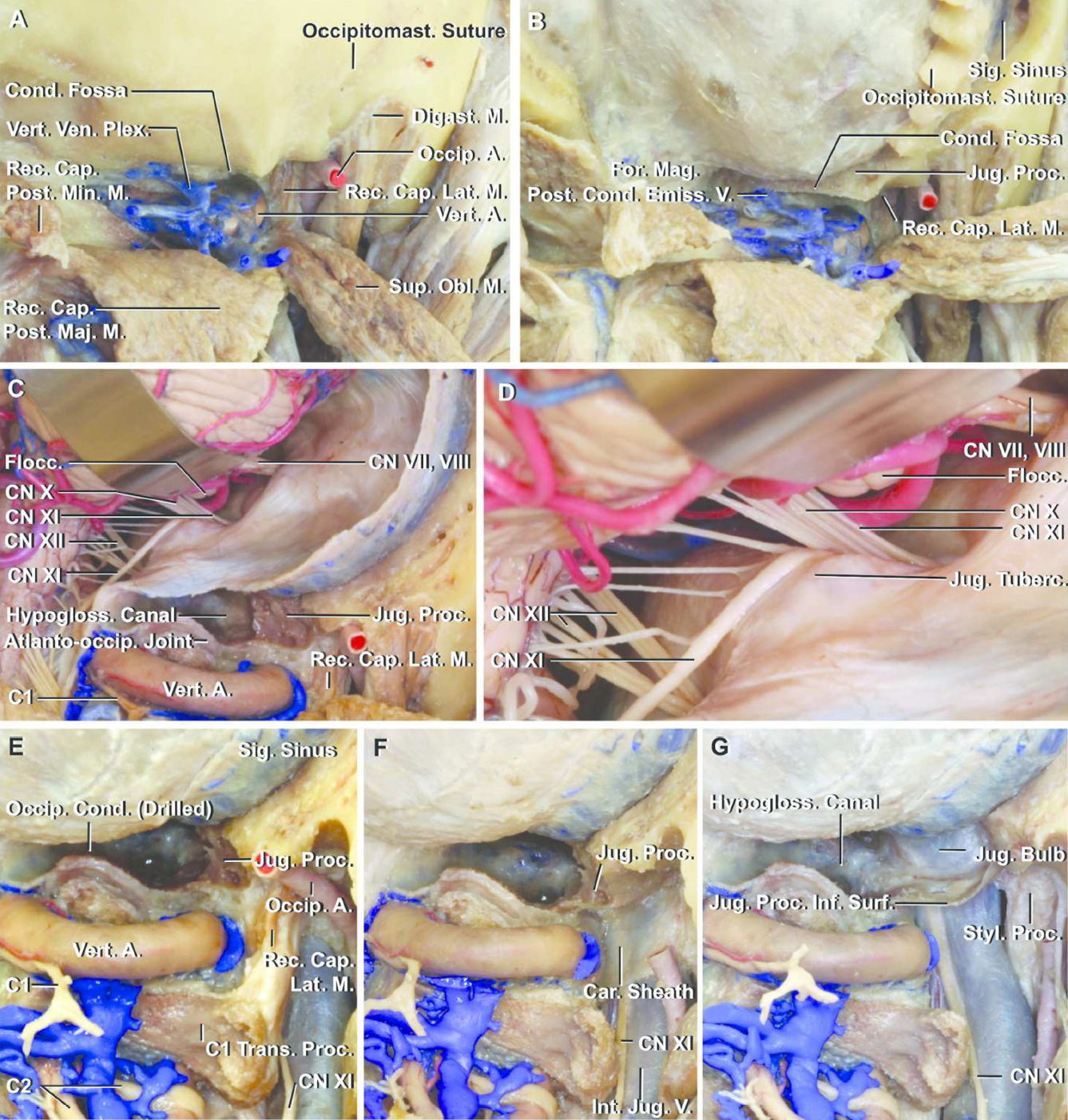
圖3。(A)右側枕下暴露,頭部為坐位。從上、下頸線上分離肌肉,暴露了枕下區域、椎動脈、椎靜脈叢周圍區域和頭側直肌。(B)在保留顱骨縫合線的情況下進行開顱手術。髁突使者靜脈與椎靜脈叢和乙狀竇相連,在髁突窩進入後髁管。頭側直肌附著於頸靜脈突的下表麵。(C)乙狀竇後暴露提供顱神經(CNs) VII至XII的視圖。枕骨髁上方的鬆質骨已鑽出舌下管,它通過枕骨髁上方。頸靜脈突被保存了下來。(D) 3C的放大視圖。 (E–G) Drilling of the occipital condyle to show that removing the condyle does not expose the posterior surface of the jugular bulb (E and F). Detaching the rectus capitis lateralis from the inferior surface of the jugular process exposes the carotid sheath, which encloses the internal jugular vein, carotid artery, and the accessory nerve. (G) Removing the jugular process exposes the posterior surface of the jugular bulb. The hypoglossal canal passes anterolaterally above the condyle. The venous plexus in the hypoglossal canal empties into the junction of the jugular bulb and the internal jugular vein. A., artery; Atlanto-occip., atlanto-occipital; Cap., capitis; Car., carotid; Cond., condylar, condyle; Dig., digastric; Emiss., emissary; Flocc., flocculus; For., foramen; Hypogloss., hypoglossal; Inf., inferior; Int., internal; Jug., jugular; Lat., lateralis; M., muscle; Mag., magnum; Maj., major; Min., minor; Obl., oblique; Occip., occipital; Occipitomast., occipitomastoid; Plex., plexus; Post., posterior; Proc., process; Rec., rectus; Sig., sigmoid; Styl., styloid; Sup., superior; Surf., surface; Trans., transverse; Tuberc., tubercle; V., vein; Ven., venous; Vert., vertebral. (Images courtesy of AL Rhoton, Jr.)
Fisch and Pillsbury12Fisch等人41A型顳下窩入路或Sekhar等28森和塞甲42采用耳前顳下顳下窩入路和兩種外側入路進入頸靜脈孔的前外側。耳前顳下顳下窩入路,如Sekhar等人所述,28提供通往顳下窩和頸靜脈球前外側的通道,並使頸動脈岩向前移位和到達岩尖成為可能(圖4A和4B)。切除卵圓孔周圍的中窩底、頸岩、岩下竇和顳骨陰道突下半部內側,露出頸靜脈球前緣、頸動脈脊和舌咽神經出口部位(圖4B)。除去莖突後,頸靜脈球開口的前外側邊緣暴露出來,但必須注意避免損傷該部位的麵神經。

