
![圖6.13。經口入路是最常用的前路入路。經口入路的變體包括經齶入路,其中軟齶或軟齶和硬齶都打開,唇頜或唇舌下頜入路,其中嘴唇、下巴、下頜骨,可能還有舌頭和口腔底部在中線分開,以增加暴露。經口入路及其變體允許切除斜坡、寰椎前弓、齒狀突以及C2和C3椎體。A,經口入路。患者頭部固定,以便進行側位x線或圖像強化檢查以確認位置。通常進行氣管造口術。導管通過鼻道插入並置於軟齶後麵並從口腔中取出或通過小舌底部的絲狀縫線連接到鼻導管可以用來收回軟齶。咽後壁在中線縱切(斷線)。B,粘膜和肌肉作為單層向外側縮回,使用骨膜下剝離到達寰椎、軸和下斜坡。 The anterior arch of the atlas, the odontoid process, and the body of the atlas may be removed (interrupted line) to expose the dura. C, it may be necessary to split the soft palate in the midline to expose the clivus (palatal incision, continuous line; pharyngeal incision, interrupted line). D, the anterior surface of the clivus has been exposed through the transpalatal approach. The anterior arch of the atlas and the odontoid process may be removed and an opening made in the clivus (interrupted line). E, if further craniad exposure is needed, laterally based mucoperiosteal flaps may be elevated from the lower surface of the hard palate (interrupted line), and the soft palate split in the midline (continuous line). The posterior part of the hard palate may be removed (oblique lines). F, care is taken to retract rather than open the mucosa lining the upper surface of the hard palate. The pharyngeal incision is extended upward through the vault of the nasopharynx to the posterior border of the vomer. When elevating the mucoperiosteal layer from the clivus, the lateral margins slope dorsally into gutter-like depressions where the tissue becomes more adherent. The clivus, anterior arch of the atlas, dens, and bodies of C2 and C3 may be removed. The clival defect is packed with muscle or fat and may be reinforced with a bone graft. The prevertebral muscle and mucosal layers and the palatal openings are closed with absorbable sutures. G, the lower lip and mandible may be split (interrupted line) to increase the exposure and reduce the operative depth. H, a step-like mandibular osteotomy (interrupted line) is accomplished in the midline after removal of a central incisor tooth. I, spreading the mandibular halves laterally without splitting the tongue permits the tongue to be depressed downward between the mandibular halves. J, if the exposure is still inadequate, the tongue and floor of the mouth may be split in the midline. Spreading the mandibular-lingual halves exposes the pharynx down to the C3 level. The mucosa and musculature of the tongue and floor of the mouth are reapproximated; the mandibular osteotomy is closed with plates; and the lip, chin, and submandibular region are carefully closed after dealing with the lesion. (From, Rhoton AL Jr, de Oliveira E: Anatomical basis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction. New York, Thieme, 1998, pp 13–57 [26].)](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Foramen_magnum_6.13.jpg)
![圖6.16。Transmaxillary方法。示出三種經上頜入路。這三種手術都可以通過口腔內切口脫手套完成。另一種類型的切口延伸到麵部,如Weber-Fergusson切口,可以考慮。A,抬高上唇,沿著臼齒周圍的上牙槽邊緣切開黏膜。粘膜從上頜骨的前側麵抬升到眶下孔以下,但要高到足以避開牙根。黏膜從上頜骨的鼻表麵抬高,鼻中隔在其與上顎的附著處上方分開。B,鋸切(實線)延伸至兩側上頜竇。上頜骨的遊離塊向下移動(箭頭),以便進入斜坡。 C, the intraoral retractor has been placed. Displacing the maxilla downward gives wide access to the clivus. D, a modified technique, called the extended maxillectomy, includes the LeForte I osteotomy with a midline incision of the hard and soft palate (solid lines). E, this allows the halves of the maxilla, which are attached to the muscles and vessels in the infratemporal fossa, to be reflected laterally, providing wider exposure to the clivus and upper cervical spine. F, retractors have been placed to expose the clivus and upper cervical area. The approach can be extended upward into the sphenoid and ethmoid sinuses and downward to C2 or C3. G–I. Unilateral maxillotomy. G, in this approach, half of the maxilla is mobilized by a bone cut, which extends back to the infratemporal fossa in the area just below the infraorbital foramen, and the maxilla is divided in the midline. A mucosal incision is made along the low surface of the hard palate parallel to the midline on the side opposite the saw cut through the hard palate, and the anterior face of the maxilla is degloved on one side. The soft palate is left intact. H, the unilateral block of maxilla, which is still attached to the structures in the infratemporal fossa along the pterygoid plates and to the soft palate, which is not interrupted, is folded downward into the floor of the mouth. I, the anterior part of the nasal septum is left undisturbed, but the posterior part is removed along with some of the turbinates and wall of the sinuses to provide a wide exposure of the clivus. This exposure can be enlarged to include the walls of the sphenoid and ethmoid sinuses. (From, Rhoton AL Jr: Anatomical basis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].)](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Foramen_magnum_6.16.jpg)
![圖6.18。A,經頸入路。氣管切開術可以使下顎緊緊閉合。t型皮膚切口(間斷線)包括從乳突尖端延伸至
門蒂聯合的下頜下切口和向下延伸至胸鎖乳突肌的下延伸。B,可切除區域(斜線)包括斜坡、軸的前弓、軸的齒狀突體。C,
暴露指向胸鎖乳突肌的前邊界和外側
內頸動脈和頸內靜脈之間,以及內側的食管、下咽和氣管。可以劃分為增加暴露的結構包括咽升動脈和甲狀腺上動脈,喉外神經,舌下神經,喉內神經,舌動脈,舌下神經,莖突舌骨肌,二腹肌前腹,莖突舌骨韌帶,舌咽神經,莖突咽肌和莖突舌骨肌。副神經在胸鎖乳突肌後麵。D,椎前筋膜、頭長肌和頸長肌在斜坡到C3的中線分離,並使用骨膜下剝離術向外側縮回,露出斜坡、寰椎和軸的腹側。E和F,寰椎前弓和齒狀突,以及從枕骨大孔延伸至蝶枕軟骨聯合的2.5 mm寬斜坡可被切除。 The basilar, vertebral, and anterior spinal arteries are exposed in the dural opening. After dealing with the pathology, the dura is closed, muscle and fat are placed in the clival window, and the prevertebral and fascia are sutured in the midline. (From, Rhoton AL Jr: Anatomical basis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].) A., artery; Ant., anterior; Bas., basilar; Car., carotid; Ext., external; Inf., inferior; Int., internal; Jug., jugular; M., muscle; Sp., spinal; Sup., superior; V., vein; Vert., vertebral.](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Foramen_magnum_6.18.jpg)

你可以有所作為。
的188bet手机app幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈我們無法繼續製作《地圖集》。
請承諾每年至少向Atlas捐贈250美元。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法使用它,他們的病人的護理依賴於它。
請立即捐款!
最後更新:2021年5月4日
枕骨位於枕骨中,枕骨有三部分:位於枕骨大孔後的鱗狀部分;位於枕骨大孔前麵的基底(斜坡)部分;以及連接鱗狀部和斜坡部的髁狀部(圖6.1)。枕下入路通過鱗片部分,前入路通過斜坡部分。髁突部分,包括枕髁、頸靜脈孔後緣和舌下管,在遠側入路和遠側入路章節中所述的髁突經、髁後和髁上病變中暴露。枕骨大孔病變累及的結構包括顱下神經和脊神經上神經、尾側腦幹和脊髓口側、椎動脈及其分支、顱椎交界處的靜脈和硬腦膜竇,以及連接寰椎、軸和枕骨的韌帶和肌肉(5,26)。枕骨大孔最常從後經枕下和上頸區或從前經鼻腔和口腔、咽或上頜骨入路。

在規劃枕骨、寰椎和椎軸入路時必須考慮的骨結構。
枕骨環繞枕骨大孔(圖6.1)。椎間孔開口呈橢圓形,後寬於前。較寬的後部傳遞髓質,較窄的前部位於齒狀突上方。枕骨分為位於枕骨大孔上方及後方的鱗狀部分、位於枕骨大孔前方的基底部分和位於枕骨大孔外側的成對髁狀部分。
鱗狀部分是位於枕骨大孔上方和後麵的一個內部凹板。它的上緣與頂骨通過羊羔骨縫合線相連它的下緣與顳骨的乳突部分通過枕乳突縫合線相連。凸起的外表麵有幾個突起,頸部的肌肉附著在上麵。最大的突起,即外枕突,位於外表麵的中心部分。小齒輪位於枕內隆突尖端以下平均1厘米和矢狀竇和橫竇彙合處的下緣。兩條平行的脊從隆起處向外側輻射:最高的頸線是較薄的上脊,上頸線是較低的較突出的脊。頸線以下的區域粗糙且不規則,是許多肌肉附著的部位。一個垂直脊,即枕外脊,從枕外隆突向下延伸至枕骨大孔後緣的中點。頸下線從脊的中點向外側延伸。
鱗狀部分的內部表麵是凹的,並在其中心附近有一個突出,即枕內隆突。內表麵被上矢狀竇溝(從突起處向上延伸)、枕內脊溝(從突起處向下延伸的突出脊)和橫竇成對溝(從突起處向外側延伸)分為四個不等的窩。右側橫竇溝通常比左側大。上兩個窩適應於枕葉的兩極。下兩個窩與小腦半球的輪廓一致。枕內脊在枕骨大孔上方分叉,形成成對的下肢,沿枕骨大孔後緣兩側延伸。下肢之間的凹陷,蚓窩,被蚓的下部所占據。小腦鐮沿內枕脊附著。
枕骨的基底部分,也被稱為斜坡,是一塊向前向上延伸的厚四邊形骨板,與枕骨大孔成45°角。它在蝶枕聯合處與蝶骨相連,就在鞍背下方(7)。斜坡的上表麵是左右凹的,並由岩石斜坡裂縫從兩側與顳骨的岩部分開。這個裂隙的上表麵有岩下竇,並在頸靜脈孔後方結束。在基底部的下表麵,在枕骨大孔前,有一個小突起,即咽結節,與咽的纖維縫相連。
成對的外側或髁狀部分位於枕骨大孔的兩側。枕骨髁與寰椎相連,從這部分的外表麵突出。這些髁位於枕骨大孔前半部分外側。它們呈橢圓形,向下凸,麵朝下和橫向,長軸指向前方和內側。結節附著於齒狀突的鼻翼韌帶,位於每個髁突的內側。舌下管,傳遞舌下神經,位於髁突上方,從顱後窩向前方和外側延伸。椎管可被骨隔部分或完全分割。在6%的幹顱骨中,在一側或兩側發現隔裂的舌下管(15)。
髁突窩是位於髁突後方外表麵的一個凹陷,常穿孔形成髁突後管,通過髁突後管有一導靜脈連接椎靜脈叢和乙狀竇。一個或兩個髁突孔可能缺失或不完全穿孔(9)。頸靜脈突是一塊四邊形的骨板,從髁突的後半部分向外側延伸,形成頸靜脈孔的後邊界。它是枕骨的髁突和鱗狀部分之間的橋梁。頸靜脈突與顳骨的頸靜脈表麵橫向相連。在髁突的顱內表麵有一個橢圓形的突起,頸靜脈結節,位於舌下管的上方,岩斜裂隙的下部內側。結節的尾部常表現為舌咽神經、迷走神經和副神經經過的淺溝。乙狀結腸竇的溝槽在頸內突的上表麵向內側向前彎曲,繞著一個向上的鉤狀突,在頸內孔結束。後髁管通向後顱窩靠近乙狀結腸竇槽的內側端。
頸靜脈孔位於髁前半部分的外側和稍上。它的後方與枕骨頸靜脈突接壤,前方和上方與顳骨岩部頸靜脈窩接壤(14)。孔位於岩斜縫合的後端。頸靜脈孔由岩骨和枕骨相對邊緣的頸內突分為兩部分,它們要麼直接連接,要麼由纖維帶連接。較小的前內側部分,即岩部,傳導岩下竇,較大的後外側部分,即乙狀竇,傳導乙狀竇。頸內部分沿頸內突分布,傳遞舌咽神經、迷走神經和副神經。頸內靜脈位於孔內的擴大部分稱為頸靜脈球。頸靜脈突也是頸靜脈孔後頭側直肌的附著點。

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.1。枕骨和枕骨大孔。A,劣勢視角。B,後下視圖。C,前後位。D,高級視圖。E,後上位。F,後上斜位。枕骨環繞橢圓形的枕骨大孔,其後方比前方寬。較窄的前部位於齒狀突上方,它從外側被枕骨髁侵犯。 The wider posterior part transmits the medulla. The occipital bone is divided into a squamosal part located above and behind the foramen magnum; a basal (clival) part situated in front of the foramen magnum; and paired condylar parts located lateral to the foramen magnum. The squamous part is internally concave. Its upper margin articulates with the parietal bone at the lambdoid suture, and its lower margin articulates with the mastoid portion of the temporal bone at the occipitomastoid suture. The convex external surface of the squamosal part has several prominences. The largest prominence, the external occipital protuberance (inion), is situated at the central part of the external surface. The superior nuchal line radiates laterally from the protuberance. A vertical ridge, the external occipital crest, descends from the external occipital protuberance to the midpoint of the posterior margin of the foramen magnum. The inferior nuchal lines run laterally on both sides from the midpoint of the crest. The internal surface of the squamous part is concave and has a prominence, the internal occipital protuberance, near its center. The internal surface is divided into four unequal fossae by the sulcus of the superior sagittal sinus, the internal occipital crest, and the sulci for the transverse sinuses. The internal occipital crest bifurcates above the foramen magnum to form a V-shaped ridge between the limbs of which is the vermian fossa. The basilar part of the occipital bone, which is also referred to as the clivus, is a thick quadrangular plate of bone that extends forward and upward to join the sphenoid bone just below the dorsum sellae. The superior surface of the clivus slopes upward from the foramen magnum and is concave from side to side. The clivus is separated on each side from the petrous part of the temporal bone by the petroclival fissure that ends posteriorly at the jugular foramen. The occipitomastoid suture extends posterolateral from the jugular foramen. On the inferior surface of the basilar part, a small elevation, the pharyngeal tubercle, gives attachment to the fibrous raphe of the pharynx. The condylar parts of the occipital bone, on which the occipital condyles an located, are situated lateral to the foramen magnum on the external surface. The alar tubercle, which gives attachment to the alar ligament, is situated on the medial side of each condyle. The hypoglossal canal is situated above the condyle. The condylar fossa, which may be converted into a foramen for the passage of an emissary vein, is located behind the condyle. The jugular process of the occipital bone extends laterally from the posterior half of the condyle and articulates with the jugular surface of the temporal bone. The sulcus of the sigmoid sinus crosses the superior surface of the jugular process. The jugular foramen is bordered posteriorly by the jugular process of the occipital bone and anteriorly by the jugular fossa of the petrous temporal bone. The jugular tubercle lies on the internal surface above the hypoglossal canal. A., artery; Ac., acoustic; Car., carotid; Cond., condyle; Digast., digastric; Ext., external; Fiss., fissure; For., foramen; Hypogl., hypoglossal; Inf., inferior; Jug., jugular; Occipitomast., occipitomastoid; Occip., occipital; Petrocliv., petroclival; Pharyng., pharyngeal; Proc., process; Protrub., protuberance; Sag., sagittal; Sig., sigmoid; Sup., superior; Trans., transverse.

