

你可以有所作為。
的188bet手机app幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈我們無法繼續製作《地圖集》。
請承諾每年至少向Atlas捐贈250美元。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法使用它,他們的病人的護理依賴於它。
請立即捐款!
最後更新:2021年6月22日
客觀的:鬆果體區病變的常見入路是沿錐體下中線入路。然而,關於將入路移離中線如何影響手術暴露和Galen靜脈支間關係的報道有限。本研究的目的是通過小腦上幕下入路檢查鬆果體區的顯微外科和內窺鏡解剖,包括中線、中間線、外側和遠側路。
方法:在手術顯微鏡和直內窺鏡的幫助下,對8例固定福爾馬林的成年屍體頭部的四叉神經池進行了解剖和檢查。檢查了20張CT血管造影,以測量鬆果體的深度,小腦的帳篷麵坡度,以及每個入路的鬆果體角度。
結果:小腦上中線路徑最短,可直接暴露鬆果體,盡管Galen靜脈的culmen和蚓下、蚓上支經常阻礙這一暴露。中線外通路提供了手術暴露,雖然略深,但可以減少從小腦上表麵進入小腦幕竇的靜脈水平和四叉神經池Galen靜脈支流水平的靜脈犧牲,並減少小腦回縮的需要。與中線入路相比,從中線到中線外暴露也能更好地觀察小腦腦裂、丘板和滑車神經。內窺鏡輔助可幫助鬆果體暴露,同時保留橋靜脈。
結論:了解通往鬆果體的不同幕下通路的特征將有助於更好地觀察鬆果體和小腦腦裂,並可能減少在引流小腦上表麵的幕下竇和Galen靜脈支流水平靜脈犧牲的需要。
小腦上幕下入路常用於涉及鬆果體的病變。1、6、10、13、32雖然中線路線經常被選擇,但在環狀肌內側和橫竇和乙狀竇橫向交界處的星形點之間,也有可能出現幾條中線外路線。中線和中線外路徑在入路深度和角度、暴露區域以及入路沿線血管結構的風險方麵存在差異。本研究檢查了通往鬆果體的各種幕下入路的顯微外科和內窺鏡解剖,包括中線、中線、外側和遠外側小腦上幕下入路。此外,本研究還確定了鬆果體的深度和小腦幕下各路徑的幕麵角度。
本研究對8例用福爾馬林固定的成人屍體頭部的後切口間隙進行了檢查。在8個灌注福爾馬林的成年屍體頭部中,有6個的動脈和靜脈被注射了紅色和藍色的矽膠。所有屍體頭部均使用手術顯微鏡和直鏡提供的3 - 40倍放大鏡進行檢查。用高速鑽頭進行骨解剖。解剖遵循外科手術的步驟。
連續20例成年患者(男6例,女14例)進行CT血管造影(CTA)以評估未破裂顱內動脈瘤,測量其與鬆果體的距離、小腦上麵斜度和入路角度。患者平均年齡為62.7歲(範圍40-82歲)。
12例使用64片東芝Aquilion 64係統(東芝醫療係統)進行CTA研究,其餘8例使用320片東芝Aquilion One係統進行CTA研究。所有影像學檢查均在九州大學醫院進行。無一例患者因顱內病變而發生腫塊效應。
成像數據采用OsiriX成像軟件5.9版(http://www.osirix-viewer.com)進行分析,采用二維多平麵重建軸向視圖進行觀察;所有軸向麵均平行於眶咽線。
在檢查不同的小腦上幕下入路(路線)時,如先前報道的那樣,小齒輪與橫竇和乙狀竇交界處之間的距離被分為三分之一。11中線路線沿著斜眼下方的中線,中線路線沿著中間和中間(中間)三分之一的交界處,外側路線沿著中間和外側三分之一的交界處,以及小腦上方毗鄰橫竇和乙狀竇交界處的遠外側路線(圖1A和B)。調整一個軸向平麵以交叉橫竇和乙狀竇的交界處(圖1A)。測量前,確定每條通路的入路點,即橫竇下方和枕骨內表麵的點(圖1C-F)。對於每條路徑,都使用一個垂直於軸向麵、與鬆果體和接近點相交的矢狀麵來測量鬆果體的深度、小腦表麵的坡度以及接近鬆果體的角度(圖1C-F)。測量鬆果體與每個接近點之間的距離,以確定每條路線的鬆果體深度。測量眼窩線與經過小腦幕麵接近點和最高點的線之間的最陡角,以確定小腦幕麵斜率(圖1C-F)。測量眶口線與經接近點和鬆果體的線之間的夾角來確定接近角(圖1C-F)。

圖。1。通過中線、中線、外側和遠外側小腦小幕下路徑測量鬆果體的深度和小腦小幕麵角度。A:橫竇和乙狀竇拐角水平的軸向CT圖像(A平麵,穿過橫竇和乙狀竇交界處的軸向平麵)。在檢查不同的小腦上幕下入路時,小齒輪和乙狀竇之間的距離被分成三份。中線路線沿中線(藍色箭頭),旁正中路線沿中間三分之二交界處(黃色箭頭),外側路線沿中間和外側三分之二交界處(綠色箭頭),遠外側路線沿小腦上方毗鄰橫竇和乙狀竇交界處(紅色箭頭)。B:小腦上幕下鬆果體手術入路右後外側視圖。圖示中線(藍色箭頭)、中線(黃色箭頭)、側線(綠色箭頭)和遠側線(紅色箭頭)。版權所有Satoshi Matsuo。已獲授權發布。C:重建的CT矢狀麵圖像,垂直於A麵板所示平麵(平麵A),與鬆果體(紅圈)和中線路線接近點(藍圈)相交。 The approach point was defined as the point just below the sigmoid sinus on the inner surface of the occipital bone. The distance between the pineal gland (red circle) and the approach point (blue circle) was defined as the depth of the pineal gland. The angle of the tentorial surface of the cerebellum was defined as the angle between the orbitomeatal plane and the line through the approach point (blue circle) and the highest point of the tentorial surface of the cerebellum (yellow circle). D: Reconstructed sagittal CT image perpendicular to Plane A and intersecting the pineal gland (red circle) and the approach point (blue circle) of the paramedian route. E: Reconstructed sagittal CT image perpendicular to Plane A and intersecting the pineal gland (red circle) and the approach point (blue circle) of the lateral route. F: Reconstructed sagittal CT image perpendicular to Plane A and intersecting the pineal gland (red circle) and the approach point (blue circle) of the far-lateral route. Gl. = gland; Infratent. = infratentorial; Lat. = lateral; Mid. = midline; Paramed. = paramedian. (Images courtesy of AL Rhoton, Jr.)