圖4。(A)插入片(左上)顯示耳廓前顳下顳下窩暴露的切口。腮腺在保留麵神經的同時向前移動。切除中窩底、下頜髁和翼突外側肌,暴露顳下窩和下頜後間隙。將頸內動脈向前移位,鑽孔顳骨鼓膜部陰道突的一部分,暴露頸靜脈孔,舌咽神經和頸動脈脊的前方。(B)曝光放大圖。在顳骨陰道突內側鑽孔,露出頸靜脈孔的前部和頸內靜脈與頸靜脈孔的交界處。舌咽神經在頸動脈脊的後麵延伸到頸部。(C)經鼻/上頜經眶後入路至頸靜脈孔。插入片(左上)顯示右側上頜竇和鼻腔。 The posterior wall of the right maxillary sinus has been removed, the sphenoid sinus is opened, and the lateral pterygoid muscle resected to expose the maxillary artery and the infratemporal and pterygopalatine fossae. (D) Retracting the medial pterygoid muscle and separating the tensor veli palatini from the eustachian tube and resecting it opens a corridor to the jugular foramen. Opening the stylopharyngeal aponeurosis exposes the internal carotid artery entering the carotid canal, and the internal jugular vein and glossopharyngeal nerve. A., artery; Apon., aponeurosis; Auric., auricular; Car., carotid; Cav., cavernous; Chor., chorda; CN, cranial nerve; Eust., eustachian; Fibrocart., fibrocartilage; Gang., ganglion; Gen., geniculate; Gl., gland; Gr., greater; Inf., inferior; Int., internal; Jug., jugular; Lev., levator; M., muscle; Max., maxillary; Mandib., mandibular; Med., medial; Men., meningeal; Mid., middle; N., nerve; Orb., orbital; Pal., palatine; Palat., palatini; Pet., petrosal; Proc., process; Pteryg., pterygoid; Sternocleidomast., sternocleidomastoid; Sphenopal., sphenopalatine; Stylopharyng., stylopharyngeal; Sup., superior; Temp., temporal; Tens., tensor; Tymp., tympani; V., vein; Vag., vaginal. (Images courtesy of AL Rhoton, Jr.)