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.2。模擬。阿特拉斯。一、視野優越;B、劣觀;C,前視圖;D,後視圖。寰椎由位於環前內側的兩個較厚的側塊組成,前部由短的前弓連接,後部由較長的彎曲後弓連接。前後結節位於前中線和後中線。上關節麵是一個橢圓形的凹麵,向上和內側與枕骨髁相連。 The inferior articular facet is a circular, flat, or slightly concave facet that faces downward, medially, and slightly backward and articulates with the superior articular facet of the axis. The medial aspect of each lateral mass has a small tubercle for the attachment of the transverse ligament of the atlas. The transverse process projects from the lateral masses. The transverse foramina transmit the vertebral arteries. The upper surface of the posterior arch adjacent to the lateral masses has paired grooves in which the vertebral arteries course. A., artery; Ant., anterior; Art., articular; For., foramen; Lat., lateral; Mass., masses; Post., posterior; Proc., process; Trans., transverse; Vert., vertebral.

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.2。情況。軸。E,前視圖;F,側麵視圖;G,上級視圖;H,劣勢視圖。軸由齒狀突(齒狀突)區分。齒突的前部是關節突,它與寰椎前弓背部的關節突形成關節。齒狀突在其後表麵的底部有凹槽,即寰椎橫韌帶通過的地方。 The oval superior articular facets articulate with the inferior facets of the atlas. The superior facets are anterior to the inferior facets. The pedicles and laminae are thicker than on the other cervical vertebra and the lamina fuse behind to form a large spinous process. The transverse foramina are directed superolaterally, thus permitting the lateral deviation of the vertebral arteries as they pass up to the more widely separated transverse foramina in the atlas. The inferior articular facets face downward and forward.
寰椎是第一頸椎,與其他頸椎不同的是,寰椎呈環狀,缺乏椎體和棘突(圖6.2)。它由兩個位於環前外側的厚側塊組成。側塊前麵由短的前弓連接,後麵由較長的彎曲的後弓連接。通常椎體的位置被軸的齒狀突所占據。前弓前凸並有前正中結節。後弓向後凸,在其上外表麵外側有正中後結節和椎動脈流經的槽。該溝可部分或完全通過從寰椎上關節麵後緣向後拱至其後弓的骨橋轉化為孔。第一頸脊神經也在溝中,它位於動脈和骨頭之間。每個側塊的上表麵有一個向上和內側的橢圓形凹麵,並與向下和外側的枕骨髁相連。每個側塊的下表麵有一個圓形、平麵或略凹的麵,朝下、向內、略向後,並與軸的上關節麵相連。 The medial aspect of each lateral mass has a small tubercle for the attachment of the transverse ligament of the atlas, which passes behind the dens. Each transverse foramen, which transmits a vertebral artery, and upon which the nerve root sits, is situated between the lateral mass and the transverse process.
軸,即第二頸椎,比寰椎更接近於典型的椎體,但由齒狀突(齒狀突)區分,齒狀突從身體向上突出(圖6.2)。齒狀突起長1.0- 1.5厘米,寬約1厘米。齒突的前部是關節突,它與寰椎前弓背部的關節突形成關節。齒狀突的頂端呈尖狀,由根尖韌帶連接;齒狀突的一側為扁平,與鼻翼韌帶相連;齒狀突的後表麵底部為凹槽,與寰椎橫韌帶相連。齒突和身體兩側有一對巨大的橢圓形切麵,從身體橫向延伸到椎弓根的毗鄰部分,並與寰椎的下切麵相連。上關節麵不與下關節麵形成關節柱,而是在後者的前麵。身體的前部在頸長肌連接區域的中線兩側被挖空。椎板比任何其他頸椎都厚,椎弓根粗壯,棘突很大。
軸的橫向突起很小。其鈍尖表現為單個結節,即前結節,位於橫突前根與機體交界處或附近。每個橫孔都朝上外側,因此當椎動脈向上延伸至寰椎中分離較廣的橫孔時,允許其發生側向偏移。下關節麵位於椎弓根和椎板的交界處,朝下向前。鏟形椎孔比較大。

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.3。模擬。枕骨大孔。後的看法。逐步剝離。A,小腦扁桃體,Magendie孔,和第四腦室的下部位於枕骨大孔上方。椎動脈在枕骨大孔下穿入硬腦膜,並通過齒狀韌帶和副神經前的枕骨大孔上升。舌咽神經、迷走神經和副神經通過頸靜脈孔,頸靜脈孔位於枕骨大孔的前半部分外側。第二,小腦被切除了。椎動脈通過枕骨大孔到達髓質前部。 C, enlarged view of the left half of the foramen magnum. The vertebral artery passes behind and below the atlanto-occipital joint, penetrates the dura, and passes in front of the dentate ligament and accessory nerve. The rostral end of the dentate ligament attaches to the dura at the level of the foramen magnum. The C1 nerve penetrates the dura with the vertebral artery. The hypoglossal nerve passes behind the vertebral artery and enters the hypoglossal canal. The hypoglossal nerve is separated into several bundles as it penetrates the dura. The posterior spinal artery arises as the vertebral artery enters the dura and gives rise to ascending and descending branches. D, a longitudinal strip of the medulla and floor of the fourth ventricle has been removed to expose the vertebrobasilar junction, the origin of the anterior spinal artery, and the median anterior medullary and median anterior spinal veins. A., artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; Asc., ascending; Atl., atlanto-; Bas., basilar; Br., branch; Bridg., bridging; CN, cranial nerve; Cruc., cruciform; Dent., dentate; Desc., descending; Flocc., flocculus; For., foramen; Horiz., horizontal; Lig., ligament; Med., median, medullary; Memb., membrane; Men., meningeal; Occip., occipital; P.I.C.A., posteroinferior cerebellar artery; Post., posterior; Sp., spinal; Trans., transverse; V., vein; Vent., ventricle; Vert., vertebral.

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.3。練習。枕骨大孔。後的看法。逐步剝離。E,右半部分髓質被切除了。脊髓前動脈主要起源於左側椎動脈,但也有少量來自右側椎動脈。兩束右側舌下細根穿透硬腦膜。F,放大視圖。髓質被切除以暴露椎體和脊髓前動脈。 The C1 nerve roots penetrate the dura with the vertebral artery. G, the intradural segment of the vertebral arteries and the dura lining the anterior margin of the foramen magnum have been removed to expose the tectorial membrane, a rostral extension of the posterior longitudinal ligament, and the vertebral venous plexus, which courses just outside the dura. H, the tectorial membrane has been removed to expose the cruciform and alar ligaments. The horizontal portion of the cruciform ligament, called the transverse ligament of the atlas, extends laterally to be attached to the medial edges of the lateral masses of the atlas, and the vertical portion ascends to attach to the anterior margin of the foramen magnum deep to the tectorial membrane. The alar ligaments pass upward and laterally and attach to the lateral edges of the foramen magnum. Anterior meningeal arteries pass along the dura and ligamentous structures in the anterior spinal canal. I, the vertical portion of the cruciform ligament has been folded downward to expose the synovial joint between the anterior surface of the cruciform ligament and the posterior surface of the dens. There is also another synovial joint between the anterior surface of the dens and the posterior surface of the anterior atlantal arch. The apical ligament of the dens extends upward to be attached to the margin of the foramen magnum.
寰椎和軸的關節包括四個滑膜關節:齒突前後的兩個正中關節,以及寰椎和軸側塊相對關節麵之間的成對外側關節(圖6.2-6.4)。每個中間關節位於齒突的前後,都有自己的纖維囊和滑膜腔。前突位於齒狀突的前表麵和寰椎前弓的後側麵之間。後側滑膜腔更大,位於軟骨覆蓋的寰椎橫韌帶前表麵和齒狀突後表麵之間。
寰椎和樞椎由十字韌帶、前後縱韌帶和圍繞在側塊上相對關節麵之間的關節囊連接。交叉韌帶有橫向和垂直的部分,在齒突後麵形成交叉。橫向部分稱為橫韌帶,是一條粗壯的帶,在齒狀突後拱過寰椎環,並將椎管分為包含硬腦膜和脊髓的較大後腔室和包含齒狀突的較小前腔室。橫韌帶在齒狀突後的中間較與寰椎側塊內側結節相連的末端更寬。當它穿過齒突時,小的縱向帶從它的後表麵向上和向下。顱骨延伸附著於斜坡的上表麵,位於齒狀突的尖韌帶和蓋膜之間。下帶附於軸體的後表麵。齒狀突的頸部在後麵被橫韌帶包圍的地方收縮。
前寰椎與寰椎軸由前縱韌帶連接,前縱韌帶是固定於寰椎前弓下緣上方、寰椎軸體前方下方的一條寬寬的韌帶。後縱韌帶下方附著於軸體的後表麵,上方附著於交叉韌帶的橫向部分和斜坡。在椎管後方,寰椎和椎軸由一層寬而薄的膜連接,黃韌帶連接在寰椎後弓的下緣和椎軸椎板的上緣。這層膜在側麵被第二頸神經刺穿。

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.4。前視圖。橫切麵的逐步解剖顯示了枕骨大孔和斜坡與鼻腔、口腔、咽和顳下窩的關係。A,軟齶,它被保存了下來,位於枕骨大孔的水平。顳下窩位於蝶大翼和顱中窩下方,包含翼肌、上頜動脈、下頜神經分支和翼靜脈叢,向後方開放,進入頸動脈鞘周圍區域,如圖左側所示。B、放大視圖。軟齶在中線分裂,葉片向側麵反射。寰枕關節和枕骨大孔大約位於硬齶的水平。C1前弓和齒狀突位於口咽部後方,斜坡位於鼻咽部和蝶竇後方。通過咽黏膜可見頭長肌上方的隆起和C1前弓。 C, the mucosa lining the posterior pharyngeal wall has been reflected to the right, exposing the longus capitis that attaches to the clivus and the part of the longus colli that attaches to the anterior arch of C1. The eustachian tube has been divided. The rectus capitis anterior extends from the transverse process of C1, posterolateral to the longus capitis, to attach to the occipital bone in front of the occipital condyle. D, the clivus and anterior arch of C1 have been removed. The dura has been opened to expose the vertebral and basilar artery. The dens has been preserved. The structures in the right infratemporal fossa and part of the right carotid artery and mandible have been removed to expose the right vertebral artery ascending between the C2 and C1 transverse processes. E, enlarged view of the step between C and D. The anterior arch of C1 has been removed to expose the odontoid process and the lower part of the clivus. The left longus coli and longus capitis have been reflected out of the exposure. The atlanto-occipital joint is exposed at the level of the odontoid apex. The transverse part of the cruciform ligament, also called the transverse ligament, extends across the back of the dens and attaches to a tubercle on the medial side of each lateral mass of the axis. The tectorial membrane, a cephalic extension of the posterior longitudinal ligament, lines the posterior clival surface. The alar ligaments attach to the lateral edges of the foramen magnum. F, enlarged view of the exposure shown in D. G, exposure after opening of the clivus. Both vertebral and anteroinferior cerebellar arteries (AICAs) and the anterior spinal artery are exposed. A., artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; Atl., atlanto-; Cap., capitis; Car., carotid; CN, cranial nerve; Eust., eustachian; For., foramen; Infratemp., infratemporal; Int., internal; Jug., jugular; Lat., lateral; Lig., ligament; Long., longus; M., muscle; Mandib., mandibular; Max., maxillary; Med., medial; Memb., membrane; Occip., occipital; Pteryg., pterygoid; Rec., rectus; Sp., spinal; Sphen., sphenoid; Trans., transverse; Vert., vertebral.
寰枕骨和枕骨由環繞寰枕關節的關節囊和寰枕前膜和後膜連接(圖6.2- 6.4)。寰枕關節的關節囊有時在內側有缺陷,其中滑膜腔可能與滑膜囊在齒狀突和寰枕橫韌帶之間相通。寰枕前膜附著於枕骨大孔前緣上方,寰枕前弓上緣下方,寰枕關節囊外側。
寰枕後膜是一層薄膜,上麵與枕骨大孔的後緣相連,下麵與寰枕後弓的上緣相連。膜的外側邊界是自由的,拱在椎動脈和頸第一神經根後麵。該膜的外側邊緣可能在其拱起椎動脈後側的區域發生骨化,從而在寰枕關節內側的動脈周圍形成部分或完整的骨環。
蓋膜、成對的鼻翼韌帶和根尖韌帶這四條纖維帶連接軸和枕骨(圖6.3和6.4)。蓋膜是後縱韌帶的頭側延伸,覆蓋齒狀突和交叉韌帶。它連著軸體的後表麵,連著枕骨上表麵枕骨大孔前,連著寰枕關節內側外側。鼻翼韌帶是兩條強壯的韌帶,出現在齒狀突上部的兩側,並斜向上外側延伸,附著於枕髁的內側表麵。齒狀突尖韌帶從齒狀突尖部延伸至枕骨大孔前緣,位於寰枕前膜和十字韌帶上延長段之間。