鬆果體位於脾體前部下方,第三腦室後方,丘板上方,Galen靜脈前方,枕骨之間。這個深區,也被稱為後切膜間隙,位於中腦後部,與鬆果體和Galen靜脈區域相對應(圖2和3)。
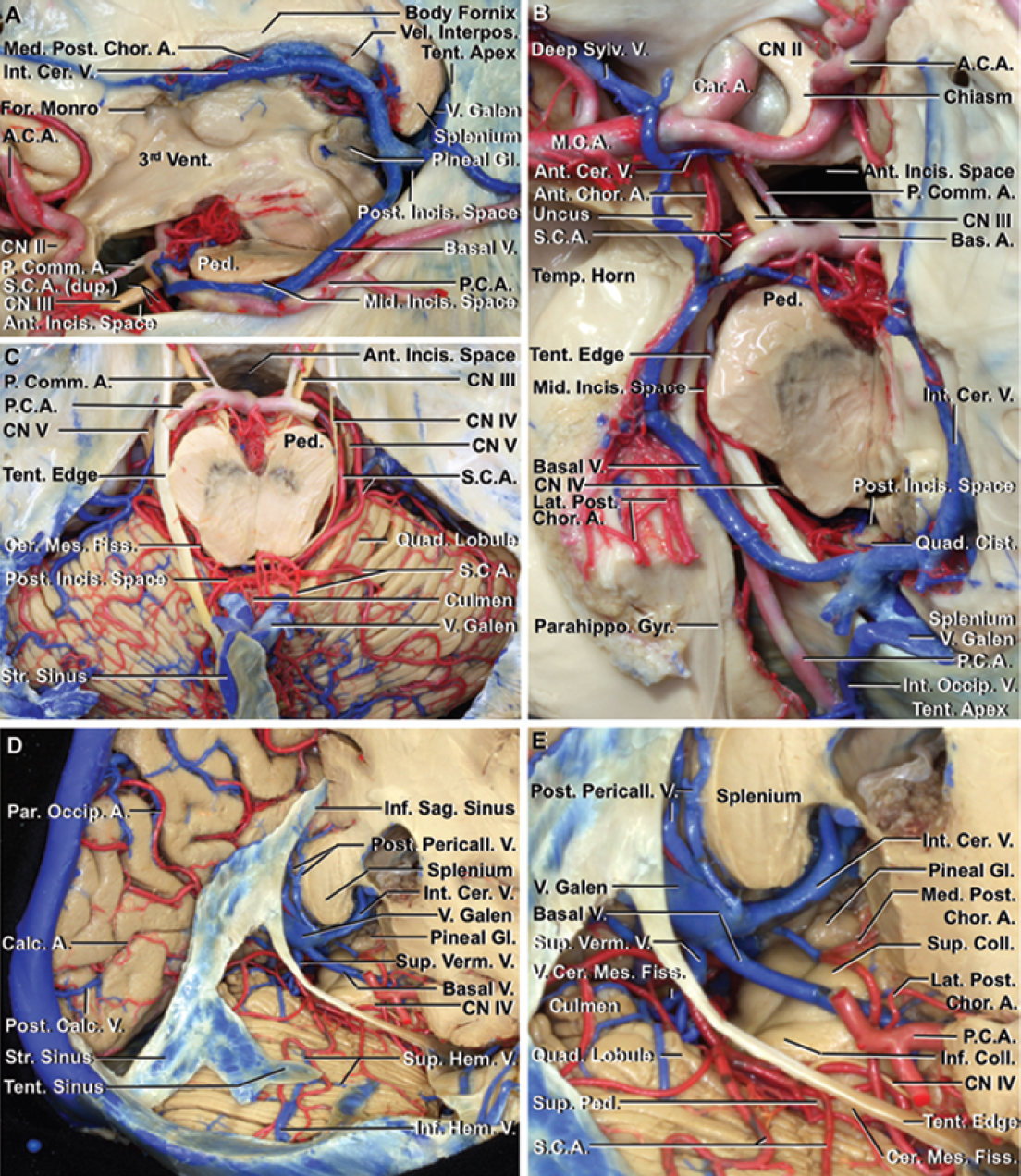
圖。2。後切口間隙的神經血管關係。A:左幕切骨側位圖。左大腦半球被切除了。小幕切骨位於小幕邊緣之間。小腦門板相對於腦幹分為前、中、後間隙。後切膜間隙,鬆果體的位置,位於中腦後和幕尖之間。腦後動脈和小腦上動脈起於前壁間隙,並繞腦幹到達後壁間隙。腦內靜脈穿過腦間膜,基底靜脈起源於前切口間隙,環繞中腦,在後切口間隙彙合,最後流入Galen靜脈。鬆果體位於第三腦室後方,Galen靜脈前方,脾前部下方,丘板上方。 B: Superior view of the left tentorial incisura after removal of all of the left cerebral hemisphere except the temporal lobe. The roof of the temporal horn and part of the parahippocampal gyrus have been removed. The basal vein, which originates in the anterior incisural space at the union of the anterior cerebral and deep middle cerebral veins, and internal cerebral vein join in the posterior incisural space and empty into the vein of Galen. C: Superior view of the tentorial incisura and cerebellum. The cerebral hemispheres and tentorium have been removed to expose the tentorial surface of the cerebellum. The distal part of the posterior cerebral artery has been removed to expose the course of the superior cerebellar artery. The superior cerebellar artery, which usually arises below the oculomotor nerve as a single trunk from the basilar artery, arises on the right side as a duplicated trunk. The superior cerebellar artery courses below the trochlear nerve and above the trigeminal nerve, to reach the cerebellomesencephalic fissure, which extends downward between the midbrain and the cerebellum. The superficial part of the posterior lip of the fissure is formed by the culmen in the midline and the quadrangular lobule laterally. After leaving the fissure, the superior cerebellar artery gives rise to the branches to the tentorial surface of the cerebellum. D: Posterolateral view of the left posterior incisural space and tentorial surface of the cerebellum. The right occipital, parietal, and temporal lobes have been removed at the level of the body of the lateral ventricle. The right tentorium has been removed to expose the tentorial surface of the cerebellum. The superior and inferior hemispheric veins drain the tentorial surface of the cerebellum and join before emptying into the tentorial sinuses. The posterior pericallosal vein, which drains the posterior part of the cingulate gyrus, empties around the splenium into the