最近,頸靜脈孔已被內窺鏡暴露。16日,36歲,37歲,43歲在該技術中,夾層通過經鼻/上頜和經甲狀腺後向咽鼓管延伸(圖4C)。咽鼓管是到達頸靜脈孔的重要標誌。橫切翼外肌後,翼內肌和齶板張肌向外側反射,露出咽鼓管、提齶板肌的管狀附著和莖咽筋膜(腱膜),後者覆蓋頸內動脈、頸內靜脈和下中樞神經係統,打開後露出頸靜脈孔下方的區域。頸內動脈在頸內靜脈的前內側上升。CN IX出頸靜脈孔後,在頸內靜脈和頸內動脈之間向外側下降(圖4D)。陰道突包圍莖突基部,覆蓋頸內靜脈和頸靜脈球的前外側和外側(圖4D)。
最後,在完成遠外側入路、雨淋下乳突切除術、保留下表麵的頸靜脈突切除術和耳前顳下顳下窩入路後,對標本進行檢查,以確定每種入路對頸靜脈孔的暴露增加程度(見圖5)。莖突根和莖突根是完全打開頸靜脈孔的障礙,切除頸靜脈突為移除頸靜脈孔內的腫瘤提供了廣闊的通道(圖5B-5D)。在耳前顳下顳下窩入路中,鑽入陰道突內側暴露頸靜脈球的前外側部分(圖5E和5F),切除莖突擴大了這種暴露。枕下外側入路聯合頸靜脈突切除提供了在顱外和顱內進入頸靜脈孔的途徑,並擴大了頸靜脈球後下麵的暴露。切除枕髁提供了進入舌下管的通道,但沒有增加頸靜脈孔的暴露(圖5G和5H)。
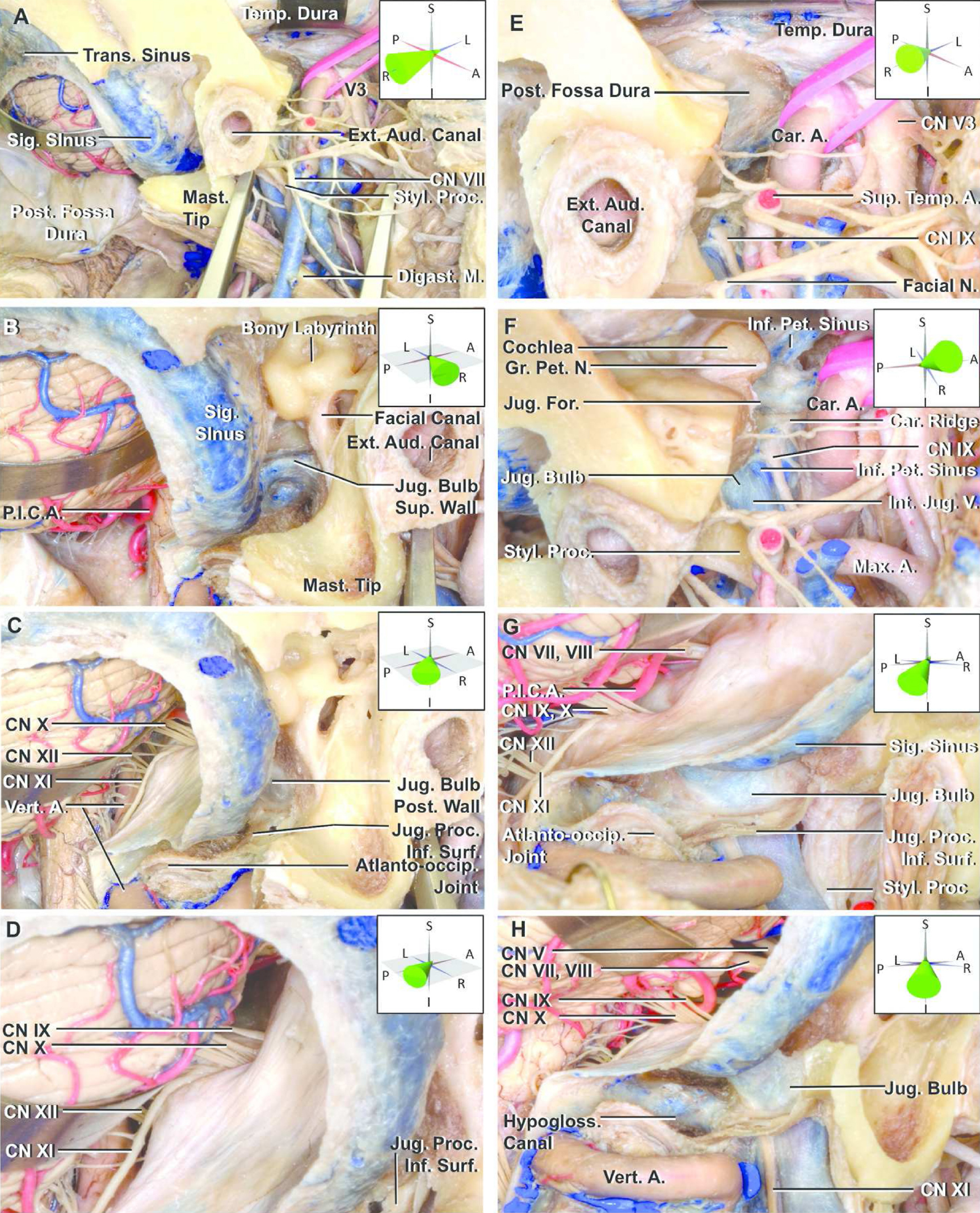
圖5。多路暴露頸靜脈孔。(A-H)右側已完成遠外側、耳前經顳下、經乳突雨淋下的暴露,以顯示不切除外耳道和麵神經易位即可實現頸靜脈球的暴露程度。腮腺被切除了以便更容易看到麵神經和頸靜脈孔周圍的區域。每個圖的角度顯示在插入使用3D坐標軸。(A)橫向視圖。乳突尖、莖突和外耳道是暴露頸靜脈孔的障礙。(B)與外耳道平行的後外側暴露。從這個角度可以看出頸靜脈球的上表麵和外側表麵。從這個角度看,乳突尖端不妨礙進入頸靜脈球外側。 However, the facial canal blocks access to the jugular bulb. (C) A 45° posterolateral view. The jugular process has been removed while preserving its inferior surface. Removing the jugular process exposes the posterior wall of the jugular bulb. (D) Rotating the view posteriorly provides a view of cranial nerves (CNs) IX, X, and XI entering the dural roof of the jugular foramen. (E) Lateral view of the preauricular subtemporal infratemporal fossa approach. The floor of the middle fossa has been removed and the medial half of the vaginal process of the tympanic part of the temporal bone drilled to expose the sigmoid sinus at the anterior edge of the jugular foramen. The parotid gland has been removed to