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.5。枕骨下的肌肉。逐步剝離。A,右側斜方肌和胸鎖乳突肌被保留。左側斜方肌和胸鎖乳突肌與盔瓣腱膜一起被反射,暴露下方的半棘肌、頭脾肌和肩胛提肌。B,右側胸鎖乳突肌和斜方肌已反射露出頭脾。切除左側頭脾,露出下方的半棘肌和頭最長肌。C,切除右側頭脾,露出半棘肌和頭最長肌。切除左側半棘肌和頭最長肌,露出由上斜肌(從C1橫突到枕骨)、下斜肌(從C1橫突延伸到C2棘突)和頭後直肌(從枕骨下頸線下延伸到C2棘突)形成的枕下三角。椎動脈在枕下三角的深處穿過C1上關節麵後並穿過後大西洋弓的上邊緣。 D, both semispinalis capitis muscles have been reflected laterally to expose the suboccipital triangles bilaterally. E, the muscles forming the left suboccipital triangle have been removed. The vertebral artery ascends slightly lateral from the transverse process of C2 to reach the transverse process of C1 and turns medially behind the superior facet of C1 to reach the upper surface of the posterior arch of C1. The C2 ganglion is located between the posterior arch of C1 and the lamina of C2. The dorsal ramus of C2 produces a medial branch that forms the majority of the greater occipital nerve. F, the muscles forming both suboccipital triangles have been removed. The rectus capitis posterior minor, which extends from the posterior arch of C1 to the occipital bone below the inferior nuchal line, has been preserved. The vertebral arteries cross the posterior arch of the atlas and penetrate the posterior atlanto-occipital membrane to reach the dura. A., artery; Atl., atlanto-; Cap., capitis; Car., carotid; CN, cranial nerve; Inf., inferior; Int., internal; Jug., jugular; Lev., levator; Longiss., longissimus; M., muscle; Maj., major; Memb., membrane; Min., minor; Obl., oblique; Occip., occipital; Post., posterior; Proc., process; Rec., rectus; Scap., scapulae; Semispin., semispinalis; Spin., spinalis; Splen., splenius; Sternocleidomast., sternocleidomastoid; Sup., superior; Trans., transverse; V., vein; Vert., vertebral.
枕骨大孔的周圍是肌肉附著在枕骨和上頸椎(無花果。6.4和6.5)。斜方肌覆蓋頭部和頸部的後部。它從頸上線的內側延伸,枕骨外隆突,頸椎和胸椎的棘突,並在肩膀上彙合,與肩胛骨和鎖骨外側的三分之一相連。胸鎖乳突肌斜向下穿過頸部從上頸線和乳突的外側延伸到胸骨上部和鎖骨的鄰近部分。這塊肌肉將頸部分成前三角和後三角。前三角的邊界是胸鎖乳突肌的前邊界,上麵是下頜骨,前麵是頸部的中間線;後三角的邊界前麵是胸鎖乳突肌的後緣,下麵是鎖骨的中間三分之一,後麵是斜方肌的前緣。頭脾位於斜方肌和胸鎖乳突肌深部並部分被其覆蓋,從上頸線外側三分之一以下的骨延伸至下頸椎和上胸椎的棘突。頭半棘肌位於頭脾肌和胸鎖乳突肌的深處,並附著於上胸椎和下頸椎,頭半棘肌附著於上頸線和下頸線之間的區域,從枕外脊內側開始,向外側延伸到枕乳突連接處,頭最長肌附著於乳突後緣。
枕下肌位於下一層,是位於枕下區的脾肌、半棘肌和頭最長肌深部的一組肌肉。這組包括上斜肌,它從頸上和頸下線之間的頭半棘肌外側延伸到寰椎橫突;下斜肌,從棘突和椎板延伸到寰椎橫突;頭後直肌,它從頸下線的外側延伸到軸脊;頭小後直肌,位於頭大後直肌的內側,部分被頭大後直肌覆蓋,從內側延伸到頸下線以下直到寰椎後弓上的結節。
枕下三角是一個由頭後大直肌上方和內側、上斜肌上方和外側、下斜肌下方和外側構成的區域(圖6.5)。它在內側被頭半棘肌覆蓋,在外側被頭脾覆蓋。三角底由寰枕後膜和寰枕後弓構成。三角形的結構是椎動脈硬膜外末端和第一頸神經。
頸闊肌是從麵部下方向下延伸穿過鎖骨到達覆蓋胸大肌和三角肌的筋膜。前椎肌插入枕骨的斜坡部分,在枕骨枕骨大孔前。這一組包括頸長肌,它附著在寰椎和第三胸椎之間的脊柱前表麵;頭長肌,從枕骨大孔前斜坡延伸到第三至第六頸椎橫突;頭前直肌,位於頭長肌上部的後麵,從枕髁前的枕骨延伸到寰椎側塊和橫突的前表麵;還有頭側直肌,它從枕骨頸突延伸到寰椎橫突。
上述肌肉嵌在頸筋膜內。這個筋膜分為淺層和深層。淺層為真皮下方的疏鬆結締組織層,覆蓋頸闊肌。深層位於頸闊肌內部,包裹著肌肉,並凝結成纖維鞘,將動脈和伴隨的靜脈連接在一起。深筋膜淺板在後中線與頸韌帶相連,薄包斜方肌,繼續向前覆蓋頸後三角,在胸鎖乳突肌後緣分包肌肉,在其前緣再次形成覆蓋頸前三角並到達中平麵的板,與對麵相應的板連續。頸動脈鞘是頸筋膜的凝結物,它覆蓋頸總動脈和頸內動脈、頸內靜脈和迷走神經。頸筋膜椎前板覆蓋椎前肌,向外側延伸與頸動脈鞘連接,覆蓋斜角肌,形成頸部後三角的筋膜底。再往上連著顱底,再往下延伸到咽部後麵在頸長肌前麵進入上縱隔。深筋膜上方與頸上線、乳突、顴弓、莖突和下頜骨融合,下方與肩胛骨、鎖骨和胸骨融合。
位於枕骨大孔區域的神經結構包括腦幹的尾端部分、小腦和第四腦室、脊髓的吻側部分以及顱下神經和頸上神經(圖6.3和6.6)(5,19)。
脊髓在任意設定的位於形成第一頸神經的背側和腹側細根的上限的水平上難以區分地混入髓質(圖6.3和6.6)。在腹側比背側更容易鑒別,因為第一頸神經的腹側小根總是存在,而在許多情況下背側小根不存在。脊髓和髓質的交界處位於第一頸根的吻側邊緣,這意味著占據枕骨大孔的是髓質,而不是脊髓。
位於枕骨大孔下方的脊髓呈圓形,由一個裂隙和幾個溝分割。前正中裂和後正中溝將脊髓分成對稱的兩半。前正中裂隙達到幾毫米的深度。後中溝較淺,後中隔從這裏穿過脊髓,幾乎到達中央管。後外側溝位於脊髓背根進入脊髓的那條線上。後微索位於後中溝和後外側溝之間。在上頸椎水平,每個後微索的表麵被另一個淺的縱向溝分隔,即後中間溝,在內側分為股薄束,在外側分為楔形束。脊髓後外側溝與前正中裂之間的區域,由脊神經的出側細根分為前脊髓索和外脊髓索。前索囊包括腹側根的出現區。側索位於腹根和後外側溝之間。 In the upper cervical region, the rootlets that unite to form the spinal part of the accessory nerve emerge through the lateral funiculus.