vein of Galen in the quadrigeminal cistern. E: Enlarged view. The internal cerebral, posterior pericallosal, basal, and superior vermian veins empty into the vein of Galen. The superior and inferior colliculi are located posterior and inferior to the pineal gland. The medial posterior choroidal artery courses beside the pineal gland and enters the velum interpositum in the roof of the third ventricle. The lateral posterior choroidal artery, which arises from the posterior cerebral artery, enters into the lateral ventricle through the choroidal fissure. A. = artery; A.C.A. = anterior cerebral artery; Ant. = anterior; Bas. = basilar; Calc. = calcarine; Car. = carotid; Cent. = central; Cer. = cerebral, cerebellar; Cer. Mes. = cerebellomesencephalic; Chor. = choroidal; Cing. = cingulate; Cist. = cistern; CN = cranial nerve; Coll. = colliculus; dup. = duplicate; Fiss. = fissure; For. = foramen (of); Gyr. = gyrus; Hem. = hemispheric; Incis. = incisural; Inf. = inferior; Int. = internal; Interpos. = interpositum; M.C.A. = middle cerebral artery; Med. = medial, medullary; Mid. = middle; Occip. = occipital; P.C.A. = posterior cerebral artery; P. Comm. = posterior communicating; Par. = parietal; Parahippo. = parahippocampal; Ped. = peduncle; Pericall. = pericallosal; Post. = posterior; Quad. = quadrigeminal, quadrangular; S.C.A. = superior cerebellar artery; Sag.= sagittal; Str. = straight; Sulc. = sulcus; Sup. = superior; Sylv. = sylvian; Temp. = temporal; Tent. = tentorium, tentorial; V. = vein (of); Vel. = velum; Vent. = ventricle; Verm. = vermian. (Images courtesy of AL Rhoton, Jr.)

圖。3。後切口間隙的神經關係。A:切除左腦半球、小腦和腦幹後切牙間隙的矢狀麵。後切間隙的前壁由鬆果體、上、下丘和蚓舌組成。後切口空間的屋頂由脾下表麵和穹窿體後部組成。後切間隙的底部由蚓部的頂部和中央小葉組成。後切間隙向下延伸至小腦腦裂。B:右半腦幹在上丘水平切除後的右後上視圖。韁肌和後連肌形成了腺體與第三腦室後部的連接。枕骨、穹窿小腿和海馬旁回構成後切口空間的側壁。 C: Inferior view of the medial temporal lobe and lateral wall of the posterior incisural space. The brainstem and cerebellum have been removed. The pulvinar, located just lateral to the pineal body, and the crus of the fornix, located posterior to the pulvinar, form the lateral wall of the posterior incisura space. Cer. Mes. = cerebellomesencephalic; Coll. = colliculus; Comm. = commissure; Hab. = habenular; Hippo. = hippocampal; Mam. = mammillary; Tr. = tract. (Images courtesy of AL Rhoton, Jr.)