facilitate the view of the anterior edge of the jugular foramen. (F) Superolateral view. The floor of the middle fossa lateral to the cochlea has been removed. The inferior petrosal sinus empties into the internal jugular vein just below the jugular bulb. The glossopharyngeal nerve descends through the dural glossopharyngeal meatus and turns downward lateral to the inferior petrosal sinus. (G) Lateral suboccipital (retrosigmoid) approach. This approach accesses the dural roof of the jugular foramen. Removing the jugular process of the temporal bone exposes the posterior and inferior surfaces of the jugular bulb. In this view, the vertebral artery partially blocks the view of the course of the accessory nerve. (H) View lateral to that shown in panel G. The intracranial, posterior/inferior surfaces of the jugular foramen, and hypoglossal canal have been exposed. The course of the accessory nerve is visible without translocation of the vertebral artery. A., artery; Atlanto-occip., atlanto-occipital; Aud., auditory; Car., carotid; Dig., digastric; Ext., external; Gr., greater; Hypogloss., hypoglossal; Inf., inferior; Int., internal; Jug., jugular; M., muscle; Mast., mastoid; Max., maxillary; N., nerve; Pet., petrosal; P.I.C.A., posterior inferior cerebellar artery; Post., posterior; Proc., process; Sig., sigmoid; Styl., styloid; Sup., superior; Surf., surface; Temp., temporal; Trans., transverse; V., vein; Vert., vertebral. (Images courtesy of AL Rhoton, Jr.)