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.6。枕骨大孔。A-D,後視圖;E和F,前視圖。A,枕下顱骨切除術和上頸椎椎板切除術暴露硬腦膜。椎動脈從內側穿過寰椎的上表麵,在那裏它們發出腦膜後動脈,這些動脈向上在枕骨大孔和後窩的後部供給硬腦膜。插入,右上角。寰椎弓左半邊的上緣在椎動脈進入硬腦膜的近端形成一個骨環。B,打開硬腦膜後另一個枕骨大孔的放大視圖。右側異食癖發生於硬腦膜外,並通過椎動脈穿透硬腦膜。 The rostral end of the dentate ligament passes between the vertebral artery and the PICA to insert into the dura along the lateral margin of the foramen magnum. The accessory nerve ascends posterior to both the PICA and the vertebral artery. The vertebral artery gives rise to a posterior spinal artery that passes along the posterolateral aspect of the spinal cord and medulla. The hypoglossal rootlets are stretched over the posterior aspect of the vertebral artery. C, the right tonsil has been retracted to expose the caudal end of the fourth ventricle, which is located above the foramen magnum. The right PICA ascends through the foramen magnum and along the posterior margin of the medulla to reach the cerebellomedullary fissure. D, another specimen. The rostral end of the dentate ligament passes between the posterior spinal artery and vertebral artery and attaches to the dura at the level of the foramen magnum. The accessory nerve ascends behind the posterior spinal artery. The C1 nerve root receives a contribution from the accessory nerve and passes through the dura with the vertebral artery and courses along the lower margin of the artery. The posterior spinal artery arises inside the dura and passes between the dentate ligament and accessory nerve and gives rise to ascending branches to the medulla and descending branches to the spinal cord. E, the anterior skull base has been removed. The vertebral arteries ascend in front of the brainstem and give rise to the anterior spinal artery. F, enlarged view. The C1 ventral roots penetrate the dura with the vertebral artery. The hypoglossal rootlets pass behind the vertebral arteries. A., artery; Bas., basilar; Cer.Med., cerebellomedullary; CN, cranial nerve; Cond., condyle; Dent., dentate; Fiss., fissure; Hypogl., hypoglossal; Lig., ligament; Men., meningeal; Occip., occipital; P.I.C.A., posteroinferior cerebellar artery; Post., posterior; Sp., spinal; Vert., vertebral.
齒狀韌帶被認為與脊髓相連,因為它與脊髓相連(圖6.3和6.6)。這個韌帶是一種白色纖維片,連接在脊髓內側和硬腦膜外側。齒狀韌帶的內側沿脊髓兩側的背側和腹側細根之間與脊膜相連,每側有一係列三角形的齒狀突起,這些齒狀突起間隔地與硬腦膜相連。在顱頸交界處,齒狀韌帶位於椎動脈與C1前腹根和脊髓後動脈和脊髓副神經後支之間;此外,它經常在硬腦膜穿入處並入椎動脈周圍的硬腦膜袖內。齒狀韌帶的最側附著位於枕骨大孔的水平,在椎動脈穿硬腦膜的上方。盡管齒狀韌帶位於副神經的前麵,但在這個水平上,韌帶位於副神經的後麵。第二個三角形突連接硬腦膜在椎動脈和C1根穿過硬腦膜的位置下麵。切開上兩個三角突可以增加脊髓前麵的通路。第一頸神經穿過硬腦膜時沿著椎動脈的後下表麵走。 The ventral root is located anterior to the dentate ligament, and the dorsal root, which is infrequently present, passes posterior to the dentate ligament. There are frequently communications between the C1 nerve root and the spinal accessory nerve.
下髓質在C1神經根水平與上脊髓難以區分(圖6.3、6.4和6.6)。髓質的前表麵由髓質金字塔組成,它們麵向斜坡、枕骨大孔的前緣和齒狀突的嘴側部分。側麵主要由下橄欖形成。髓質的後表麵分為上下兩部分。上部由第四腦室下半部分的中線組成,外側由小腦下梗組成。後表麵下部內側為纖細束和結節,外側為楔形束和結節。
枕下小腦麵位於枕骨大孔的後外側邊緣之上。隻有由扁桃體和雙側小葉形成的半球的下部,以及由結節、小舌和錐體形成的蚓部的下部與枕骨大孔有關。雙側小葉位於枕骨大孔外側上方,扁桃體位於後緣水平上方(圖6.3和6.6)。在枕骨大孔後部上方的小腦表麵有一個很深的垂直凹陷,即小腦後切口,它包含小腦鐮並向下延伸至枕骨大孔。扁桃體位於枕骨大孔後緣上方,常發生枕骨大孔疝。每個扁桃體都是卵形結構,沿其上外側邊界與小腦的其餘部分相連。小腦延髓裂在小腦和髓質之間向上延伸,位於枕骨大孔後緣的吻側。
副神經是唯一穿過枕骨大孔的腦神經(圖6.3和6.6)。它有一個由從延髓中產生並與迷走神經相連的細根組成的顱部,還有一個由從延髓下部和脊髓上部產生的一係列細根結合而成的脊髓部。在後窩,副神經由一條來自脊髓的主幹和3 - 6條來自髓質的小細根組成。大多數吻側髓質細根是迷走神經下細根,因為它們起源於迷走神經核(25)。下髓根與神經的脊髓部分相連。上髓根進入頸靜脈孔而不與脊髓部分相連,但一旦進入頸靜脈孔,它們就與迷走神經或副神經相連。脊髓的貢獻來自於脊髓的頸部分,是位於腹側和背側之間的一係列細根。在50條檢查的神經中,2條附屬神經的根狀小根的最低起點位於C7根,10條為C6, 13條為C5, 11條為C4, 7條為C3, 5條為C2, 2條為Cl(5)。這些細根結合形成直徑約1.0 mm的主幹,通過齒狀韌帶和脊髓背根之間的枕骨大孔上升,進入椎動脈後方的顱後窩。
在我們之前的研究中檢查的50個副神經中,所有的副神經都與上頸神經的背根相連。最常見和最大的吻合是與第一頸神經背根的吻合(5,22)。28個C1背根隻來自副神經沒有來自脊髓的C1水平。所有的15個Cl背根在C1水平接受了來自脊髓的細根,也有來自副神經的吻合纖維。50條副神經中4條與C2神經根吻合,10條與C3神經根吻合,8條與C4神經根吻合,2條與C5神經根吻合。
下四根顱神經距離枕骨大孔足夠近,可能會出現病變(圖6.3和6.6)。它們的硬膜內解剖在本問題關於橋小腦角和後窩顱神經的章節中進行了描述。
每個背側根和腹側根由一係列6 - 8個小根組成,分別扇形進入脊髓的後外側和前外側表麵(圖6.3和6.6)。背根和腹根分別穿過蛛網膜下腔和硬腦膜的橫切麵,然後在椎間孔附近彙合形成脊神經。枕骨大孔區域的細根幾乎直接橫向穿過到達硬腦膜孔。背根的神經元聚集形成神經節,位於椎間孔中背根和腹根聯合的近端,但第一頸背根和相關的神經節可能缺失。C1, C2和C3神經,遠端神經節,分為背支和腹支。背支分為內側支和外側支,支配頸部後部的皮膚和肌肉。C1神經,稱為枕下神經,位於枕骨和寰椎之間的椎管,有一個比腹側支大的背側支。背支在寰椎後弓和椎動脈之間走行,到達枕下三角,在那裏它向頭直肌後大、小、上、下斜肌和頭半棘肌發出分支,偶爾也有皮膚分支伴隨枕動脈到達頭皮。C1腹側支在寰椎後弓和椎動脈之間向前延伸,在寰椎側塊外側和椎動脈內側,支配頭側直肌。C2神經位於寰椎後弓和軸板之間,脊節位於硬膜外,C1下關節突內側和椎動脈。 Distal to the ganglion, the nerve divides into a larger dorsal and a smaller ventral ramus. After passing below and supplying the inferior oblique muscle, the dorsal ramus divides into a large medial and a small lateral branch. It is the medial branch that is most intimately related to this suboccipital operative field and that forms the greater occipital nerve. It ascends obliquely between the inferior oblique and the semisplenius capitis, pierces the latter and the trapezius muscle near their attachments to the occipital bone, and is joined by a filament from the medial branch of C3. It supplies the semispinalis capitis muscle, ascends with the occipital artery, and supplies the scalp as far forward as the vertex, and occasionally the back of the ear. The lateral branch sends filaments that innervate the splenius, longissimus, and semisplenius capitis, and is often joined by the corresponding branch from the C3 nerve. The C2 ventral ramus courses between the vertebral arches and transverse processes of the atlas and axis and behind the vertebral artery to leave this operative field. Two branches of the C2 and C3 ventral rami, the lesser occipital and greater auricular nerves, curve around the posterior border and ascend on the sternocleidomastoid muscle to supply the skin behind the ear.
第一頸神經位於枕骨大孔下方,值得特別注意(圖6.3和6.6)。它與其他頸神經的不同之處在於形成神經的背側細根的一致性和起源。C1腹根由4到8個橫向連接和延伸的小根組成。在進入硬膜孔之前,C1腹側根和相應的背側根(如果存在)附著於椎動脈硬膜內起始部分的後下表麵,並通過椎動脈周圍的漏鬥狀硬膜孔出硬膜囊。腹側根與背側根在硬腦膜孔內外相連。
第一頸神經的背根比腹根複雜因為它的組成和與副神經的連接不同。在檢查的25個頸脊髓中,人們預計會發現50個C1背根起源於後外側溝,但隻有15個被發現(5)。副神經在35個根中有28個根與C1神經有根,其中28個根缺乏來自脊髓的背根。其餘7例C1背根缺失。每15根起源於脊髓的背根也都有副神經的作用。
與枕骨大孔相關的主要動脈是椎動脈和小腦後下動脈(PICA),椎動脈的腦膜分支,頸外動脈和頸內動脈(圖6.3、6.4和6.6)(16,20,21)。
成對的椎動脈起於鎖骨下動脈,經上六個頸椎橫突上升,經過軸側塊後方,進入枕髁後方硬腦膜,經枕骨大孔上升至髓質前部,在橋髓交界處彙合形成基底動脈。每條動脈分為硬膜內和硬膜外部分(圖6.3-6.6)。
硬膜外部分分為三段。第一個節段從鎖骨下動脈起點延伸至最低橫孔的入口,通常在C6水平。第二節通過頸神經根前的上六個頸椎的橫孔上升。該節段在軸上方橫向偏離,到達寰椎橫孔的橫向位置。第三節是與枕骨大孔最密切相關的部分,從寰椎橫突的枕骨大孔延伸至硬腦膜的通路部位。動脈穿過寰椎橫突後,位於頭直肌外側內側。第三節穿過寰椎側塊和寰枕關節後的內側,並壓入寰椎後弓外側部上表麵的凹槽,在那裏沿枕下三角的底部行進。它通過寰枕膜外側邊界前進入椎管。它部分被寰枕後膜和半棘肌,頭直肌後大肌,上斜肌和下斜肌覆蓋。它被頸深靜脈和硬膜外靜脈的吻合組成的靜脈叢包圍。 The C1 nerve root passes through the dura mater on the lower surface of the vertebral artery between the artery and the groove on the posterior arch of the atlas with the vertebral artery. This bony groove is frequently transformed into a bony canal that completely surrounds a short segment of the artery. Of the 50 arteries we examined, 24 (48%) were in a shallow groove, 12 (24%) were partially, but incompletely, surrounded by bone, and 14 (28%) coursed through a bony ring that completely surrounded the artery (Fig. 6.6) (5). The terminal extradural segment of the vertebral artery gives rise to the posterior meningeal and posterior spinal arteries, branches to the deep cervical musculature, and infrequently the PICA.
硬膜內段開始於硬腦膜孔位於枕骨大孔側邊下方。這個區域的硬腦膜比其他區域要厚得多,它在動脈周圍形成一個漏鬥狀的孔,長度為4- 6mm。第一頸神經從椎管出來,脊髓後動脈通過硬腦膜孔和椎動脈進入椎管。這三種結構通過硬膜纖維帶在小孔處結合在一起。椎動脈的硬膜內段在第一頸神經的背根和腹根上方,在脊髓後動脈,齒狀韌帶,和副神經的脊髓部分的前麵。
一旦進入硬腦膜,動脈從下外側上升到髓質的上前表麵。動脈硬膜內部分分為外側和前髓段(5,16)。外側髓段起於硬腦膜孔,沿外側髓麵前上延伸至橄欖前溝。前髓段起於橄欖前溝,在舌下細根的前麵或中間穿過金字塔,在橋髓溝處或附近與另一椎動脈彙合形成基底動脈。在其上升過程中,外側髓段的前表麵和外側表麵麵對枕骨髁、舌下管和頸靜脈結節。前髓段位於斜坡上。椎動脈在枕骨大孔區域的分支為脊髓後動脈、脊髓前動脈、異食癖動脈、腦膜前動脈和腦膜後動脈。
配對的脊髓後動脈通常起源於椎動脈的後內側表麵,就在硬腦膜外,但它們也可能起源於椎動脈的硬膜內初始部分,或起源於異食症(圖6.3和6.6)(5,16,21)。在硬腦膜切開時應注意保護脊髓後動脈,因為它可能與椎動脈周圍的硬腦膜袖帶合並。當每條脊髓後動脈穿過硬腦膜時,它被與椎動脈和第一頸神經根相同的纖維隧道所包圍。在蛛網膜下腔內,它在齒狀韌帶的最口部附件後的內側走行,到達下延髓時,分為升支和降支。上升分支穿過枕骨大孔,支配枕狀體、纖細結節和楔形結節、副神經的細根和麥根蒂孔附近的脈絡膜叢,並可產生與異食癖分支吻合的分支。降支在脊髓後外側的背側小根和齒狀韌帶之間向下延伸,支配頸脊髓背側半部分的淺表部分。它與進入椎孔的神經根動脈的後支吻合。下行分支產生側支,每一個較低的分支比上一個更小,更不穩定,它們穿過脊髓後表麵的內側,並在中線形成平行於脊髓後動脈的動脈。
異食動脈是椎動脈最大的分支(圖6.3和6.6)。它通常起源於硬腦膜,但也可能很少起源於椎動脈的硬膜外末端。它可能出現在枕骨大孔上或下;在50個小腦中發現的42條動脈中,35條位於小孔上方,7條位於小孔下方(16)。扁桃體髓內異食癖段,形成尾袢與扁桃體下部相關,與枕骨大孔關係最密切。42條動脈中有37條尾袢下端位於枕骨大孔邊緣之上,4條位於枕骨大孔邊緣之下,1條位於枕骨大孔邊緣水平。
脊髓前動脈由成對的脊髓前腹側動脈結合形成,起源於椎動脈基底動脈起點附近的前髓質段(圖6.3、6.4和6.6)。在我們84%的標本中,脊髓前腹動脈的連接點位於橄欖下端枕骨大孔上方(5)。在某些病例中,脊髓前腹動脈中的一條繼續向下延伸作為脊髓前動脈,另一條終止於髓質前表麵或連接較小的脊髓前腹動脈與主導動脈的初級通道。
脊髓前動脈通過髓質前表麵的枕骨大孔和脊髓在前正中裂內或附近下行。在髓質上,它支配金字塔及其交叉、內側小丘、橄欖間束、舌下核和神經,以及後縱束(17)。它與進入頸椎孔的神經根動脈的前支吻合。下行通道較大時與神經根前支吻合較少,較小時與神經根前動脈連接頻繁。
枕骨大孔周圍的硬腦膜由椎動脈的前、後腦膜分支以及咽升動脈和枕動脈的腦膜分支供應(圖6.3和圖6.6)(5,20)。這些動脈,加上腦膜垂體幹的脊膜背側分支起源於頸內動脈海綿內段,支配著顱後窩的硬腦膜。異食癖、脊髓後動脈和椎動脈硬膜內部分罕見地產生腦膜分支。
椎動脈的腦膜前分支起源於椎動脈硬膜外部分的內側表麵,緊接於第三頸椎橫孔上方(圖6.3)。該動脈通過第二和第三頸椎之間的椎間孔進入椎管,並在後縱韌帶和硬腦膜之間上升。在齒尖的水平上,每根動脈都向內側移動,從另一側與它的配偶連接,並在齒尖上形成一個拱形。它的分支支配斜坡區域的硬腦膜、枕骨大孔前部和椎管上部,它們與咽升動脈和脊膜背側動脈的分支吻合,後者支配覆蓋後窩前部和前外側的硬腦膜。腦膜前動脈還產生肌肉和骨性分支,它們支配身體和軸的齒狀突以及寰枕關節和寰樞關節的關節板。
脊膜後動脈起於椎動脈的後上表麵,環繞寰椎側塊,在後弓上方或在穿透硬腦膜之前;然而,它可能起源於硬膜內,在這種情況下,它穿過蛛網膜到達硬腦膜(圖6.6)(5)。它沿著曲折的上升路徑穿過硬腦膜,到達大孔後緣。經過枕骨大孔後,上升至小腦鐮附近,並在小腦鐮附近分為幾支,最後終止於幕和腦鐮的後部。它供應後顱窩後外側和後部的硬腦膜,並與咽升動脈和枕動脈的腦膜分支吻合。
頸外動脈的咽升支通常有兩個分支在枕骨大孔上方的硬腦膜。一個分支通過舌下管,另一個通過頸靜脈孔進入(14)。穿過舌下管的分支分為向上穿過硬腦膜覆蓋斜坡並與腦膜背側動脈分支吻合的上升分支和向下分支,向下走向枕骨大孔前緣並與由腦膜前動脈形成的齒狀突上方拱廊的分支吻合。這個吻合網在硬腦膜上,在枕骨大孔前,在斜坡上,為枕骨斜坡提供骨分支。經頸靜脈孔進入的分支分為後方和後上方的分支,與枕部和腦膜後動脈的腦膜分支吻合,並供應後顱窩後部和後外側的硬腦膜。
枕動脈腦膜分支是不穩定的,如果存在,它通過乳突使者孔穿透顱骨。它分為兩個分支,一個分支向後上方延伸,與腦膜後動脈的分支相連後者在後窩後部供給硬腦膜,另一個分支向前外側延伸,與咽升動脈的腦膜分支相連。
枕骨大孔區域的靜脈結構分為三組:一組由硬膜外靜脈組成,另一組由硬膜內(神經)靜脈組成,第三組由硬膜靜脈竇組成(13,18)。三組通過橋靜脈和使者靜脈進行吻合。
該區域的靜脈流動分為兩個係統:一個由頸內靜脈引流,另一個流入椎靜脈叢。頸內靜脈及其支流形成了顱頸區最重要的引流係統。頸內靜脈起源於頸靜脈孔,由乙狀竇和岩下竇彙合(14,18,25)。環繞枕下三角椎動脈的靜脈叢是由許多小通道形成的,這些小通道進入椎叢內部(硬腦膜和椎骨之間),從椎弓骨後弓上方的椎管發出。該椎靜脈叢及多條來自深部肌肉的小靜脈與密集靜脈叢相通,在寰椎橫突伴隨椎動脈進入椎間孔,經連續頸椎橫孔下行至頭臂靜脈。後髁使者靜脈穿過後髁管,在椎靜脈叢和乙狀結腸竇之間形成溝通。舌下管靜脈叢沿舌下管穿過,將基底靜脈叢與邊緣竇連接起來,後者環繞枕骨大孔。靜脈叢的一部分閉塞暴露了椎動脈的硬膜外上段。
硬腦膜中環繞枕骨孔的靜脈通道有邊緣靜脈叢、枕骨靜脈叢、乙狀竇靜脈叢、岩下靜脈叢和基底靜脈叢。邊緣竇位於枕骨大孔邊緣硬腦膜層之間。它通過一係列的小竇,與斜坡上的基底竇相連,與枕竇相連。它通常與乙狀竇或頸靜脈球相連,通過一個穿過顱內表麵的竇,並與舌下管的靜脈相通。這些吻合為頸內靜脈阻塞的情況下靜脈引流提供了另一種途徑。枕竇位於小腦鐮。它的下端分為成對的分支,每一分支都在枕骨大孔的前方與乙狀狀竇或頸靜脈球相連,其上端與torcula相連。
基底靜脈叢位於上斜坡硬腦膜層之間。它由兩側吻合岩下竇、上方吻合海綿竇、下方吻合邊緣竇和硬膜外靜脈叢的靜脈通道相互連接而成。岩下竇沿岩斜坡裂隙延伸,上與基底竇相通,下與頸靜脈球相通。乙狀竇沿乙狀竇溝下行,經頸靜脈孔乙狀竇部出顱,前外側下行至枕骨髁,前至寰椎橫突。
枕骨大孔區域的硬膜內靜脈引流小腦和腦幹下部、脊髓上部和小腦髓裂。髓質靜脈與脊髓形成縱向叢狀通道,在枕骨大孔處吻合。脊髓中位前靜脈在脊髓前中縫深處至脊髓前動脈,與脊髓中位前靜脈在髓質前中溝上連續。脊髓外側前靜脈沿腹側根的起點縱行,並在上方與脊髓外側前靜脈彙合,後者沿舌下根的起點縱行於前外側髓(橄欖前)溝。脊髓後外側靜脈,沿著脊髓後外側溝的背側根起始線,與沿橄欖後溝的外側髓靜脈在上方連續。脊膜後正中靜脈沿脊膜後正中溝走行,脊膜後正中靜脈與脊膜後表麵的主靜脈在上方連續,脊膜後正中靜脈沿脊膜後正中溝走行。橫向髓靜脈和橫向脊髓靜脈在不同的水平穿過髓質和脊髓,相互連接主要的縱向通道。橋靜脈可將神經靜脈與枕骨大孔區域的硬腦膜竇連接起來。
小腦組織疝入枕骨大孔可引起神經壓迫,甚至死亡。這些疝通常被稱為扁桃體疝(8,27),但疝通常累及扁桃體和雙側小葉,兩者都在枕骨大孔邊緣處形成深深的溝槽。疝可壓迫髓質,嚴重時疝組織發生壞死。枕骨大孔疝患者可能無症狀;或可表現為疼痛、神經受壓、顱內壓增高和突然意外死亡。由小腦、腦幹、下顱神經和上脊神經功能障礙引起的症狀包括頸部和上臂疼痛、頭暈、共濟失調、步態障礙、複視、吞咽困難、耳鳴、聽力下降、眼球震顫、虛弱到四肢癱瘓的程度以及四肢感覺障礙。咳嗽或打噴嚏可加重症狀,引起暈厥。一些沒有症狀的突然死亡的患者在屍檢時發現有通過枕骨大孔的疝。這些患者的猝死意味著枕骨大孔疝是一種不穩定的情況,輕微的壓力可能會加重(8)。這些猝死病例的共同點是扁桃體和雙側小葉鄰近部分進入枕骨大孔。疝可能是雙側對稱的,但更常見的是不完全對稱的,可能是單側的。 The herniated tonsils are tightly pressed against the medulla. Acute or chronic herniations may be seen with space-occupying lesions, such as cerebellar astrocytomas or cystic tumors. Chronic herniation is seen with the Arnold-Chiari malformation.
圖6.7。枕骨大孔手術入路。硬膜內病變通常選擇後路手術入路。位於枕骨大孔前方的硬膜外病變通常選擇前路。對於位於腦幹外側和/或前方的硬膜內病變,特別是涉及顳骨或與顳骨相鄰時,可選擇外側入路。通過顳骨的外側入路將在本問題的後麵部分進行考慮。
起源於枕骨大孔區域的腫瘤被Cushing和Eisenhardt(4)分為顱脊髓組和脊柱組,前者起於枕骨大孔上方,向下生長,後者起於枕骨大孔下方,向上生長。該區域的硬膜內髓外腫瘤通常是良性的,以腦膜瘤和神經鞘瘤最為常見。髓內腫瘤主要表現為星形細胞瘤和室管膜瘤。小腦腫瘤,特別是發源於第四腦室和小腦半球下部或蚓部的腫瘤,可延伸至或通過枕骨大孔進入上椎管。摘要脊索瘤和轉移是最常見的硬膜外腫瘤。脊索瘤通常發生在斜坡水平,並可向尾側延伸至枕骨大孔。
枕骨大孔腫瘤經常逃避早期診斷,因為它們引起類似頸椎病、多發性硬化症或退行性疾病的奇怪症狀(1,23,30)。在其他疾病中常見的症狀或體征也應提示枕骨大孔區域存在腫瘤,包括頸部僵硬和疼痛,累及下顱神經,特別是脊髓副神經,單側上肢無力和萎縮,手不協調,步態障礙,肢體模糊感覺障礙或感覺異常,非解剖模式的客觀感覺喪失,上肢不協調,錐體束表現為痙攣步態。發生於第四腦室或小腦尾部的腫瘤,可因阻塞第四腦室水平的腦脊液引流而引起顱內壓升高。