除後方外,硬膜後間隙均被神經組織包圍。前壁由鬆果體、上丘和下丘、蚓舌和小腦上梗按從口側到尾側的順序形成(圖2A、2D、2E和3)。帽簷連接形成上、後連接,即腺體與第三腦室後部的下部連接(圖3B)。前壁位於丘板下方的中間部分由蚓舌、蚓的最上麵部分、外側部分由小腦上梗構成(圖2E和3A)。後切口空間的頂部包括脾下表麵、穹窿底端和位於底端之間的海馬連脊(圖2A、2D、2E、3A和3B)。後切口空間的底部由內側蚓部和中央小葉的culmen和外側半球的四邊形小葉構成(圖2D、2E和3A)。後切間隙向下延伸至小腦腦裂(圖1F)。外側壁由枕骨、穹窿小腿和脾以下的大腦半球內側表麵構成(圖3B)。枕骨位於鬆果體的外側(圖3C)。穹窿的腳形成了枕骨後的外側壁(圖3B和C)。外側壁的後部由海馬旁回和齒狀回形成(圖3B和C)。24
大腦後動脈和小腦上動脈及其分支都穿過後切口。腦後動脈起於顱底分叉,環繞中腦,穿過腳池和周圍池,到達後壁間隙,通常分叉為其末端分支,鈣動脈和頂枕動脈,在其穿過幕頂遊離邊緣的附近(圖2D)。24日,34小腦上動脈起於基底動脈頂端附近,經過動眼神經下方,並環繞腦幹(圖2A-C)。動脈經過滑車神經下方和三叉神經上方進入小腦腦裂(圖2C)。離開裂隙後,動脈產生分支,供應小腦幕麵(圖2D和E)。小腦上動脈通常以單幹形式出現,但也可能以雙幹形式出現(圖2A-C)。21大腦後動脈供應上丘下緣以上的結構,小腦上動脈供應下丘上緣以下的結構。24
腦內靜脈、基底靜脈和Galen靜脈及其支流穿過後切膜間隙(圖2A、B、D、E)。腦內靜脈起於Monro孔後方,穿過腦間膜進入後切膜間隙,在此靜脈與對側夥伴彙合形成Galen靜脈(圖2A、B、D、基底靜脈起源於大腦前靜脈和Sylvian深靜脈的結合(圖2B)。基底靜脈在後側中腦和顳葉之間,到達後切膜間隙,流入腦內靜脈或Galen靜脈(圖2A, B, D, E)。22前鈣質靜脈,又稱枕內靜脈,引流楔形和舌前部,並流入蓋倫靜脈。22後胼胝體周圍靜脈,引流扣帶回後部,經脾部流入四叉神經池的Galen靜脈或腦內靜脈(圖2D和E)。22腦窩靜脈引流腦窩板,並向後排入小腦腦裂靜脈、Galen靜脈或蚓上靜脈(圖4C、4D和5)鬆果體靜脈起源於鉤狀三角區附近,向後向鬆果體上或下外側延伸,流入腦內靜脈或Galen靜脈(圖4C、4D和5)。2Galen靜脈經過脾下,排空至幕尖的直竇(圖2A、2B、2D和2E)。Galen靜脈與直竇的交界處,如果幕尖位於脾下,則接近平坦,如果幕尖位於脾上,則形成一個銳角,因此Galen靜脈必須急劇向上轉,才能到達幕尖的直竇。22

圖。4。中線(A和B)和右中線(C和D)小幕下小腦上顯微手術和內鏡入路到鬆果體。A:鬆果體顯微中線入路。打開四叉神經池,可以看到蚓上靜脈、枕內靜脈、基底靜脈、腦內靜脈和Galen靜脈。在中線入路中,可能需要收縮或犧牲蠕蟲上靜脈以暴露鬆果體區。B:內窺鏡中線入路。C:鬆果體右側旁位顯微外科入路。在蚓上靜脈和腦內靜脈之間可暴露鬆果體和上、下丘,而不犧牲靜脈。腺體的離中線視圖打開了腺體周圍大靜脈之間的視角。D:內鏡輔助入路。 The pineal gland can be exposed between the galenic tributaries. Retracting the cerebellum can provide access to the superior and inferior colliculi. Coll. = collicular, colliculus; Med. = medial; Tent. = tentorial, tentorium. (Images courtesy of AL Rhoton, Jr.)