大多數頸靜脈孔神經鞘瘤經側路或後路入路。有些外側入路和後路入路相似,但名稱不同,有些是以前入路的組合,並賦予了新的名稱(表1)。這增加了選擇手術入路的難度。本研究的目的是確定頸靜脈孔入路的解剖步驟。在頸靜脈孔入路的手術步驟中,頸靜脈突切除是其中最重要的步驟之一。Wen等人,32Nakamizo等人,25Nakamizo等人,31和Sanna等人44描述了切除頸靜脈突對暴露頸靜脈球後下表麵的重要性(圖6A)。如果椎間孔內的腫瘤向後延伸或閉塞球,可以考慮加行頸靜脈突切除。3、6、8、14、17、19、21、23日,29日,30日,45在鑽頸突時應注意避免損傷麵神經,因為莖突孔位於頸突的外側。另一個重要步驟是雨淋下乳突切除術,通常包括在外側入路或聯合入路,但也可以包括在後入路(表1)。

圖6。(A)頸靜脈孔下視圖。右側頸靜脈孔下表麵的圖像顯示頸靜脈球(深藍色)、頸內動脈(紅色)和乙狀竇(淺藍色)的位置。頸靜脈突切除後暴露出的椎間孔邊緣(綠色)。經耳前顳下入路暴露的區域沿著孔的前外側邊緣(黑色實線),切除鼓室的陰道突(黑色間斷線)可使頸動脈向前轉位並鑽開孔的前緣。(B)的前視圖後麵對一個日冕部分通過頭骨後正確的外耳道的白線所示插入麵板的上部角落B infralabyrinthine乳突切開術打開了一個廣闊的區域內從頂部的圓頂的外側頸靜脈球(固體紫色的線麵板B)。宮頸接觸提供下麵的頸內靜脈孔(打斷了紫色的線麵板B)。外側枕下入路(乙狀竇後暴露)可在顱內進入頸靜脈孔(圖B中橙色圓圈區域)。交流,聲;CN,顱神經;的車。, carotid; Cond., condyle; Int., internal; JF, jugular foramen; Jug., jugular; Mand., mandibular; Mast., mastoid; Meat., meatus; N., nerve; Occip., occipital; Pet., petrosal; Proc., process; Sig., sigmoid; Stylomast., stylomastoid; V., vein. (Images courtesy of AL Rhoton, Jr.)
A型顳下窩入路12日,41耳前顳下顳下窩入路,28日,42這兩條外側通路,都通向頸靜脈孔的前外側和前邊緣。頸靜脈孔是由前上方顳骨的岩石部分和後下方枕骨的頸靜脈突組成的。陰道突包圍莖突基部阻斷了通往頸內靜脈和頸靜脈球連接處的前外側和外側的通路。暴露頸靜脈孔的前外側很有挑戰性因為頸靜脈孔的下開口位於頸動脈管的後外側。進入孔的前外側可能需要麵神經移位,頸動脈岩部處理,外耳道和中耳獻祭,陰道突鑽孔。Fisch和Pillsbury所描述的方法121979年提供頸靜脈孔的上、外側和前方的顯露,包括麵神經的前移位和必要時犧牲外耳道和鼓室。從那以後,其他人對Fisch的方法進行了修改和擴展。馬佐尼和桑娜13提出了頸靜脈孔後外側暴露的經乙狀結腸入路。Tedeschi和Rhoton14介紹一種耳後經顳孔入路。Sanna等人44報告了A型顳下窩入路經髁突和隆突延伸以獲得頸靜脈球的後下內側通路。此外,各種其他手術入路的頸靜脈孔已被描述。3 - 13, 15-32 44-47內窺鏡經鼻/經上頜眶後入路是一種不常用的前路。