圖6.8。枕骨下的方法。根據病變部位的不同,可以采用垂直中線切口或曲棍球棒切口。A,患者最常見的是三分之四俯臥位。B,垂直中線切口用於位於椎管上部和位於枕骨大孔上方區域後方或後外側的病變。皮下組織從接近齒輪的下筋膜分離,以獲得空間,在肌肉上形成Y形切口。“Y”的上肢開始於上頸線的水平,並在齒輪以下連接。C,切口有足夠的長度來完成枕下顱骨切除術和椎板軸和寰椎切除術(斜線)。D,勾勒出硬膜切口(間斷線)。E,硬膜內暴露。 The major extracranial hazard is injury to the vertebral artery as it courses below the atlantoaxial joint and across the posterior arch of the atlas. The vertebral arteries and PICAs are in the lower part of the exposure. The accessory nerve ascends posterior to the dentate ligament. The glossopharyngeal, vagus, and accessory nerves pass toward the jugular foramen. F, upper left. Hockey-stick retrosigmoid exposure. Skin incision (solid line) and bone removal (oblique lines). Lower right. Intradural exposure. The hockey-stick incision extends superomedial from the mastoid process along the superior nuchal line to the inion and downward in the midline. This incision is selected if the lesion extends anterolateral or anterior to the brainstem toward the jugular foramen or cerebellopontine angle. This exposure permits the removal of the full posterior rim of the foramen magnum, the posterior elements of the atlas and axis, and, in addition, the ability to complete a unilateral suboccipital craniectomy of sufficient size to expose the anterolateral surface of the brainstem and the nerves in the cerebellopontine angle. Tumors in this area may extend upward through the cerebellomedullary fissure to be attached to the roof or floor of the fourth ventricle. Laterally situated tumors may be attached to the initial intradural segment of the vertebral artery and the thick dural cuff around the artery, which also incorporates the posterior spinal arteries and the C1 nerve root in fibrous tissue. As one moves superiorly along the lateral surface of the medulla, the origin of the PICA and the glossopharyngeal, vagus, accessory, facial, vestibulocochlear, and trigeminal nerves are encountered. The dura is closed with a dural substitute if closure of the patient’s dura constricts the cerebellar tonsils or the cervicomedullary junction. A., artery; A.I.C.A., anteroinferior cerebellar artery; Lig., ligament; P.I.C.A., posteroinferior cerebellar artery; Vert., vertebral.

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.9。經鼻腔進入上斜坡。A,麵部結構的截麵橫跨鼻腔,上鼻甲和中鼻甲,上頜竇,靠近鼻尖的眼眶,以及蝶竇前的篩竇。顴神經和眶下神經起源於翼齶窩的下頜骨神經,位於上頜竇後壁後。B,去除鼻甲和篩竇後氣細胞,露出犁骨和蝶竇的正麵。鼻淚管沿鼻腔側壁向下,在下鼻甲下方開口,進入下鼻道。C,切除蝶竇前麵以暴露多分隔蝶竇和蝶鞍前壁。視神經管上方的骨突起位於蝶竇的上外側邊緣。D,蝶鞍前壁和蝶竇外壁已經被切除以暴露頸動脈岩穴和腦下垂體。形成上斜坡前表麵的蝶竇後壁被保留了下來。 A., artery; Car., carotid; Cav., cavernous; CN, cranial nerve; Gang., ganglion; Gl., gland; Inf., inferior; Infraorb., infraorbital; M., muscle; Max., maxillary; M.C.A., middle cerebral artery; Med., medial; Mid., middle; N., nerve; Nasolac., nasolacrimal; Pet., petrous; Rec., rectus; Sphen., sphenoid; Sup., superior; Turb., turbinates.
枕骨大孔最常從後方或前方入路,較少從外側入路(圖6.7)。硬膜內病變常選擇後路手術入路,枕骨大孔前硬膜外病變常選擇前路手術入路。對於位於腦幹外側或腦幹前方的病變,可選擇外側入路,特別是當病變累及或鄰近顳骨和斜坡時。通過顳骨的外側入路將在顳骨章節中進行回顧。

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.10。通往斜坡的鼻道。逐步解剖顯示形成經鼻至斜坡的側限的結構。A,整個斜坡位於硬齶之上,在大多數情況下,可以通過鼻腔和鼻咽進入。鼻鼻甲、鼻肉和咽鼓管在暴露的外側邊緣。B,切除部分上、中、下鼻甲,打開蝶翼突與上頜骨後壁之間的區域,暴露出鼻腔外側壁的翼齶窩。上頜竇和額竇的開口進入位於中鼻甲下方的中鼻道。鼻淚管位於下鼻甲下方,進入下鼻道。咽鼓管位於枕骨大孔前和斜坡下緣,在翼突後緣進入鼻咽。進入斜坡加上寰椎和軸需要一個可以在上顎上下的入路。 Rosenmuller’s fossa is located behind the eustachian tube. C, the medial wall of the maxillary sinus has been opened to expose the infraorbital nerve, which arises in the pterygopalatine fossa and passes forward in the sinus roof. The maxillary nerve passes through the foramen rotundum to enter the pterygopalatine. The upper cervical carotid and eustachian tube form the lateral limit of the exposure of the lower clivus and the junction of the petrous and cavernous carotid limits the lateral exposure of the upper clivus. D, enlarged view. The bone and dura covering the optic canal in the superolateral part of the sphenoid sinus has been opened to expose the optic nerve and ophthalmic artery in the optic canal. The junction of the petrous and cavernous carotid limits the exposure below the level of the sella. The maxillary nerve exits the foramen rotundum and enters through the pterygopalatine fossa where it gives rise to the infraorbital, zygomatic, and greater palatine nerves, plus communicating rami to the pterygopalatine ganglion. Terminal branches of the maxillary artery intermingle with the neural structures in the pterygopalatine fossa. A., artery; Ant., anterior; Car., carotid; Cav., cavernous; Eust., eustachian; For., foramen; Gang., ganglion; Gr., greater; Inf., inferior; Infraorb., infraorbital; Max., maxillary; Mid., middle; N., nerve; Ophth., ophthalmic; Palat., palatine; Pet., petrosal; Proc., process; Pteryg., pterygoid; Pterygopal., pterygopalatine; Sup., superior.