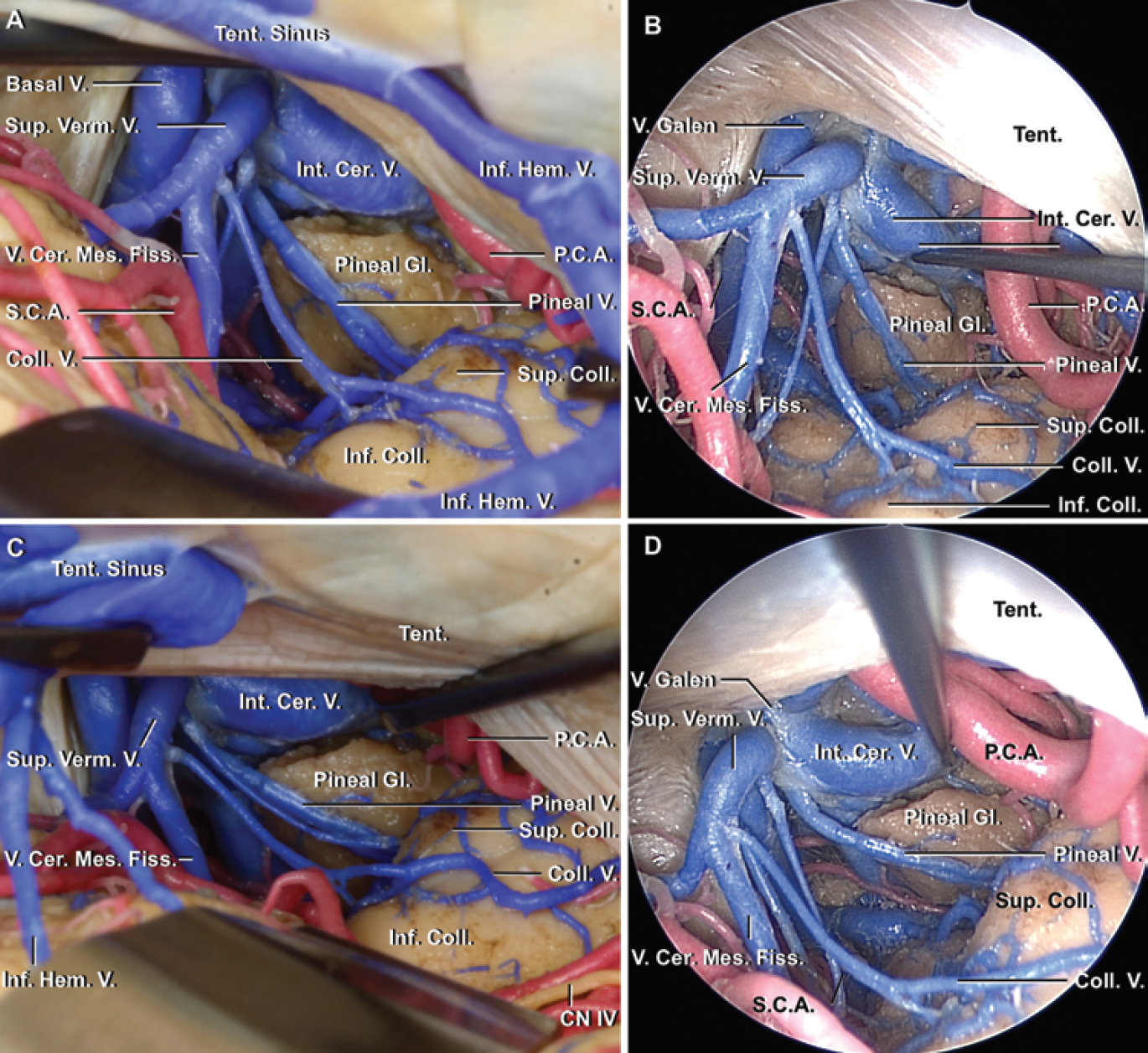
圖。5。右側(A和B)和遠側(C和D)小幕下小腦上顯微外科和內窺鏡入路到鬆果體。A:鬆果體右側顯微外科入路。注意,中線外入路允許暴露在半球靜脈之間,在淺層流入幕竇,在Galen靜脈水平前於蚓上靜脈。B:內窺鏡側入路。C:鬆果體右側遠側顯微手術入路。進路向外側移動得越遠,蚓上靜脈與腦內靜脈之間的進路就越寬。D:內鏡遠側入路。Cer。=腦; Cer. Mes. = cerebellomesencephalic; Coll. = collicular, colliculus; Tent. = tentorial, tentorium. (Images courtesy of AL Rhoton, Jr.)
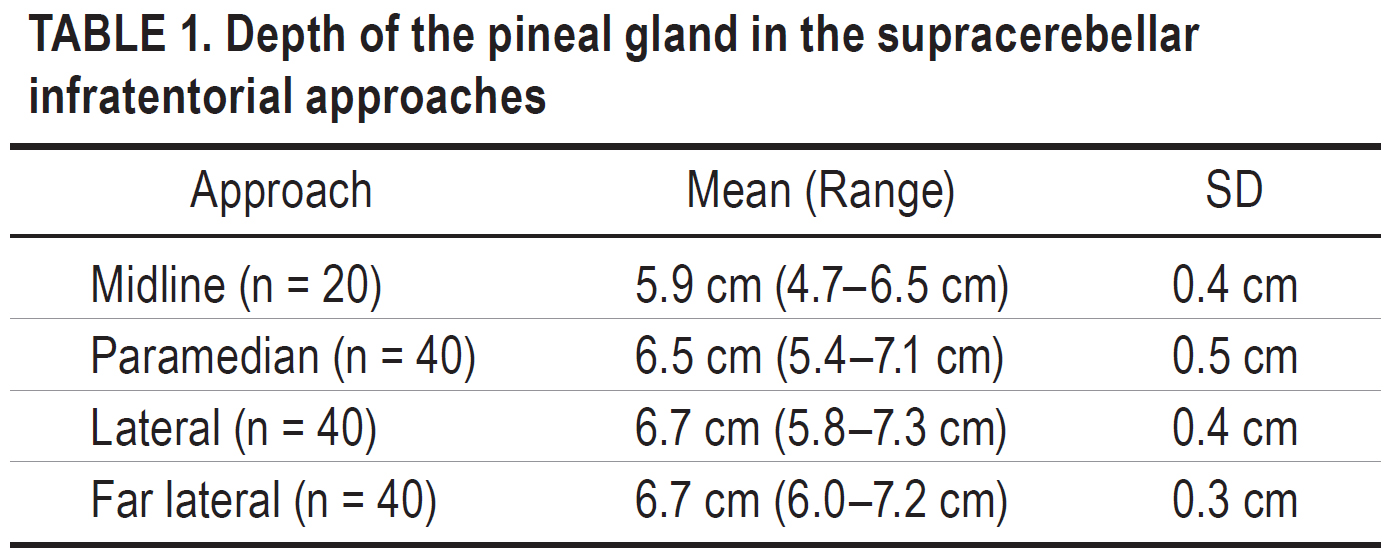
4條路徑中,錐體中線以下鬆果體深度最短(平均[±SD] 5.9±0.4 cm,範圍4.7 ~ 6.5 cm;3條中線外路徑深度基本相同,均比中線進路深度大於5mm(表1)。中線進路幕麵坡度平均值為35.2°±6.9°(範圍21.0°-46.8°),是4條進路中坡度最陡的一條。隨著入路側向移動,入路夾角逐漸減小(表2)。中線入路的入路夾角均值為20.3°±5.8°(7.6°-30.1°),與中間入路和外側入路的入路夾角均值基本相同,而遠側入路的入路夾角均值最大(24.0°±3.3°,17.1°-29.6°;表3)。


幕下入路位於上方的大腦後動脈幹和下方的小腦上動脈幹之間(圖4和圖5)。大腦後動脈幹大部分位於幕上,但從上方與硬膜間隙重疊,小腦上動脈幹主要在小腦裂鬆果體下方和幕表麵。這些血管不穿過鬆果體的後方,除非它們彎曲或拉長。在去除鬆果體病變時,大腦後、小腦上和脈絡膜動脈的小神經分支,包括丘、丘腦和鬆果體,比大動脈幹的風險更大。
在幕下入路的2個水平處遇到明顯的靜脈幹。第一個是在流經小腦的靜脈的水平穿過幕下空間流入幕下竇流入torcula,直竇和橫竇。第二個是在四叉神經池的水平,這裏有多個Galen靜脈的大支流圍繞著腺體(圖4、5和6)。
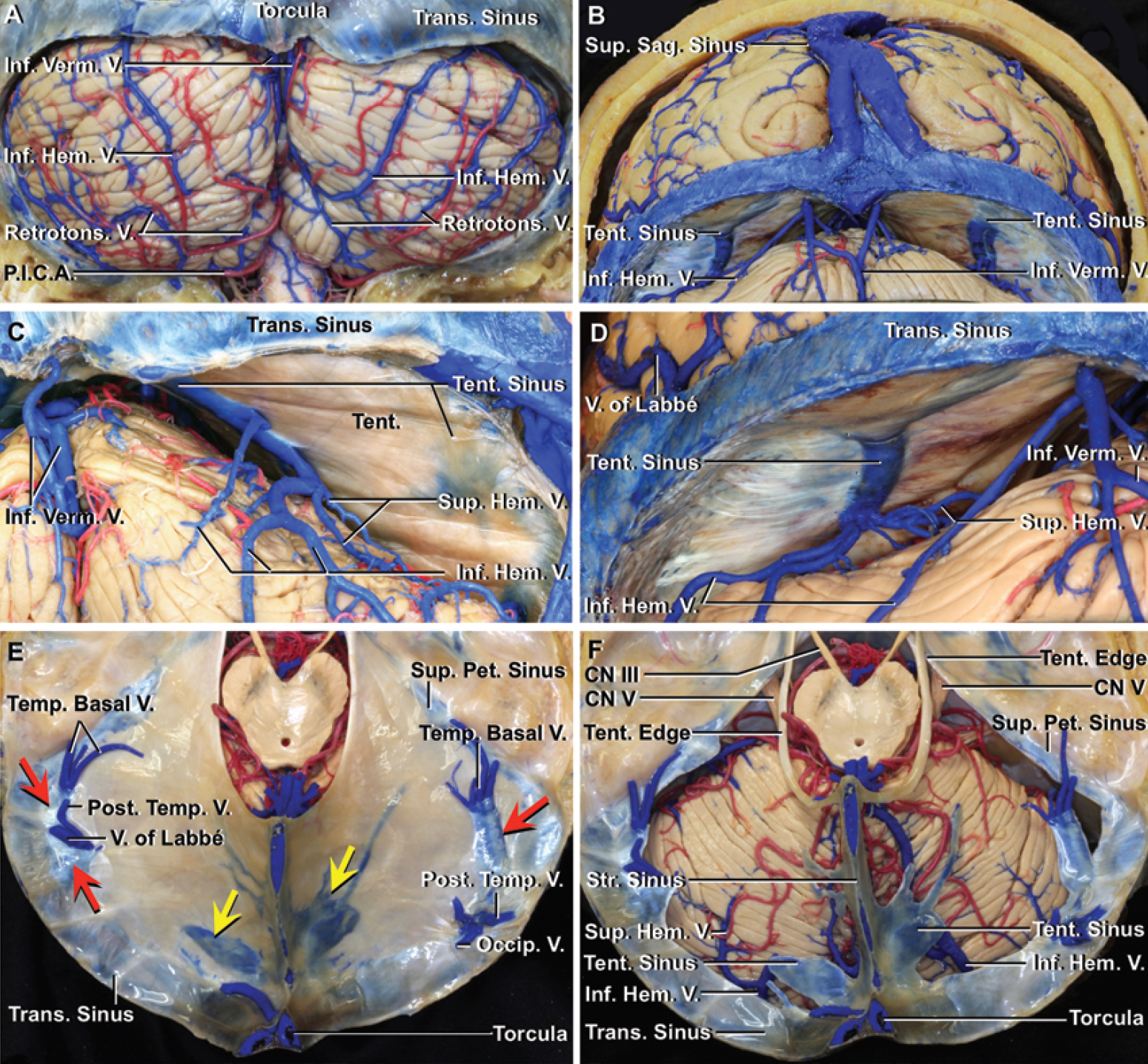
圖。6。小腦上幕下鬆果體顯微手術入路。A:小腦枕下表麵。扁桃體後靜脈上行與蚓下靜脈彙合,蚓下靜脈沿蚓半球裂隙上行並流入橫竇靠近眼眶和中線。下半球靜脈上升進入幕內靜脈竇。右下半球靜脈與扁桃體後靜脈吻合。B:帳篷下方的後視圖。蚓下靜脈引流扁桃體、蚓下和半球的鄰近部分,並流入中線附近的橫竇。上、下半球靜脈引流枕下麵和小腦幕麵,並流入幕下竇,其可流入直竇(C)或橫竇(D)。兩組半球橋靜脈之間的離中線幕下入路通常可進入鬆果體,而不損害任何橋靜脈。而中線入路通常需要明顯的回縮或閉塞這些橋靜脈。 