在我們的解剖中,外耳道、麵道和莖突根阻止了頸靜脈孔外側的完全開放。唯一不能在沒有麵神經轉位的情況下打開的區域是莖突根內側(圖5和6A)。完全切除頸靜脈孔神經鞘瘤一般不需要麵神經前轉位,否則可能導致麵神經缺損。27日,48經乳突入路,犧牲迷宮和耳蝸來擴大手術視野,很少被選擇用於頸靜脈孔神經鞘瘤,因為腫瘤切除後聽力的保存和改善是常見的。49-51
椎動脈在橫孔上升,並在寰髁或枕髁後水平運行,不需要移位。然而,切除寰椎橫突是有幫助的,因為它擴大了乙狀竇和頸內靜脈和下中樞神經後的手術視野,而不發生椎動脈易位。25日,45
不切除頸突而切除枕髁無助於打開頸靜脈窩,是不必要的。32切除髁突的後外側邊緣可能有助於暴露頸內靜脈的後內側邊緣,但切除超過後三分之一的髁突可能導致顱頸不穩定。
切除竇,結紮乙狀竇和頸內靜脈,打開頸靜脈球,用於該區域的頸靜脈球瘤,但不常被考慮完全切除阻塞竇的頸靜脈孔神經鞘瘤。6
暴露頸靜脈孔和頸靜脈球內容物的關鍵步驟是雪雨下乳突切除術和/或頸靜脈突切除術,這可能與枕下外側入路或耳後經顳孔入路和/或頸暴露相結合。根據椎間孔內腫瘤的生長方式選擇治療方法。如果腫瘤的有孔部分延伸到霰雨下區,並向下推頸靜脈球,則應加行乳突切除術。如果腫瘤延伸至後下方,則需要切除頸靜脈。頸靜脈下段和頸靜脈下段聯合切除可以為椎間孔腫瘤的切除增加更廣闊的視野。
外側枕下入路有多種術式。遠側延伸將有助於切除腫瘤向前延伸到下腦幹。20.對於顱內生長的椎間孔腫瘤,枕下外側入路可聯合雨淋下乳突切除術和/或頸突切除術。枕岩經乙狀結腸入路結合了迷路後和雪雨下乳突切除術和枕下外側入路,同時犧牲乙狀結腸竇。13該入路可切除顱內、椎間孔和頸部病變,同時保留麵神經功能和外耳道、鼓室和迷路。52如果a型(顱內)腫瘤僅向頸靜脈孔的上部有部分延伸,則頸靜脈上延伸(隻切除頸靜脈孔頂部的內側部分)可使腫瘤完全切除。26日,53最近,一種乙狀結腸後內窺鏡入路已經開發出來,該入路隻包括鑽穿內聲口以下區域的椎間孔頂部,可以完全切除腫瘤,並將腫瘤小範圍延伸至椎間孔。54
雪花雨下乳突切除術提供了沿頸靜脈球的穹窿和外側的通路。15日,55當頸靜脈窩內的腫瘤向上延伸至頸靜脈球以上或向下移位頸靜脈球而不向顱內延伸時,霰雨下乳突切除術是一個很好的選擇,但隻能提供有限的接觸腫瘤的空間,應經常與另一種方法結合以擴大暴露。對於有部分顱內延伸的B型(椎間孔)腫瘤,雪雨下乳突切除聯合乙狀竇前顯露(可使小腦縮回最小)是切除腫瘤的一個很好的選擇,該腫瘤位於聽口和頸靜脈孔之間。6日,15日,47歲
高頸暴露可使患者接觸到頸靜脈孔下方的區域,但通常結合雪雨下乳突切除術和/或頸靜脈突切除術,以治療向下延伸至頸靜脈高區域的頸靜脈孔內腫瘤,或向上延伸至頸靜脈孔的主要顱外腫瘤。這個組合,包括Kaye等人,7蘭伯特等人,22加德納等人17該入路最初被稱為雪花雨下入路,可以提供從頸靜脈球頂部到頸部的廣泛暴露(圖6B)。
頸靜脈孔神經鞘瘤常累及多個區域;A1B, B1C和D腫瘤。報道的D型腫瘤的入路是聯合入路,包括外側枕下入路和頸暴露聯合雪雨下乳突切除術和/或頸突切除術。14、18、21、23日,45幾乎所有報道的入路都增加了頸靜脈突切除。然而,先前的研究報道,經髁突頸靜脈上入路保留頸靜脈球壁通常能在腫瘤切除後保持其通暢,即使術前研究顯示其沒有流入頸靜脈球。6、56、57