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.11。鼻道通往斜坡。A,這個橫截麵穿過鼻腔,眼眶,上頜竇和篩竇。篩竇位於蝶竇的前麵。中鼻甲和下鼻甲被保留。B,蝶竇前壁被打開,露出多間隔竇和鞍前壁。左鼻甲被切除了。左上頜竇後壁的一部分已經被切除以暴露出齶大動脈它起源於翼齶窩的上頜動脈。頸內動脈在蝶竇外側壁形成蜿蜒的突起。C,切除蝶竇的粘膜和骨壁以暴露頸內動脈,它們形成了上斜坡經鼻暴露的外側界限。 The pituitary gland has been exposed. Additional posterior wall of the left maxillary sinus has been removed to expose the infratemporal fossa, which contains the branches of the maxillary artery, the pterygoid muscles, pterygoid venous plexus, and branches of the mandibular nerve. The nasopharyngeal mucosa covering the longus capitis and the lower clivus is exposed in the interval between the palate and the vomer. D, enlarged view of the sphenoid sinus and sellar region. The anterior surface of the upper clivus is exposed below the pituitary gland. The lateral clival exposure is limited at this level by the internal carotid arteries. E, oblique view. The medial wall of the left cavernous sinus has been opened to expose the abducens and oculomotor nerves. The pterygopalatine fossa is located below the orbital apex. The maxillary nerve passes through the foramen rotundum and gives rise to the communicating rami to the pterygopalatine ganglion and the infraorbital nerve that courses along the floor of the orbit. F, enlarged view of the structures in the medial cavernous sinus. The ophthalmic artery courses below the optic nerve in the optic canal. A., artery; Car., carotid; Cav., cavernous; CN, cranial nerve; Gl., gland; Gr., greater; Inf., inferior; Infratemp., infratemporal; Max., maxillary; Mid., middle; Ophth., ophthalmic; Palat., palatine; Pterygopal., pterygopalatine; Sphen., sphenoid; Turb., turbinates.
垂直中線切口用於位於椎管上部和枕骨大孔水平的後外側或後外側的病變(圖6.3、6.6和6.8)。垂直中線皮膚切口有足夠的長度來完成枕骨大孔上方的顱骨切除術和椎板軸和寰椎切除術。皮下組織從齒輪附近的底層筋膜分離,以獲得y形肌肉切口的空間。“Y”的上肢開始於頸上線水平,枕骨外隆突外側,並連接幾厘米以下的小股,留下一個肌筋膜瓣沿頸上線關閉。Y型切口的下肢在中線向下延伸。主要的顱外危險是椎動脈沿寰椎後弓外側行進時的損傷。如果切口嚴格位於中線,則不會遇到這條動脈,但如果肌肉切口向外側偏離,或當肌肉從寰椎後弓外側剝離時,常在枕下三角底部遇到這條動脈。如果打開使者靜脈和椎靜脈叢,應迅速清除。
如果病變向頸靜脈孔或橋小腦角的前方或前外側延伸,則選擇曲棍球棒切口。皮膚切口從乳突沿頸上線延伸至小齒輪,並在中線向下延伸。沿著上頸線留下一個肌肉袖帶,以方便閉合。該切口可切除枕骨大孔的全部後緣、寰椎和椎軸的後部部分,此外,還可完成足夠大的單側枕下顱骨切除術,以暴露腦幹的前外側表麵和橋小腦角的神經。
在使用中線或曲棍球棒入路打開硬腦膜時,會遇到邊緣竇和枕竇,以及從神經表麵到這些和乙狀結腸竇的橋靜脈。後硬膜內病變很容易從腦和脊髓表麵分離。另一方麵,它們可以附著在神經根和脊髓上,也可以向上延伸穿過小腦髓裂,連接到下髓膜、脈絡膜叢或第四腦室底部。打開脈絡膜和下髓膜可促進該區域腫瘤的暴露。異食癖在扁桃體周圍和扁桃體上極與下髓膜和脈絡膜之間的間隙內運動時,應注意避免損傷異食癖。
側位腫瘤可附著於椎動脈的硬膜內起始段和動脈周圍的厚硬膜袖帶,其中還包括脊膜後動脈和脊髓後動脈、Cl神經根、副神經和齒狀韌帶。遠外側入路可促進這些病變的處理,該入路擴展到包括寰枕關節、硬膜外椎動脈和C1橫突的暴露,並結合枕髁的鑽孔,如遠外側入路章節(29,33)中詳細描述的那樣。分割齒狀韌帶上三角突的附屬物可能有助於暴露前麵的病變。沿延髓外側表麵向上暴露時遇到的結構包括異食癖神經、舌咽神經、迷走神經、副神經和舌下神經。椎動脈可通過曲棍球棒暴露向上追蹤至其與基底動脈的交界處。最難切除的病變是位於舌咽部、迷走神經、副神經和椎動脈外側髓段前的病變。在犧牲這些神經的任何細根之前,應該嚐試輕輕地分離細根,並通過細根之間的間隔進行手術。通常,腫瘤會擴張並擴大小根之間的間隔,從而為中間位置的病變提供一些通路。另一條可能更容易到達延髓和腦橋前麵的病變的路徑是前庭耳蝸神經和麵神經下緣和舌咽神經上緣之間的間隔。在迷走神經小根之間工作是不常見的; however, the lower cervical rootlets of the accessory nerve are very fine and are often separated by a wide interval. Consideration might be given to sacrificing a few of the lower accessory rootlets if it will make an otherwise incurable lesion curable. The intracapsular contents of the tumor are removed, and the remaining tumor capsule is separated from the surface of the brainstem and nerves rather than attempting to deliver the whole intact tumor through the limited exposure. Extreme care should be used when cutting into tumors situated anterolateral to the brainstem, since these tumors, especially meningiomas, may encase a segment of the vertebral artery or the PICA. The dura mater is closed with a dural substitute if closure of the patient’s dura mater constricts the cerebellar tonsils or the cervicomedullary junction. A pseudomeningocele may form at the operative site if there is any tendency toward the development of hydrocephalus. Spinal drainage, repeated spinal punctures, or a shunting procedure may be required to decompress a postoperative pseudomeningocele.
前路首先用於到達脊髓前方的病變,隨後用於暴露腦幹前方的病變(圖6.4、6.5和6.9-6.11)。前入路最大的優點是直達病灶,主要的缺點是經前入路暴露硬膜內病灶後,汙染野和腦脊液瘺、假脊膜膨出、腦膜炎發生率高。手術視野的深度曾經被認為是一個缺點,但是手術顯微鏡的使用降低了這個因素的重要性。
前路已用於到達寰椎、中軸和斜坡的腫瘤;用於韌帶和骨損傷後齒狀突的切除和固定;用於減壓顱頸交界處的骨性畸形,如顱底凹陷,從前方壓迫髓質或脊髓;以及接近基底動脈下部三分之一,椎基底交界處和椎動脈上部的動脈瘤。
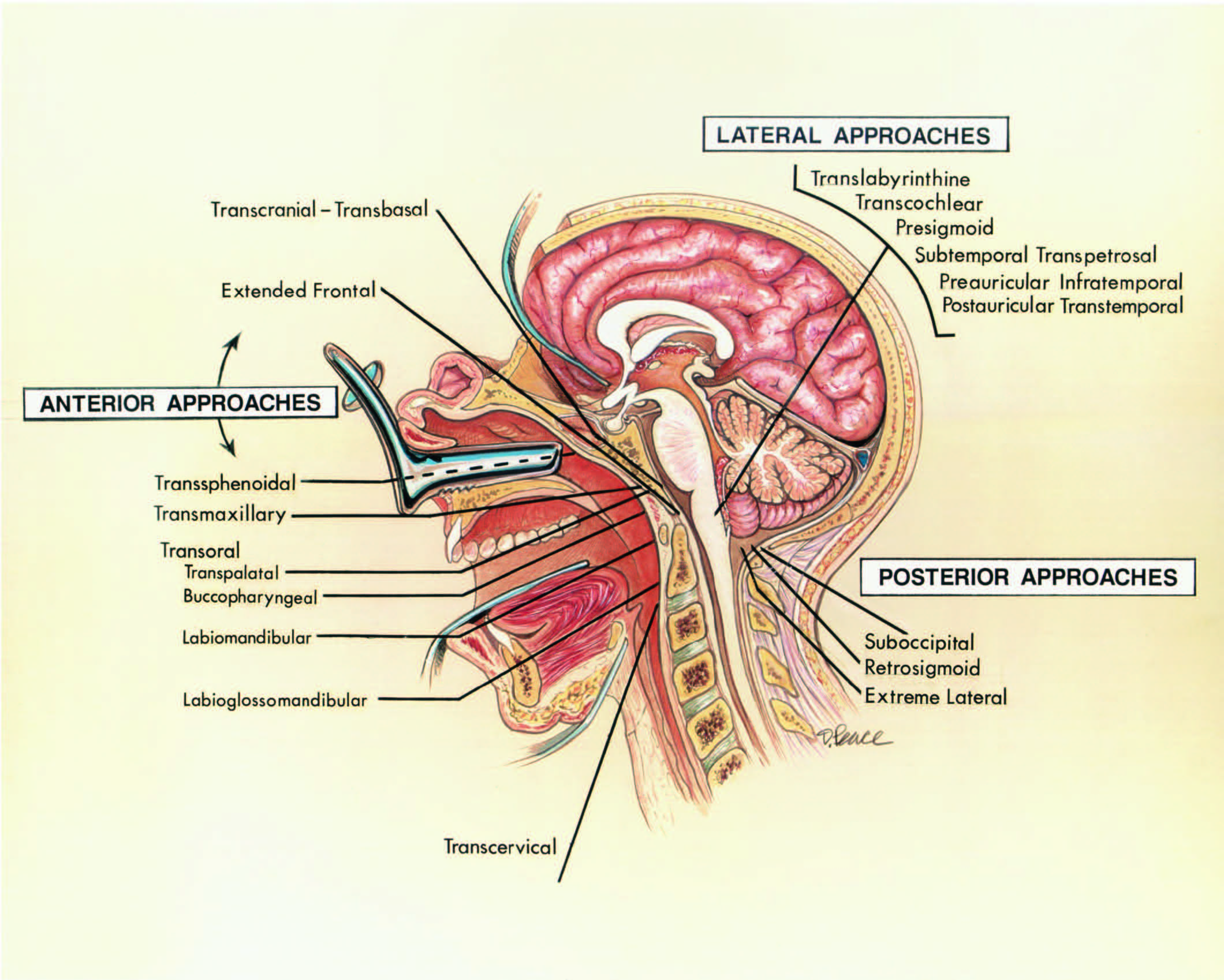
經口途徑通過口和咽後壁,稱為口咽入路,是最常選擇的前入路。基本的經口入路可以修改為包括打開軟齶或軟齶和硬齶的齶入路,以及唇頜或唇舌下頜入路,其中唇、下頜骨,可能還有舌頭和口腔底部被分開以增加暴露。其他類型的前入路有:經頸入路沿著胸鎖乳突肌的前邊界穿過下頜下區域(31);經顱-經基底入路,在切除蝶竇和篩竇後,通過雙額開顱術到達斜坡(6);擴大額部入路,其中雙額部開顱術聯合眶緣截骨術;經蝶竇入路在唇下,沿著鼻中隔,通過蝶竇到達斜坡的上部。

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.12。f。經口、經齶和經上頜入路到斜坡和枕骨大孔。A,強行張開嘴可以使斜坡暴露在上顎以下。B,張開嘴前視。從硬齶向後延伸的軟齶會擋住上斜坡的視線。C,在軟齶中線有一個切口。D,剖開軟齶,露出下斜坡粘膜。E,在中線打開咽黏膜,露出頭長肌和大腸長肌,頭長肌向側麵反射。 F,左側頭長肌和大腸長肌橫向反映。 A., artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; Bas., basilar; Cap., capitis; CN, cranial nerve; For., foramen; Gr., greater; Infratemp., infratemporal; Jug., jugular; Long., longus; M., muscle; Max., maxillary; N., nerve; P.I.C.A., posteroinferior cerebellar artery; Sp., spinal; Sphen., sphenoid; Temp., temporal; Vert., vertebral; Vert., vertebral; Zygom., zygomatic.

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.12。G-J。經口、經齶和經上頜入路到斜坡和枕骨大孔。G,下斜坡已被打開,以暴露椎動脈,基底動脈下部,右側異食動脈,左側異食動脈,以及外展神經和舌下神經。H,切除C1前弓以暴露齒狀突。I,脫套骨膜下剝離暴露上頜骨的前麵和前梨狀孔的下部。J,上頜橫截骨術(LeFort I)通過上頜竇延伸至牙尖上方和眶下管下方。

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.12。k - n。經口、經齶和經上頜入路到斜坡和枕骨大孔。K,下上頜骨向下移位了。通過曝光可以看到斜坡窗和椎動脈。L,斜坡開口的放大視圖。M,上頜骨在中線處垂直分裂,兩部分橫向反射,使斜坡開口向上延伸。N,斜坡暴露的放大視圖。右AICA在右外展神經後麵而左AICA在左外展神經前麵。
經口入路,將軟齶收回至寰椎和軸的前部,並在中線縱向切開咽後壁(圖6.4、6.12和6.13)。通過骨膜下剝離術將粘膜和椎前肌抬高為單一的粘膜骨膜層,並向外側縮回。為了暴露斜坡,通常需要在中線切開軟齶。如果需要增加顱骨暴露,可從硬齶下表麵抬高側基粘骨膜瓣,並可切除硬齶後部。覆蓋在硬齶上表麵的黏膜要縮回,不要打開。這使得咽切口可以通過鼻咽穹窿向上延伸到犁骨的後緣。當從斜坡抬高粘液骨膜層時,側緣向背側傾斜成“溝槽狀”凹陷,其中組織變得更厚,更粘附。根據病變情況,斜坡、寰椎前弓、齒狀突和C2和C3椎體可以用鑽頭和咬骨鉗切除。枕骨髁之間的斜坡暴露為2- 2.5 cm寬,2.5- 3.0 cm長。必須注意避免第六通過12個顱神經,頸內動脈,頸內靜脈,和岩石下鼻竇,這些都是在暴露的外圍。 The most common lesions approached by this route are in an extradural location. Opening the dura mater will expose both vertebral arteries and the lower part of the basilar artery.
為了增加暴露和減少手術深度,可以垂直切開嘴唇和下巴,並在去除中切牙後在中線完成步進式下頜骨截骨術。在不分裂舌頭的情況下,向外側展開下頜骨邊緣,允許舌頭在下頜骨兩半之間向下壓抑。如果暴露仍然不足,舌頭和口腔底部可能在中線裂開。展開下頜骨-舌部,將咽壁暴露到杓狀軟骨的水平。在處理病灶後,重新接近舌和口底的粘膜和肌肉組織,用金屬絲重新定位下頜骨截骨,並仔細閉合嘴唇、下巴和下頜下區域。
圖6.13。經口入路是最常用的前路入路。經口入路的變體包括經齶入路,其中軟齶或軟齶和硬齶都打開,唇頜或唇舌下頜入路,其中嘴唇、下巴、下頜骨,可能還有舌頭和口腔底部在中線分開,以增加暴露。經口入路及其變體允許切除斜坡、寰椎前弓、齒狀突以及C2和C3椎體。A,經口入路。患者頭部固定,以便進行側位x線或圖像強化檢查以確認位置。通常進行氣管造口術。導管通過鼻道插入並置於軟齶後麵並從口腔中取出或通過小舌底部的絲狀縫線連接到鼻導管可以用來收回軟齶。咽後壁在中線縱切(斷線)。B,粘膜和肌肉作為單層向外側縮回,使用骨膜下剝離到達寰椎、軸和下斜坡。 The anterior arch of the atlas, the odontoid process, and the body of the atlas may be removed (interrupted line) to expose the dura. C, it may be necessary to split the soft palate in the midline to expose the clivus (palatal incision, continuous line; pharyngeal incision, interrupted line). D, the anterior surface of the clivus has been exposed through the transpalatal approach. The anterior arch of the atlas and the odontoid process may be removed and an opening made in the clivus (interrupted line). E, if further craniad exposure is needed, laterally based mucoperiosteal flaps may be elevated from the lower surface of the hard palate (interrupted line), and the soft palate split in the midline (continuous line). The posterior part of the hard palate may be removed (oblique lines). F, care is taken to retract rather than open the mucosa lining the upper surface of the hard palate. The pharyngeal incision is extended upward through the vault of the nasopharynx to the posterior border of the vomer. When elevating the mucoperiosteal layer from the clivus, the lateral margins slope dorsally into gutter-like depressions where the tissue becomes more adherent. The clivus, anterior arch of the atlas, dens, and bodies of C2 and C3 may be removed. The clival defect is packed with muscle or fat and may be reinforced with a bone graft. The prevertebral muscle and mucosal layers and the palatal openings are closed with absorbable sutures. G, the lower lip and mandible may be split (interrupted line) to increase the exposure and reduce the operative depth. H, a step-like mandibular osteotomy (interrupted line) is accomplished in the midline after removal of a central incisor tooth. I, spreading the mandibular halves laterally without splitting the tongue permits the tongue to be depressed downward between the mandibular halves. J, if the exposure is still inadequate, the tongue and floor of the mouth may be split in the midline. Spreading the mandibular-lingual halves exposes the pharynx down to the C3 level. The mucosa and musculature of the tongue and floor of the mouth are reapproximated; the mandibular osteotomy is closed with plates; and the lip, chin, and submandibular region are carefully closed after dealing with the lesion. (From, Rhoton AL Jr, de Oliveira E: Anatomical basis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction. New York, Thieme, 1998, pp 13–57 [26].)