C: Posterior view beneath the right half of the tentorium. The superior and inferior hemispheric veins drain the suboccipital and tentorial cerebellar surfaces and empty into a tentorial sinus, which empties into the straight sinus in the posterior fossa. D: Posterior view beneath the left half of the tentorium. The superior and inferior hemispheric veins drain the suboccipital and tentorial cerebellar surfaces and empty into a tentorial sinus that empties into the transverse sinus. E: Superior view of the tentorium. The cerebral hemispheres have been removed while preserving the tentorium. Each half of the tentorium has 2 tentorial sinuses. The medial tentorial sinuses (yellow arrows) course medially to empty into the straight sinus near the junction of the straight and transverse sinuses. The lateral tentorial sinuses (red arrows), formed by the union of veins from the basal and lateral surfaces of the temporal and occipital lobes, including the vein of Labbé and temporobasal and occipital veins, course laterally to empty into the terminal portion of the transverse sinus. F: Superior view of the tentorial cerebellar surface. The tentorium has been removed while preserving the tentorial edges and the tentorial, superior petrosal, straight, and transverse sinuses. The medial tentorial sinuses formed by the union of the superior and inferior hemispheric veins course medially to empty into the torcula or straight sinus. P.I.C.A. = posterior inferior cerebellar artery; Pet. = petrosal; Retrotons. = retrotonsilar; Tent. = tentorial, tentorium; Trans. = transverse.