一般來說,通過改良來擴大手術範圍的方法是有利的。頸部暴露結合雨淋下乳突切除和頸突切除可以提供廣闊的手術視野,並可通過各種改進進一步擴大手術視野,包括不需麵神經移位的輸卵管橋技術,這提供了更大的手術空間,並改善了腫瘤延伸到鼓室下或頸靜脈球前外側的可視性。如果腫瘤擴展到顱內,可以加行乙狀結腸後或乙狀結腸前入路。如果腫瘤向岩尖方向延伸並包圍頸岩,可能需要像Fisch的A型顳下窩入路一樣,在切除外耳道後移位麵神經。11日,12日,41歲如果需要麵神經移位,保留莖突動脈和麵神經周圍的筋膜袖套將有助於避免麵神經麻痹。然而,保持麵神經功能最有效的方法是避免打開麵神經管。如果神經鞘瘤不能與頸靜脈球或頸內靜脈分離,如果術前研究顯示通過椎間孔的血流受阻,則可以在結紮乙狀竇和頸內靜脈後獻祭頸靜脈球以擴大手術視野。
如果椎間孔神經鞘瘤向前擴展,可采用a型顳下窩入路或耳前顳下窩入路暴露椎間孔的前外側。如果腫瘤延伸到顳下窩,沿頸內動脈的岩部經咽鼓管,或延伸到岩尖的鬆質部,可考慮內鏡下經鼻/上頜經三角竇入路。然而,這種入路的應用是有限的,隻有當腫瘤占據了顳下窩,並通過後移頸動脈和頸內靜脈形成手術通道,且隻需要對翼肌進行最小程度的剝離時才應考慮。16日,36歲,37歲有椎間孔和前伸的顱內腫瘤很難接近。Sanna等人44建議將A型顳下窩入路與經頸靜脈、經髁突和經結節的延伸相結合,以治療Fisch的C2 - C4型中耳室頸靜脈副神經節瘤,並進行一些技術改進,包括使用纖維蛋白膠將麵神經前路重定向,使用Surgicel (Johnson & Johnson, Piscataway, NJ)與A型顳下窩入路相比,對s型竇進行腔外壓迫。除了上側和前外側外,這種延伸允許後下和內側進入孔。神經鞘瘤很少向前方延伸並浸潤頸動脈岩壁。然而,如果神經鞘瘤從顱內和椎間孔向岩尖和岩頸動脈擴張,則應考慮采用這種入路。
從眾多報道的入路中選擇最佳入路應基於顯示腫瘤大小和位置的術前檢查。應注意避免損傷中樞神經係統,因為頸靜脈孔神經鞘瘤大多是良性的,生長緩慢,通常造成輕微的中樞神經係統缺損。準確了解每種入路和頸靜脈孔所涉及的複雜解剖結構對於實現腫瘤的完全切除同時最小化風險是非常重要的。
貢獻者:Noritaka Komune醫學博士,Ken Matsushima醫學博士,Toshio Matsushima醫學博士,Shizuo Komune醫學博士,和Albert L. Rhoton, Jr醫學博士
內容來自Komune N, Matsushima K, Matsushima T, Komune S, Rhoton AL, Jr.頸靜脈孔神經鞘瘤的外科入路:一項解剖學研究。頭頸2016年,38:E1041-E1053。doi.org/10.1002/hed.24156.
神經外科188bet手机app圖譜很榮幸能夠繼承Albert L. Rhoton, Jr . MD的遺產。
請登錄發表評論。
一定要在社交媒體上關注我們,獲取精彩內容並保持更新生活科恩醫生的會議,關於手術技術的問題,以及更多!



您必須登錄才能查看此材料。
的188bet手机app這幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。
請承諾每年至少捐贈250美元給Atlas。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法獲得它,他們的病人的護理依賴於它。
請立即捐款!
如果沒有你們的大量捐贈,我們就無法繼續開展地圖集。請承諾每年至少捐贈250美元給Atlas。
如果沒有這個承諾,Atlas將很快需要付費訂閱世界上許多病人的護理都依賴於它的外科醫生將無法使用它。請立即捐款!