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.14。模擬。下頜切開術到斜坡和枕骨大孔。A,入路可通過口腔內的脫手套切口進行;然而,在這種情況下,為了更充分地顯示解剖結構,使用Weber-Fergusson鼻旁切口和眶下延伸術來暴露上頜骨的前麵。眶下神經已分裂,但通常可通過脫手套切口保留。咬肌沿著顴骨的下緣附著。B,上頜竇的粘膜內襯暴露在顴弓下方。去除下頜骨冠突或與顳肌反射,暴露翼肌內側和外側肌以及顳下窩的上頜動脈。C,翼外肌和一段上頜動脈已經被切除。 Removal of the lateral pterygoid exposes the mandibular nerve and its branches in the medial part of the infratemporal fossa. D, a lower maxillectomy has been completed. In this approach, the maxilla can be folded on a vascularized pedicle of soft palate into the floor of the mouth. The pterygoid process, which forms the posterior wall of the pterygopalatine fossa, has been preserved. The nasal mucosa remains intact. The maxillary artery exits the infratemporal fossa to enter the pterygopalatine fossa. A., artery; A.I.C.A., anteroinferior cerebellar artery; Alv., alveolar; Ant., anterior; Bas., basilar; Cap., capitis; Car., carotid; Cav., cavernous; CN, cranial nerve; Eust., eustachian; Gl., gland; Inf., inferior; Infraorb., infraorbital; Int., internal; Intercav., intercavernous; Lat., lateral; Long., longus; M., muscle; Max., maxillary; Med., medial; N., nerve; Pal., palatini; Pet., petrous; Pteryg., pterygoid; Pterygopal., pterygopalatine; Tens., tensor; TM., temporomandibular; Vert., vertebral.

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.14。情況。下頜切開術到斜坡和枕骨大孔。E,鼻黏膜已打開,咽後壁向另一側反射。頭長肌附件已與斜坡分離。F,頭長肌和大腸長肌向外側反射,暴露寰椎前弓、齒狀突和軸體。G,斜坡和硬腦膜已被打開以暴露髓質和椎動脈。H,通過切除蝶竇和蝶鞍前壁,暴露向上延伸。岩狀頸動脈的末端限製了斜坡水平的側暴露,海綿狀頸動脈限製了蝶竇水平的側暴露。海綿間竇連接成對的海綿竇。
經上頜入路被提倡用於病理延伸至斜坡的上三分之一和中三分之一,這是經口入路難以達到的(圖6.12和6.14-6.16)。四種不同類型的經上頜入路已被使用(2,3)。其中一種入路完成LeFort I截骨術,上頜骨和硬齶向下骨折進入口腔。在第二種方法中,稱為擴展上頜切除術,LeFort截骨術與軟齶和硬齶的中線切口相結合,並將上頜骨的一半側向擺動。在第三種入路中,單側下頜骨次全切開術、一半上頜骨和硬齶鉸接在軟齶上並向下折疊到口腔底部(6)。內側頜骨切開術是第四種不太廣泛的入路,允許斜坡暴露。它包括移除上頜前壁的內側部分和前梨狀孔附近的上頜部分(圖6.15)。這提供了一個通過鼻竇和鼻腔相鄰部分的開口,暴露出硬齶上方的斜坡。在手術結束時可以重建鼻竇壁和梨狀前孔。通常可通過脫手套切口進行,但如果需要將入路延伸至內側眶,則可使用側鼻切開術切口(11,12)。
第一種入路采用LeFort截骨術,抬高上唇,沿上牙槽邊緣開粘膜切口,沿兩側磨牙周圍延伸(圖6.16)。剝離上頜骨前部眶下孔下方的黏膜。鋸切延伸到眶下孔下方的上頜竇,高度足以避開牙根,延伸到鼻腔,而上頜內動脈分支和上頜骨和上顎的神經完好無損。上頜骨鼻表麵的粘膜被剝離,鼻中隔在其與上顎的連接上方被分割。遊離骨塊包括位於眶下孔下方的上頜骨和上頜牙部分,其完整的血液和神經供應進入顳下窩和翼狀板區域。軟齶完好無損的事實減少了言語和吞咽障礙的發生率。然而,完整的上頜塊阻礙了通往顱脊交界處的通道,盡管它提供了通往斜坡上三分之一和中三分之一的合理通道。為了增加進入顱椎骨連接處的機會,LeFort截骨術與硬齶和軟齶的中線切口相結合,從而允許上頜半部分及其附著物向外側反映(3)。該手術的缺點是難以獲得良好的咬合和硬齶和軟齶的正常功能。
在下頜骨次全切開術中,位於眶底和眶下管下方的一半上頜骨部分,在血管化組織的鉸鏈上折疊到口腔底部,包括上頜內動脈,並保留軟齶完整(圖6.14)(2,11)。硬齶在中線被分割,小心地保留軟齶。這打開了一條通過鼻腔和口腔到達斜坡、枕骨大孔和上頸部區域的通道。
在每一種入路中,鼻中隔和鼻甲的後部可能被切除,以暴露咽後壁,並提供斜坡和上頸椎的通道。這些入路還可進入蝶竇、篩竇和蝶鞍,以及前窩底內側。鼻中隔兩側粘膜後部可準備皮瓣,可折疊入斜坡缺損以閉合。此外,計劃將允許顳肌移植物折疊到斜坡缺損處進行閉合。在軟齶被分割的手術中,吞咽和語言困難的發生率明顯高於完好無損的手術。在每一種方法中,在進行骨切割之前都要放置鋼板和螺釘,以在手術後實現滿意的咬合。單側下上頜切開術提供了更快速的口齶功能恢複,因為隻有一半的上頜骨受到幹擾,軟齶保持完整。該入路斜坡略斜,但可提供與雙側上頜切開術一樣寬的暴露。

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.15。內側上頜切開術進入斜坡和枕骨大孔。A,側鼻切開術切口沿眶內緣延伸。內側眥韌帶暴露在外。B,內側眥韌帶已經被分割以暴露眼窩的內側。如果不需要暴露眼窩,可以保留韌帶,眼眶內側壁保持完整。梨狀前孔暴露在外。C,截骨術如圖所示,以打開鼻腔和內側上頜骨。內側骨打開鼻腔,外側骨取出暴露上頜竇。內側上頜切開術有助於顯露斜坡。 D, the exposure has been directed to the posterior nasopharyngeal wall behind which the clivus sits. The anterior wall of the sphenoid sinus has been removed, exposing the sphenoid septum. The posterior part of the nasal septum has been removed to expose the clivus below the sphenoid sinus. Removal of the medial part of the posterior wall of the maxillary sinus exposes the maxillary artery in the pterygopalatine fossa. E, enlarged view of the pterygopalatine fossa exposed by removing the medial part of the posterior wall of the maxillary sinus. The maxillary nerve and artery enter the pterygopalatine fossa. The maxillary artery is the major source of bleeding during surgery in this area. The maxillary artery enters the pterygopalatine fossa by passing through the pterygomaxillary fissure. The maxillary nerve enters the fossa by passing through the foramen rotundum and gives off communicating rami to the pterygopalatine ganglion. F, the pharyngeal mucosa has been opened, the longus capitis reflected laterally, and the clivus and dura opened to expose the basilar artery ascending in front of the pons. The pituitary gland is at the upper margin of the exposure. A., artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; Bas., basilar; Cap., capitis; CN, cranial nerve; Eust., eustachian; Gang., ganglion; Gl., gland; Gr., greater; Lig., ligament; Long., longus; M., muscle; Max., maxillary; Med., medial; N., nerve; Nasolac., nasolacrimal; Post., posterior; Pterygopal., pterygopalatine; Sphen., sphenoid; Vert., vertebral.
圖6.16。Transmaxillary方法。示出三種經上頜入路。這三種手術都可以通過口腔內切口脫手套完成。另一種類型的切口延伸到麵部,如Weber-Fergusson切口,可以考慮。A,抬高上唇,沿著臼齒周圍的上牙槽邊緣切開黏膜。粘膜從上頜骨的前側麵抬升到眶下孔以下,但要高到足以避開牙根。黏膜從上頜骨的鼻表麵抬高,鼻中隔在其與上顎的附著處上方分開。B,鋸切(實線)延伸至兩側上頜竇。上頜骨的遊離塊向下移動(箭頭),以便進入斜坡。 C, the intraoral retractor has been placed. Displacing the maxilla downward gives wide access to the clivus. D, a modified technique, called the extended maxillectomy, includes the LeForte I osteotomy with a midline incision of the hard and soft palate (solid lines). E, this allows the halves of the maxilla, which are attached to the muscles and vessels in the infratemporal fossa, to be reflected laterally, providing wider exposure to the clivus and upper cervical spine. F, retractors have been placed to expose the clivus and upper cervical area. The approach can be extended upward into the sphenoid and ethmoid sinuses and downward to C2 or C3. G–I. Unilateral maxillotomy. G, in this approach, half of the maxilla is mobilized by a bone cut, which extends back to the infratemporal fossa in the area just below the infraorbital foramen, and the maxilla is divided in the midline. A mucosal incision is made along the low surface of the hard palate parallel to the midline on the side opposite the saw cut through the hard palate, and the anterior face of the maxilla is degloved on one side. The soft palate is left intact. H, the unilateral block of maxilla, which is still attached to the structures in the infratemporal fossa along the pterygoid plates and to the soft palate, which is not interrupted, is folded downward into the floor of the mouth. I, the anterior part of the nasal septum is left undisturbed, but the posterior part is removed along with some of the turbinates and wall of the sinuses to provide a wide exposure of the clivus. This exposure can be enlarged to include the walls of the sphenoid and ethmoid sinuses. (From, Rhoton AL Jr: Anatomical basis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].)

圖6.17。蝶竇入路。左上,這個入路在上唇下方,沿著鼻中隔,穿過蝶竇,可以用來暴露斜坡的上三分之一。可切除區域(斜線)包括蝶鞍底和前壁、犁骨和斜坡的上三分之一。這種方法適用於一些從枕骨大孔向上延伸的腫瘤的活檢。右下,杯鉗檢查斜坡腫瘤。B,通過鼻窺鏡觀察。鼻前棘被保留,鼻中隔軟骨的前部仍然附著在一側的鼻中隔粘膜上。鼻鏡插入鼻中隔左側和鼻中隔粘膜之間。鼻中隔和鼻中隔右側的黏膜被窺鏡推到右側,鼻中隔左側的黏膜被推到左側。 The keel on the vomer is exposed. C, magnified view. The vomer has been removed to open the sphenoid sinus. The sellar floor is above the midline septum. In approaching the clivus, the floor of the sella is removed, and the opening in the bone is extended downward on the clivus (interrupted lines) to the inferior margin of the sphenoid sinus.
圖6.18。A,經頸入路。氣管切開術可以使下顎緊緊閉合。t型皮膚切口(間斷線)包括從乳突尖端延伸至 門蒂聯合的下頜下切口和向下延伸至胸鎖乳突肌的下延伸。B,可切除區域(斜線)包括斜坡、軸的前弓、軸的齒狀突體。C, 暴露指向胸鎖乳突肌的前邊界和外側 內頸動脈和頸內靜脈之間,以及內側的食管、下咽和氣管。可以劃分為增加暴露的結構包括咽升動脈和甲狀腺上動脈,喉外神經,舌下神經,喉內神經,舌動脈,舌下神經,莖突舌骨肌,二腹肌前腹,莖突舌骨韌帶,舌咽神經,莖突咽肌和莖突舌骨肌。副神經在胸鎖乳突肌後麵。D,椎前筋膜、頭長肌和頸長肌在斜坡到C3的中線分離,並使用骨膜下剝離術向外側縮回,露出斜坡、寰椎和軸的腹側。E和F,寰椎前弓和齒狀突,以及從枕骨大孔延伸至蝶枕軟骨聯合的2.5 mm寬斜坡可被切除。 The basilar, vertebral, and anterior spinal arteries are exposed in the dural opening. After dealing with the pathology, the dura is closed, muscle and fat are placed in the clival window, and the prevertebral and fascia are sutured in the midline. (From, Rhoton AL Jr: Anatomical basis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].) A., artery; Ant., anterior; Bas., basilar; Car., carotid; Ext., external; Inf., inferior; Int., internal; Jug., jugular; M., muscle; Sp., spinal; Sup., superior; V., vein; Vert., vertebral.

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.19。f。經基底和額葉延伸入路的關係。A,雙冠狀頭皮皮瓣向前反射。顱骨周圍膜通常被反射為一個單獨的層,以便以後用於閉合顱前窩底。B、骨瓣和截骨術。經顱-經基底入路僅使用前顱窩底部的雙額開顱術,不進行截骨手術。完成了雙額大開顱術和額眶顴截骨術。截骨部分可延伸至鼻骨和外側眶緣,但對於大多數斜坡病變,更有限的骨瓣和截骨(虛線)通常就足夠了,可以根據需要進行定製,以處理涉及鼻腔、鼻竇或眼眶的情況。C,眶周與眶壁分離,準備進行截骨手術。 Division of the medial canthal ligament is not necessary for most lesions, but may be required for lesions extending into the lower nasal cavity or orbit. The ligaments should be re-approximated at the end of the procedure. D, the right medial canthal ligament has been divided and the orbital contents retracted laterally to expose the nasolacrimal duct and the anterior ethmoidal branch of the ophthalmic artery at the anterior ethmoidal foramen. E, the osteotomies have been completed and the frontal dura elevated. The dura remains attached at the cribriform plate. The upper part of both orbits are exposed. F, an osteotomy around the cribriform plate leaves it attached to the dura and olfactory bulbs, a maneuver that has been attempted to preserve olfaction, but is infrequently successful. The anterior face of the sphenoid sinus and both sphenoid ostia are exposed between the orbits. A., artery; A.C.A., anterior cerebellar artery; A.I.C.A., anteroinferior cerebellar artery; Ant., anterior; Bas., basilar; Car., carotid; CN, cranial nerve; Ethm., ethmoidal; Gl., gland; Lam., lamina; Lig., ligament; M.C.A., middle cerebral artery; Med., medial; Nasolac., nasolacrimal; Pit., pituitary; Sphen., sphenoid; Sphenopal., sphenopalatine; Sup., superior; Term., terminalis; Turb., turbinates; Vert., vertebral.