硬腦膜打開後,通常可以看到橫跨小腦幕麵和幕下竇之間幕下空間的橋靜脈(圖6)。26即使分裂數量有限的這些靜脈也可能導致嚴重的小腦腫脹和並發症,如出血性梗死,因為大麵積的引流。1、7、19在中線入路中,通向眼眶和直竇的橋靜脈可能需要縮回或清除,以達到四叉神經池和腺體。到達四叉神經池後,來自上蚓部和小腦裂的Galen靜脈的支流會在鬆果體正下方遇到,並可能沿中線阻塞鬆果體的暴露(圖4A和B)。18日,23日,26歲在中線外入路中,引流小腦幕麵前部的半球上靜脈和上行穿過枕部和小腦幕麵邊緣的枕下靜脈經常彙合形成引流小腦大部分的橋靜脈。這些大的橋靜脈通常沿外側離中線幕下通路流入幕內中間三分之一的幕竇(圖6B-F)。15日,26日這些橋靜脈在中間和遠外側中線外入路比在外側入路更不容易遇到。然而,這些橋靜脈的位置有相當大的變異性,而中線外的路徑最有可能使它們得以保存。17日,26日,29歲從中線外路徑中選擇可以避免或減少靜脈犧牲的需要。17日,29日
解剖環繞四神經池的蛛網膜,可見由Galen靜脈支流形成的第二層靜脈,它阻斷了通往鬆果體區的通道。Galen靜脈的這些支流,包括上vermian和小腦裂靜脈,從中線的下方向接近Galen靜脈,其他如腦內靜脈和基底靜脈,從靠近中線的上方到達Galen靜脈(圖2A, 2B, 2D, 2E, 4, 5)。蚓上靜脈和小腦上靜脈在鬆果體下方一條高於另一條,如果入路嚴格沿著中線,可能需要收縮或犧牲(圖4和5)。將入路稍微側向偏離中線可避免犧牲這些靜脈。離中線入路的一個優點是,當它們向外側移動得更遠時,它們打開了位於下方的腦小腦裂與上方的腦內靜脈之間的夾角,並提供了通往腺體的通道,通常沒有靜脈犧牲,除了可能的小支流,如鬆果體靜脈,直接從鬆果體和鄰近的神經結構流出(圖4和圖5)。
眾所周知,在中線附近小腦culmen和四邊形小葉的突出限製了儀器的工作角度,並幹擾了鬆果體深度的充分照明,小腦上表麵通過每條路徑的深度和坡度都會影響手術的可操作性。然而,這些不同的深度和坡度以前並沒有被確定。我們發現離中線路徑之間的深度差異隻有幾毫米,盡管離中線路徑比中線路徑深5毫米以上,從而提供了最短的進路。另一方麵,每條路徑的小腦上(幕)麵坡度隨著入路從內側向外側移動而發生顯著變化。在幕下入路中,中線入路的坡度大約是外側和遠側入路的兩倍。我們還發現,中線和中線路線的小腦(幕)麵斜率大於這些進路的角度。相比之下,側路和遠側路的小腦(幕)麵坡度小於這些入路的角度。因此,中線和中線路線比外側和遠側路線需要更大的小腦回縮以接近鬆果體。離中線路線,特別是通過中間或外側三分之一的幕,需要較少的小腦回縮到達鬆果體。然而,根據我們之前的研究,經過中間三分之一的路徑需要犧牲小腦上表麵到幕竇的橋靜脈的風險更高。15日,26日
小腦上幕下入路是鬆果體病變的常用入路。6、10、13、32傳統的鬆果體幕下入路是沿著圓錐體下的中線,25但它需要更大的小腦回縮比中線外入路,由於高度的梗。中線外幕下小腦上入路,即中間路、外側路和遠外側路,已被開發出來,以最大限度地減少小腦回縮的需要,並促進後切口空間的不同部分的暴露。8、12、14、17、19、20、28、30、31鬆果體病變選擇中間和外側路徑,後外側中腦病變而非鬆果體病變選擇遠外側路徑。14日,30Komune等人。11報告了遠側小腦上幕下入路至下丘,包括無幕下切口的枕下側開顱術。在這項研究中,我們發現鬆果體也可以通過遠側入路進入,直接靠近橫竇和乙狀竇。離中線入路的優點還在於可以更直接地看到沿小腦腦裂前壁的結構,如丘板和第四腦神經。更外側入路的一個缺點是,枕骨可能隱藏鬆果體區域的一部分,並防止接觸到第三腦室頂部丘腦兩半之間鬆果體中線向前延伸的病變。
供應鬆果體區域的小腦上動脈和大腦後動脈的主幹在接近鬆果體區域時通常不像靜脈那樣有很大的風險,因為這些動脈不穿過鬆果體的後方,而靜脈在接近鬆果體區域時有更大的風險。主要的動脈風險是大腦後、小腦上和進入四叉神經池邊界的脈絡膜動脈的小穿孔分支。
犧牲上蚓靜脈、半球靜脈或蚓靜脈橋靜脈被認為是相對安全的。5、6、10、20Kodera等人。10報道如果保留每條靜脈的側支循環,這些靜脈可以被犧牲。然而,Page等人。18報告一例嚴重小腦腫脹後犧牲半球和蚓橋靜脈通過中線入路。Jakola等人。7報道即使犧牲有限數量的小腦幕橋靜脈也可能引起靜脈梗死或小腦出血。14雖然小腦和幕靜脈係統的解剖學關係已經被很好地研究,但在術前或手術中尚不可能確定哪些靜脈可以被犧牲。15日,16日,23日,26歲即使術前靜脈造影也隻能識別屍體研究中所見靜脈數量的一半。4為了避免危險的並發症,在指導入路時,應考慮將橋靜脈的犧牲限製在最小數量和最小尺寸的靜脈。通常,這些小靜脈連接形成橋靜脈進入小腦幕竇,如果阻塞可能犧牲大麵積的小腦引流。腦收縮聯合靜脈犧牲比單獨使用任何一種都有更高的腦損傷風險。9為了避免危險的並發症,在指導手術方法時,減少腦內縮回的需要應該是一個考慮因素。內窺鏡下小腦上幕下入路需要較少的小腦回縮,可能有助於在不犧牲橋靜脈的情況下接近鬆果體病變。
常見的鬆果體病變的手術暴露是通過垂直枕下中線切口。通過這個切口,橫竇下方和中線附近的骨暴露可以向外側延伸,進入兩側的旁正中和相鄰外側入路。另一種進入小腦上表麵遠外側部分的常見入路是乙狀竇後入路,通過該入路,骨骼暴露可以向內側延伸,以利用外側入路,這取決於與進入幕竇靜脈相關的靜脈結構。此外,在中位旁入路和外側入路時,乙狀結腸後切口可從通常的星號下方中心位置向內側移動。另一種方法是利用一側的中外側、外側和遠外側入路,從乳突區沿著上頸線向上延伸到torcula,然後在中線向下延伸。大多數鬆果體腫瘤通過中線切口進入。然而,采用中線外入路有明顯的優勢,它減少了在幕橋靜脈和四叉神經池水平上犧牲靜脈的可能需要。
內窺鏡幕下小腦上入路已應用於鬆果體囊腫、表皮樣和星形細胞瘤等病變,3、27它被認為是顯微鏡下鬆果體的另一種方法。33最近,Hasan等人。33通過測量手術自由度定量研究了內窺鏡和顯微外科小腦上幕下入路。他們報告說,他們的側路,我們在本研究中稱為遠側路,提供了最大的手術暴露和最大的垂直攻擊角度,而中線路在通過內窺鏡小腦上幕下入路接近鬆果體時提供了最大的水平角度。33內窺鏡下小腦上幕下入路需要更少的小腦收縮,並可能在不犧牲橋靜脈的情況下幫助接近鬆果體病變(圖4B, 4D, 5B和5D)。
小腦上幕下入路,包括中、中、側和遠側入路,為大多數涉及鬆果體的腫瘤的切除提供了途徑。了解小腦上幕下入路的差異,包括入路深度和角度的差異,選擇需要在小腦上方幕下間隙和四叉神經池分別劃分最少數量橋靜脈的入路,可以減少術後並發症。內窺鏡下小腦上幕下入路對接近鬆果體也有幫助,特別是在確定一條最小化靜脈犧牲的路徑方麵。
貢獻者:Satoshi Matsuo, MD, Serhat Baydin, MD, Abuzer Güngör, MD, Koichi Miki, MD, Noritaka Komune, MD, PhD, Ryota Kurogi, MD, Koji Iihara, MD, PhD和Albert L. Rhoton, Jr, MD
內容來自Matsuo S, Baydin S, Güngör A, Miki K, Komune N, Kurogi R, Iihara K, Rhoton AL, Jr.鬆果體中線和中線外幕下小腦上入路。J Neurosurg2017; 126:1984 - 1994。doi.org/10.3171/2016.7.JNS16277.
神經外科188bet手机app圖集很榮幸能夠保持Albert L. Rhoton, Jr, MD的遺產。
請登錄發表評論。
請務必在社交媒體上關注我們,獲取令人興奮的內容,並保持更新生活科恩醫生的會議,關於手術技術的問題,以及更多!



您必須登錄才能查看此資料。
的188bet手机app幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈我們無法繼續製作《地圖集》。
請承諾每年至少向Atlas捐贈250美元。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法使用它,他們的病人的護理依賴於它。
請立即捐款!
如果沒有你們的大量捐贈我們無法繼續製作《地圖集》。請承諾每年至少向Atlas捐贈250美元。
如果沒有這個承諾,Atlas將很快需要付費訂閱世界各地的許多外科醫生都無法使用它,他們的病人的護理都依賴於它。請立即捐款!