點擊這裏查看此圖像的交互模塊和相關內容。
圖6.19。G-L。經基底和額葉延伸入路的關係。G,打開蝶竇暴露出蝶竇內的隔膜。蝶齶動脈穿過蝶骨的前麵。H,蝶竇內的間隔,鞍底和側竇壁已被切除,以暴露海綿狀頸動脈,腦下垂體和視神經管。斜坡被打開,暴露腦幹對麵的硬腦膜。基底竇與海綿竇後部相連,位於上斜坡硬腦膜層之間。J,斜坡已打開,暴露彎曲的椎動脈,它們在斜坡開口左側外側緣連接形成基底動脈。這兩個美洲國家的起源都暴露了。 A vein splits the right abducens nerve into two bundles adjacent to the brainstem. K, the frontal dura has been opened and the frontal lobes elevated to expose the olfactory and optic nerves, the internal carotid, and the anterior and middle cerebral arteries. L, enlarged view. The subfrontal and clival openings are separated by the sella and pituitary gland. The lateral limit of the clival exposure is defined by the internal carotid arteries and optic nerves. The lamina terminalis is exposed above the optic chiasm.
![圖6.20。A,如果腫瘤還涉及並需要切除部分篩骨和蝶骨(斜線),則可采用經顱-經基底入路接近枕骨大孔前緣的腫瘤。B,插入。下顎頭皮切口位於發際線後,雙額開顱術(間斷線)嚴格置於眶上,不考慮額竇(斜線)。右下方。額下硬腦膜與眶頂分離,硬膜外剝離至蝶骨小翼、鞍結節和前楔突基部。在切除前顱窩底的後部、篩竇和蝶竇壁的上部以及鞍底後到達斜坡。繼續向下,切除斜坡,打開枕骨大孔的前緣。從脊柱前部分離咽黏膜,暴露寰椎前弓,甚至C2和C3椎體的前部。不應打開鼻咽黏膜。 Dural defects are closed with a leak-proof dural graft after dealing with the lesion. C, the orbital roof and the remainder of the cranial base are reconstructed using bone grafts. If the clivus has been removed, the graft above the ethmosphenoidal space is fitted into the edge of a vertical graft extending from the anterior margin of the foramen magnum or the anterior arch of the atlas to the floor of the sella. (From, Rhoton AL Jr: Anatomical basis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].)](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Foramen_magnum_6.20.jpg)
圖6.20。A,如果腫瘤還涉及並需要切除部分篩骨和蝶骨(斜線),則可采用經顱-經基底入路接近枕骨大孔前緣的腫瘤。B,插入。下顎頭皮切口位於發際線後,雙額開顱術(間斷線)嚴格置於眶上,不考慮額竇(斜線)。右下方。額下硬腦膜與眶頂分離,硬膜外剝離至蝶骨小翼、鞍結節和前楔突基部。在切除前顱窩底的後部、篩竇和蝶竇壁的上部以及鞍底後到達斜坡。繼續向下,切除斜坡,打開枕骨大孔的前緣。從脊柱前部分離咽黏膜,暴露寰椎前弓,甚至C2和C3椎體的前部。不應打開鼻咽黏膜。 Dural defects are closed with a leak-proof dural graft after dealing with the lesion. C, the orbital roof and the remainder of the cranial base are reconstructed using bone grafts. If the clivus has been removed, the graft above the ethmosphenoidal space is fitted into the edge of a vertical graft extending from the anterior margin of the foramen magnum or the anterior arch of the atlas to the floor of the sella. (From, Rhoton AL Jr: Anatomical basis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].)
沿鼻中隔經蝶竇入路可暴露斜坡的上三分之一(圖6.9-6.11和6.17)(10)。切除犁肌進入蝶竇,露出蝶鞍底和斜坡的腹側表麵。鼻前棘和鼻中隔軟骨前部被保留。在接近斜坡時,蝶鞍底部可能被切除,骨開口向下延伸至蝶竇下緣。延伸到斜坡上三分之一的病變可通過這種方法進行活檢或部分切除。鞍部和斜坡開口由脂肪或肌肉和鼻中隔軟骨封閉。該方法的優點是並發症發生率低,缺點是手術範圍小,局限於斜坡的上三分之一。
Stevenson等人采用經頸入路,經頸部筋膜平麵至枕骨大孔區域(圖6.18)(31)。它避免打開口咽粘膜,但由於暴露深度和不是直接的中線暴露,很少選擇。氣管造口術可以使下顎緊緊閉合,便於暴露。t型皮膚切口包括從乳突尖端到下頜聯合的下頜下切口和從下頜下切口中點穿過胸鎖乳突肌的下延伸。在咽和椎前肌之間的筋膜平麵是通過沿著胸鎖乳突肌的前邊界和外側頸動脈鞘與食管和氣管之間的暴露到達的。椎前筋膜和肌肉向外側縮回,露出斜坡、寰椎和椎軸的腹側。可由下而上劃分以增加暴露的結構包括咽升動脈和甲狀腺上動脈、喉外神經、舌下神經、喉內神經、舌狀動脈、舌下神經、莖突舌骨肌、二腹肌前腹、莖突舌骨韌帶、舌咽神經、莖突咽肌和莖突舌骨肌。寰椎前弓和齒狀突,以及從枕骨大孔延伸至蝶枕軟骨聯合的2厘米寬斜坡可被切除。側偏可能損傷頸內靜脈、頸內動脈、咽鼓管和第九至第十二腦神經。
![圖6.21。擴大正麵入路。A,左上插入圖顯示頭皮皮瓣和顱骨移除順序(1,2,3)。第三步,眶前篩竇截骨術,包括眶上脊、眶頂前部、額竇、篩板和部分篩竇氣細胞。B,矢狀圖。沿顱底的斜線顯示了骨頭可能被切除的程度。在切除前窩底的後部、篩竇氣細胞、蝶竇壁和斜坡後到達枕骨大孔。C,軌道周圍沿軌道頂部暴露。骨移除已擴展到篩竇空氣細胞和蝶竇。暴露可沿斜坡延伸至枕骨大孔。D,使用顱瓣重建。 A fat graft is placed in the ethmoid and sphenoid sinuses before reflecting the pericranial flap over them. In addition, a fat graft may also be applied to the inner side of the pericranial flap. (From, Rhoton AL Jr: Anatomical basis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].)](https://assets.neurosurgicalatlas.com/neuroanatomy/Rhoton_-_Missed_Images/Foramen_magnum_6.21.jpg)
圖6.21。擴大正麵入路。A,左上插入圖顯示頭皮皮瓣和顱骨移除順序(1,2,3)。第三步,眶前篩竇截骨術,包括眶上脊、眶頂前部、額竇、篩板和部分篩竇氣細胞。B,矢狀圖。沿顱底的斜線顯示了骨頭可能被切除的程度。在切除前窩底的後部、篩竇氣細胞、蝶竇壁和斜坡後到達枕骨大孔。C,軌道周圍沿軌道頂部暴露。骨移除已擴展到篩竇空氣細胞和蝶竇。暴露可沿斜坡延伸至枕骨大孔。D,使用顱瓣重建。 A fat graft is placed in the ethmoid and sphenoid sinuses before reflecting the pericranial flap over them. In addition, a fat graft may also be applied to the inner side of the pericranial flap. (From, Rhoton AL Jr: Anatomical basis of surgical approaches to the region of the foramen magnum, in Dickman CA, Spetzler RF, Sonntag VKH (eds): Surgery of the Craniovertebral Junction. New York, Thieme Medical Publishers, Inc., 1998, pp 13–57 [24].)
如果腫瘤還涉及並需要切除部分篩骨、蝶骨和斜坡,則可采用額下經基底入路接近枕骨大孔前方的腫瘤(圖6.19和6.20)。經基底入路,如Derome(6)所示,是通過位於發際線後的雙冠狀頭皮切口和嚴格位於眶上的雙額遊離骨瓣而不考慮額竇。額下硬腦膜與眶頂分離,嗅覺神經在篩板處分離,硬膜外剝離經後至蝶骨小翼、鞍結節和前楔突基部。人們曾嚐試將嗅球附著在篩板上,但這通常不能防止這些手術後常見的嗅覺喪失。在切除前顱窩底的後部、篩竇和蝶竇壁的上部以及蝶鞍底後到達斜坡。從鞍底向下,切除斜坡,打開枕骨大孔的前緣。從脊柱前部分離咽黏膜允許暴露寰椎前弓,甚至C2和C3椎體。經顱經基底入路不開放鼻咽黏膜,但通常在包括眶上截骨術和雙額瓣的手術中暴露。硬腦膜缺損用一種比缺損大兩倍以上的防漏硬腦膜替代物封閉,將其縫合在暴露部位最遠處的硬腦膜上。眶頂和顱底其餘部分用自體骨移植重建。 If the clivus has been removed, the graft above the ethmosphenoidal space is fitted into the edge of a vertical graft extending from the anterior margin of the foramen magnum or the anterior arch of the atlas to the floor of the sella. The advantages of the transbasal approach are that a tighter closure of the dura mater is possible than can be achieved through the transoral approaches, the subcranial mucosal planes can be preserved, and it can be combined with another intradural approach without the high risk of infection associated with the transoral approaches. The transbasal approach may be combined with a transbasal-transsphenoidal route to gain access to the sella turcica. In the transbasal approach the clivus and sphenoid bone can be resected more extensively than by the transsphenoidal approach, but the subsellar area is hidden by the bulging dura in the transbasal approach. Both approaches may be combined to permit removal of all of the clivus below the level of the dorsum sellae. Anosmia is the only certain side effect. The most frequent complications are cerebrospinal fluid leaks, meningitis, and pseudomeningoceles.
擴大額部入路與經顱-經基底入路相似,不同之處在於它包括眶額篩竇截骨術(圖6.19和6.21)(28)。它也可用於枕骨大孔前部的腫瘤,特別是當腫瘤需要切除部分篩骨和蝶骨以及斜坡時。該方法使用了下顎頭皮切口、雙額骨瓣和眶額篩竇截骨術,其中眶上脊、部分眶頂和可能的上鼻、篩竇頂和篩板一次性切除。病灶切除可采用硬膜外或硬膜內-硬膜外聯合入路。切除前顱窩底的後部、篩竇和蝶竇的上壁以及鞍底後可到達斜坡和枕骨大孔。如果需要,眶上截骨術甚至可以在大小和位置上進行定製,以包括外側眶緣。
斜坡或上頸椎前硬膜外病變最好采用其中一種前入路。經口入路用於大多數涉及枕骨大孔的前硬膜外病變,因為它提供了一個中線暴露,是最直接的病理途徑。對於更廣泛的病變,可考慮經上頜入路。在選擇需要通過口咽打開硬腦膜的前路入路之前,應該考慮選擇後路入路,因為如果通過口咽打開硬腦膜,腦脊液漏、腦膜炎和假性脊膜膨出的發生率很高。經頸入路的優點是通過頸部深筋膜麵到達枕骨大孔,而不是通過口咽;然而,暴露的深度,完成解剖所需的時間長度,以及不從中線接近枕骨大孔的事實阻礙了它的普遍使用。經顱-基底和額部延伸入路為到達枕骨大孔提供了另一種前路,但這些入路不應被考慮用於接近嚴格局限於枕骨大孔區域的腫瘤,而可用於涉及篩竇和蝶竇以及斜坡和枕骨大孔的廣泛病變。經蝶竇入路為枕骨大孔區域的病變活檢提供了一個簡單的途徑,如果病變延伸到斜坡的上三分之一,但它不能提供足夠的暴露來去除該區域較大的病變。經蝶入路可聯合另一入路切除斜坡和枕骨大孔病變。
大多數硬膜內病變首選後路。垂直中線切口,雙側枕下顱骨切除術和上頸椎椎板切除術用於位於椎管上部和枕骨大孔上方後方或後外側的病變。如果病變向頸靜脈孔或橋小腦角前外側或前方延伸,則選擇曲棍球棒切口和單側枕下顱骨切除術和上頸椎椎板切除術。枕下外側入路的遠側修飾,將在下一章遠側入路中描述,為腦幹腹側和枕骨大孔前緣的病變提供了更直接的入路,同時減少了神經結構的回縮(32,33)。枕骨大孔也可以通過顳骨進入,這是顳骨一章的主題;然而,為了到達枕骨大孔和斜坡,這些入路可能需要重新定位頸動脈或麵神經,並可能切除聽覺和前庭迷路。
貢獻者:Albert L. Rhoton, Jr
內容來自Rhoton AL, Jr.後顱窩:顯微外科解剖和手術入路。神經外科2000; 47:1196。doi.org/10.1097/00006123 - 200105000 - 00065.經牛津大學出版社許可,代表神經外科醫生協會。©神經外科醫生協會。
神經外科188bet手机app圖集很榮幸能夠保持Albert L. Rhoton, Jr, MD的遺產。
請登錄發表評論。
請務必在社交媒體上關注我們,獲取令人興奮的內容,並保持更新生活科恩醫生的會議,關於手術技術的問題,以及更多!



您必須登錄才能查看此資料。
的188bet手机app幾乎完全取決於你的捐款。
如果沒有你們的大量捐贈我們無法繼續製作《地圖集》。
請承諾每年至少向Atlas捐贈250美元。如果沒有這種承諾,Atlas將很快需要付費訂閱,世界各地的許多外科醫生將無法使用它,他們的病人的護理依賴於它。
請立即捐款!
如果沒有你們的大量捐贈我們無法繼續製作《地圖集》。請承諾每年至少向Atlas捐贈250美元。
如果沒有這個承諾,Atlas將很快需要付費訂閱世界各地的許多外科醫生都無法使用它,他們的病人的護理都依賴於它。請立即捐款!